When it comes to the treatment of stomach cancer, most people’s first thought is surgery, thinking that surgery is the way to go, and that once the surgery is done and the tumor is removed, they can rest easy. In fact, surgery is indeed an important tool in the treatment of gastric cancer, but it is not the only one.
Gastric cancer cells are like the “bad guys” in the human body, and while surgery can wipe out the “criminal gang” gathered in the stomach, there will always be “fish in the net” and “bad guys” that are scattered around the edges. However, there will always be the “unlawful elements” (residual cancer cells or cancer cells that have entered the human blood or lymphatic system) that are scattered around the edges and roaming outside, which may wait for the opportunity to make waves again and lead to recurrence or metastasis. In order to avoid this, patients with gastric cancer often need post-operative adjuvant chemotherapy to protect them from the first signs of recurrence and metastasis.
What is the purpose of postoperative adjuvant chemotherapy?
As the name implies, postoperative adjuvant chemotherapy is chemotherapy administered after radical gastric cancer surgery, with the aim of eliminating residual cancer cells, suppressing subclinical lesions (i.e., lesions that cannot be detected with clinical examination or the naked eye and exist around or distant from the main tumor lesion), and preventing recurrence and metastasis after surgery, thereby improving the survival rate of gastric cancer.
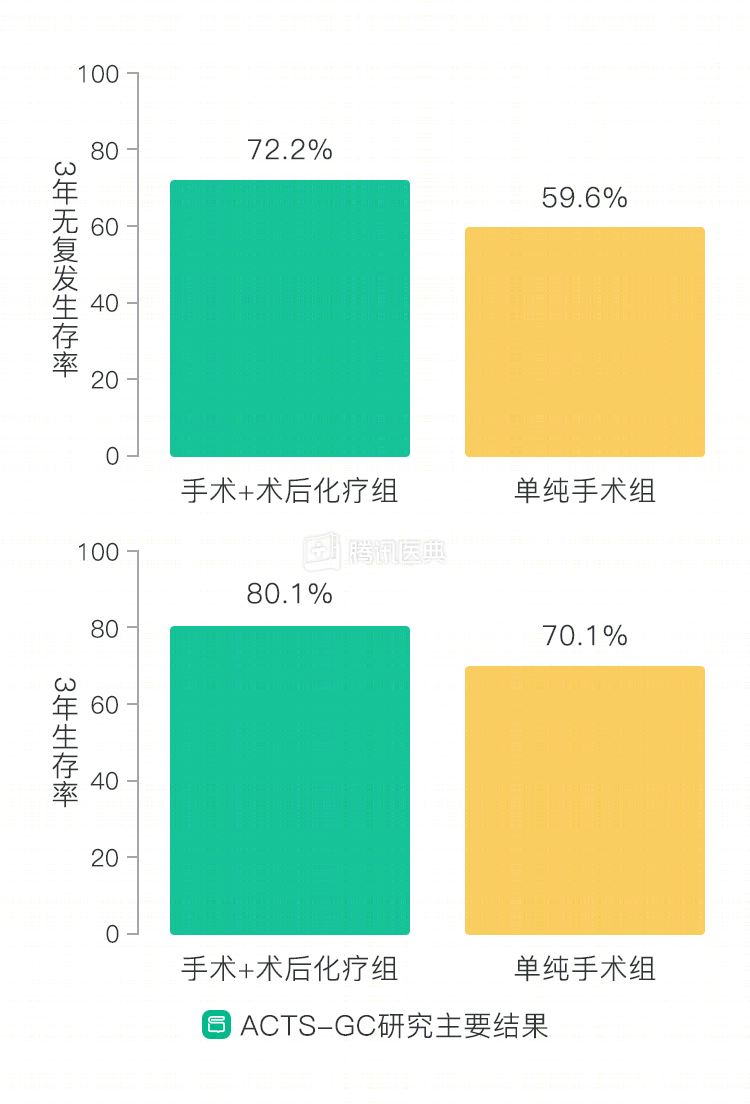
Postoperative adjuvant chemotherapy for gastric cancer began in the 1980s and has undergone a process of optimization from scratch. In the early years, although there were many studies confirming that adjuvant chemotherapy could lead to improved survival, the results were not convincing because of old protocols and insufficient sample size. It was only with the advent of two landmark studies, the ACTS-GC study in 2007 and the CLASSIC study in 2012, that the place of adjuvant chemotherapy in the treatment of gastric cancer was established. Both of these phase III clinical studies in Asian patients confirmed that postoperative adjuvant chemotherapy can reduce the postoperative recurrence rate and prolong the survival of gastric cancer patients. Postoperative adjuvant chemotherapy for gastric cancer has moved from empirical to evidence-based medicine and is now one of the main options chosen by oncologists facing gastric cancer.
Do all patients with gastric cancer after surgery need adjuvant chemotherapy? The answer is no. The need for adjuvant chemotherapy is determined by the TNM stage of the tumor and the presence of high-risk factors.
The following patients will require postoperative adjuvant chemotherapy depending on the tumor
- Early gastric cancer Some patients with early gastric cancer usually have a 5-year survival rate of 90% to 95% after surgery, even without adjuvant chemotherapy, and these patients usually only need regular follow-up reviews. However, early gastric cancer patients with postoperative pathologically confirmed lymph node metastases require postoperative adjuvant chemotherapy; for patients with pathologic residual (R1, cancer cells visible under the microscope at the cut edge of the surgical specimen) and naked eye visible tumor residual (R2) early gastric cancer, postoperative fluorouracil- or paclitaxel-based concurrent radiotherapy is usually required.
- Locally advanced gastric cancer All patients who undergo D2 radical surgery for gastric cancer (i.e., removal of perigastric lymph nodes to station 2) with R0 resection (i.e., no cancer cells found microscopically at the cut edge of the surgical specimen) and who are not treated preoperatively, as long as the depth of infiltration is above T2 (tumor reaching the muscular layer) and/or is accompanied by Patients with T2N0M0 (stage IB) also generally require postoperative adjuvant chemotherapy when they are no older than 50 years, have a histologic grade of high-grade or poorly differentiated, have nerve bundle invasion, vascular infiltration, or have not undergone a standard D2 lymph node dissection.
- Post-neoadjuvant chemotherapy Adjuvant chemotherapy is recommended after radical surgery in patients who have received pre-operative neoadjuvant chemotherapy and who have not completed their chemotherapy program, but the physician will consider how the patient’s physical condition has changed as a result of post-operative GI reconstruction, for example, and adjust the treatment regimen and dose accordingly.
According to medical conditions, chemotherapy should not be received for the following conditions
Patients need to meet certain physical conditions to receive chemotherapy and usually cannot receive chemotherapy when:
- Poor general condition, old and frail, KPS (Karnofsky Performance Status score) not greater than 40 points, severe cardiopulmonary insufficiency, and unable to tolerate chemotherapy;
- Poor bone marrow hematopoiesis, severe anemia, white blood cell count less than 2.5×10/L, neutrophil count less than 1.0×10/L or platelet count less than 50×10/L;
- Severe abnormalities in liver and kidney function;
- Patients who have had multiple courses of chemotherapy, extensive radiotherapy, advanced age, bone marrow metastasis, severe infection, adrenocortical insufficiency, and severe complications should be treated with caution or without chemotherapy;
- Patients with a propensity for perforation of the gastrointestinal tract;
- Patients with psychiatric disorders or those who cannot cooperate adequately;
- Pregnant women, who may first undergo abortion or induction of labor;
- It should be used with caution in allergic patients and is contraindicated in those who are allergic to the chemotherapy drugs used.
The need for postoperative adjuvant chemotherapy requires a comprehensive judgment by the physician based on the stage of the tumor, whether it is accompanied by high-risk factors, and combined with the patient’s physical condition. After gastric cancer surgery, patients need to fully communicate with their doctors, receive scientific and standardized treatment and follow-up, and reasonably combine surgery with adjuvant chemotherapy to minimize the risk of recurrence and metastasis. (Contributed by Yanwen Diao, Department of Gastrointestinal Oncology, The First Hospital of China Medical University)