Surgery is one of the most important treatments for gastric cancer, and there are many surgical options. Many patients with stomach cancer wonder why others have only part of their stomach removed while they have all of it removed, and what the difference is.
The main types of surgery to remove gastric cancer include distal major gastrectomy, proximal major gastrectomy, and total gastrectomy, depending on where it is removed.
Different patients
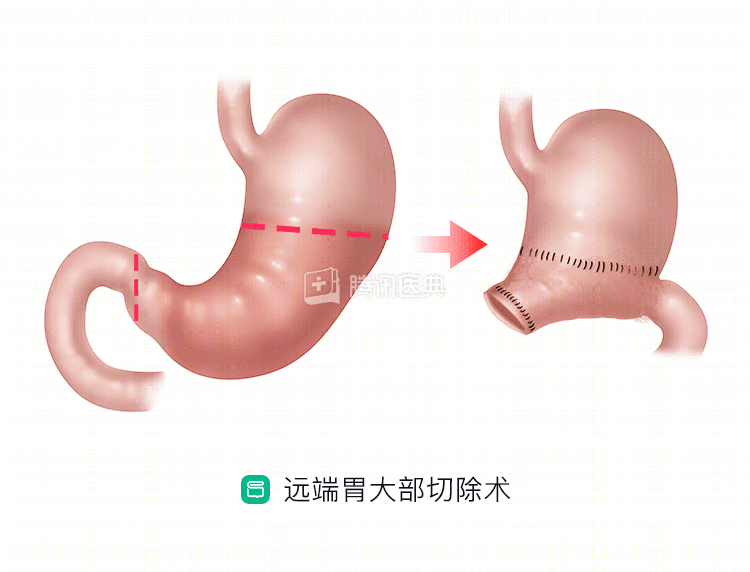
- Distal major gastrectomy: mainly for sinus cancer and some early limited gastric body cancer.
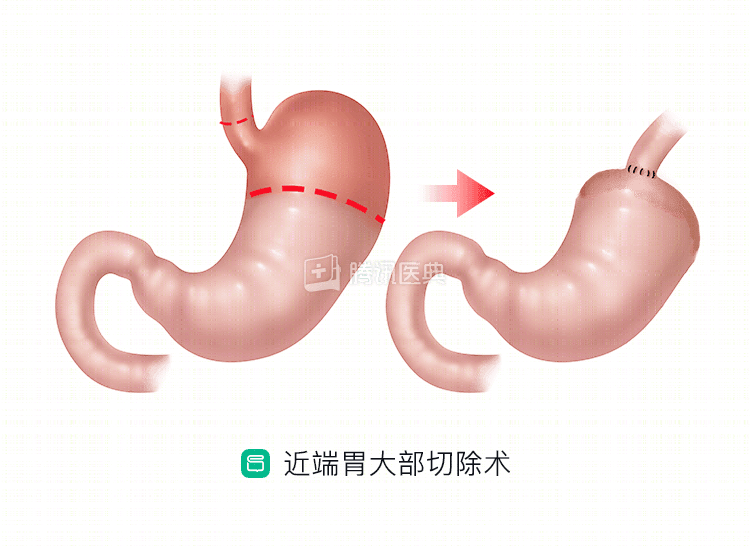
- Proximal major gastrectomy: It can be used for tumors in the proximal part of the gastric body and cardia, including gastric cardia cancer and larger benign gastric tumors.
- Total gastrectomy: for cancer of the body of the stomach and progressive cancer of the upper part of the stomach, cancer of the gastric sinus infiltrating into the body of the stomach, multiple gastric cancers, residual gastric cancer, and recurrent cancer after major gastrectomy for distal and proximal gastric cancer.
Differences in the extent of resection and GI reconstruction methods
- Distal major gastrectomy: The resection area includes 2/3 to 4/5 of the stomach and part of the duodenum distally (i.e., far from the entrance of the stomach), in addition to some other tissues of the mesentery and lymph nodes to be cleared.
Digestive tract reconstruction includes direct anastomosis of the gastrectomized stump to the duodenal stump (Billroth I), and anastomosis of the stump to the jejunum (Billroth II, Roux-en-Y).
- Proximal gastrectomy: The esophagus is usually cut 4 to 5 cm above the cardia at the entrance of the stomach, and in cases of cardia involving the lower esophagus, the esophagus is usually cut 4 to 5 cm above the tumor and the stomach is cut 5 cm below the tumor. In principle, the residual stomach volume should not be less than 1/2 of the whole stomach. in addition, some lymph nodes need to be dissected.
For reconstruction of the GI tract, doctors usually choose to anastomose the stomach to the esophagus.
- Total gastrectomy: As the name implies, the stomach is completely removed. The resection usually includes the lower esophagus, the whole stomach, part of the duodenum, and the greater omentum. The tumor is more than 3 cm from the incisional margin of the esophagus and the duodenum is usually 3 cm below the pylorus, and the associated lymph nodes are cleared.
The GI reconstruction is usually performed by anastomosis of the esophagus to the jejunum (Roux-en-Y procedure).