
With the rapid development of immunotherapy in recent years, many patients may have heard about the “miraculous effects” of immunotherapy, but can it be used for breast cancer patients?
Primarily for triple-negative breast cancer
The efficacy of immunotherapy can be predicted based on tumor infiltrating lymphocytes (TILs), which reflect the level of lymphocytes that accumulate in the area of the tumor lesion. Higher levels mean that immunotherapy is more effective.
The levels of tumor-infiltrating lymphocytes vary by type of breast cancer (Table 1) and are highest in triple-negative breast cancer; therefore, immunotherapy is primarily used for triple-negative breast cancer.
Table 1 Levels of tumor-infiltrating lymphocytes in different types of breast cancer

Note: The full name of HER-2 is human epidermal growth factor receptor-2; TILs are tumor-infiltrating lymphocytes.
What are the available immunotherapies for patients with triple-negative breast cancer?
Immune checkpoint inhibitors
Only the immune checkpoint inhibitor PD-L1 monoclonal antibody, Atezolizumab (trade name: Tecentriq), is currently approved for marketing by the FDA
PD-L1, whose Chinese name is “programmed death receptor ligand-1”, is found on the surface of tumor cells and binds to PD-1 (programmed death receptor-1) on the surface of T cells, inhibiting the immune system’s ability to kill tumors. The PD-1/PD-L1 inhibitor, however, prevents tumor cells from binding to T cells, releasing the “brakes” on immune suppression and restoring the body’s normal immunity to tumors (Figure).

How does it work?
In a study published this year, Atezolizumab in combination with chemotherapy as first-line treatment (initial therapy) for advanced triple-negative breast cancer not only resulted in longer median progression-free survival (PFS) (7.2 months vs. 5.5 months) compared with chemotherapy alone, but also reduced the risk of death by 38%.
Where median progression-free survival is the data for patients who ranked right in terms of time to maintain stable tumors after treatment; similarly, median overall survival is the data for patients who ranked right in terms of overall survival time, which is a point estimate. And a reduction in the risk of death not only means a prolongation of median overall survival, but also represents an improvement on one face, an overall difference between the treatment and control groups.
In terms of efficacy, this is a very impressive improvement. And because of this result, the FDA approved Atezolizumab in combination with chemotherapy (albumin paclitaxel) in triple-negative breast cancer.
In addition to Atezolizumab, several other PD-1/PD-L1 monoclonal antibodies – Avelumab (trade name: Bavencio), and pabrolizumab (trade name: Corydal) – have also been shown to be effective in advanced triple-negative breast cancer in studies, but the number of patients in most trials The number of patients in most of the trials is small and the efficacy needs to be further verified. We compare them all in the table below.
Table 2 PD-1/PD-L1 monoclonal antibody in advanced triple-negative breast cancer
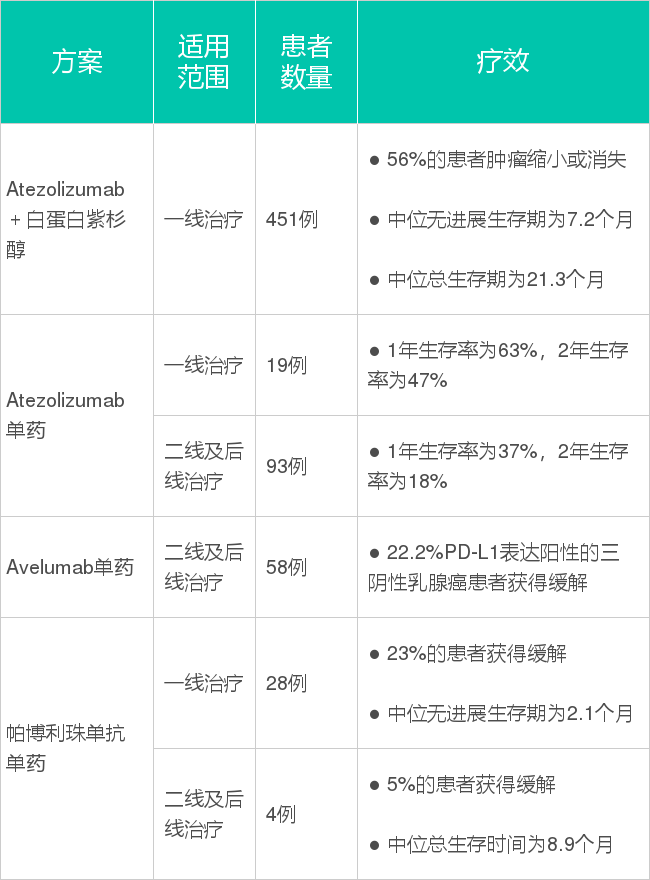
From the data in the table above, it is clear that as first-line therapy, Atezolizumab in combination with chemotherapy has the best efficacy. With Atezolizumab alone, the efficacy was much less than with the combination regimen. Currently, Atezolizumab, Avelumab, and pabrolizumab alone, have all shown to be effective in backline therapy, and it remains to be clarified by research as to who is best.
Other immunotherapies
One such case was published in 2018 in the top medical journal nature medicine.
A 49-year-old patient with triple-negative breast cancer had cancer that had metastasized from her right breast to her liver, bones, and other parts of her body after multiple failed chemotherapy treatments. However, treatment with CAT-T in combination with pablizumab cleared all the cancer cells from the body and achieved a cure.
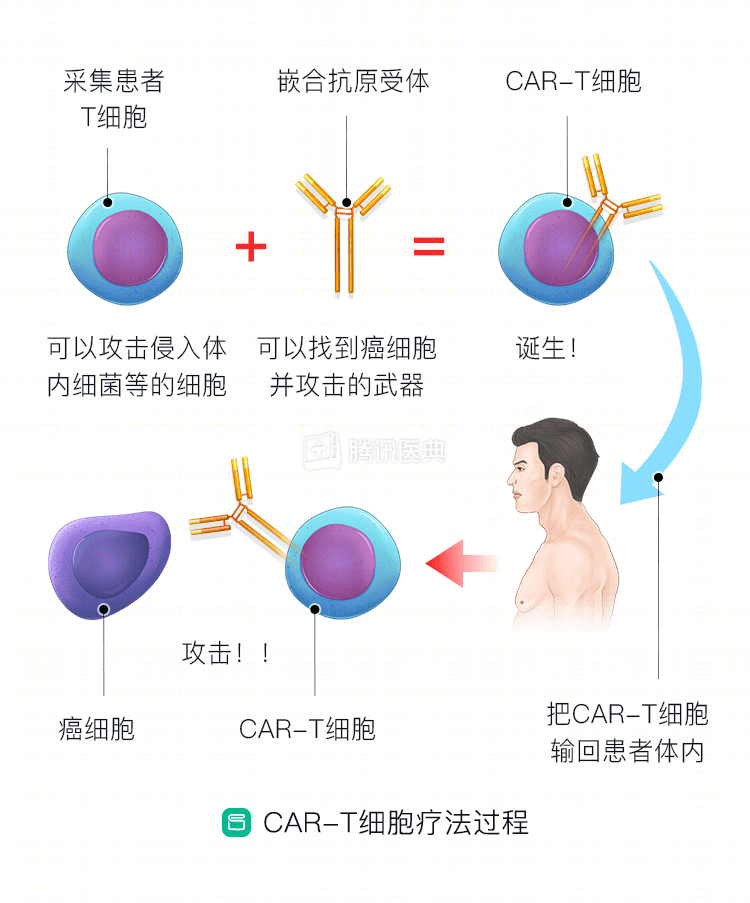
In addition to pablizumab, the patient was treated with CAR-T, a cellular immunotherapy treatment called chimeric antigen receptor T-cell therapy.
The first step is to collect enough T cells from the patient’s blood and send them to the lab to be “processed” so that they can better recognize and kill tumor cells. The T cells are then transfused back into the body for the purpose of treatment (Figure).
But this is an isolated case, and it cannot be assumed that the treatment will work for all patients with triple-negative breast cancer. Early data from one study showing six patients with triple-negative breast cancer treated with CAR-T, four of whom were treated effectively but three had cytokine-releasing syndrome (CRS), is now being studied.
Cytokine release syndrome is one of the more serious adverse effects that can occur with CAR-T therapy. This is because when CAR-T cells kill cancer cells, they cause a large release of cytokines to activate more immune cells to work together to fight the target. However, at the same time, the large amount of cytokines can launch a surprising attack on other tissues and organs, leading to high fever, low blood pressure, shock, and even death.
Despite cases of cure, CAR-T cell therapy for breast cancer is still in preclinical trials and clinical trials, and is still some distance away from true clinical use.