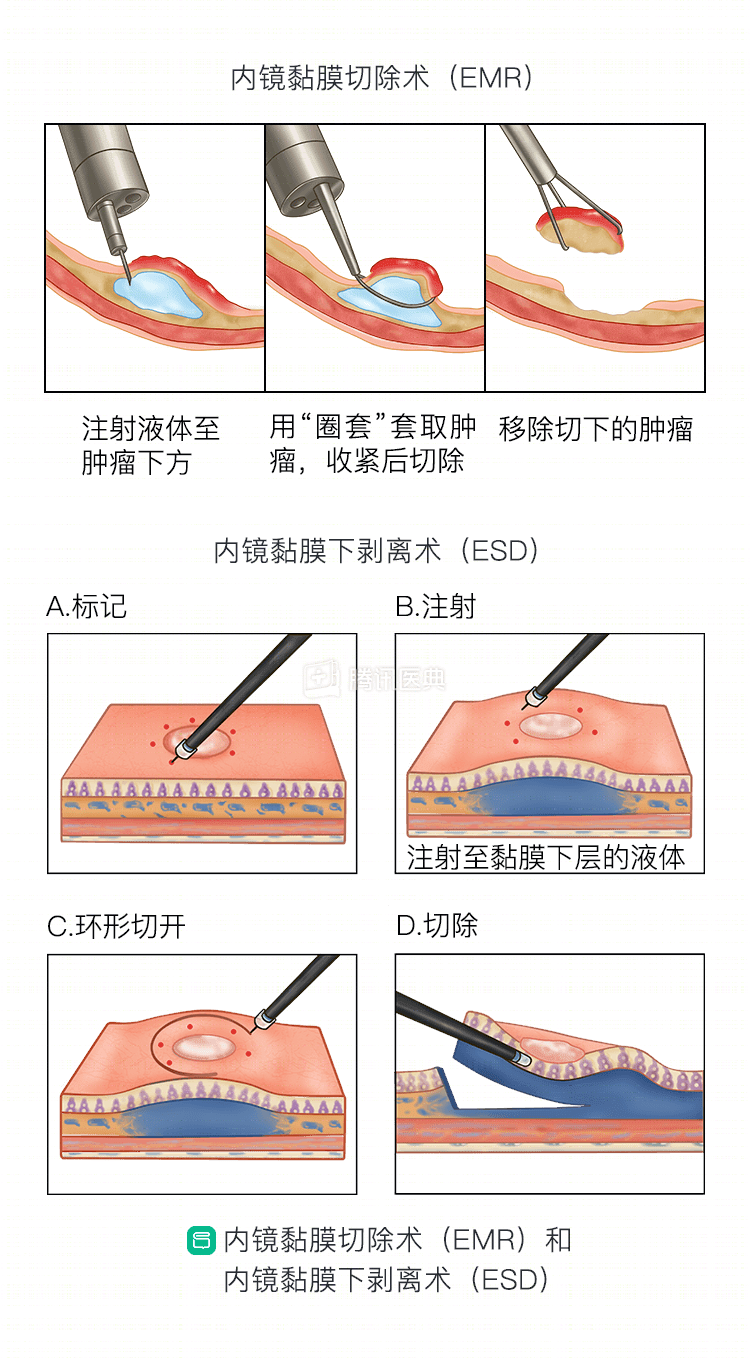
The two most commonly performed endoscopic resections are endoscopic mucosal resection (EMR) and endoscopic submucosal dissection (ESD).
What is the procedure for endoscopic resection?
.
The procedure for both types of endoscopic dissection is similar to cutting a watermelon rind: saline is injected underneath the mucosal layer to create a submucosal cushion that lifts the mucosal layer; then the entire mucosal layer and most of the submucosal tissue is peeled off by an endoscopic electric knife along the cushion underneath the mucosal layer (see the figure below for the procedure). The wound will heal completely after endoscopic excision in about 1 to 2 months.
How is healing determined after endoscopic resection?
The excised specimen will be sent to the pathology department. The pathologist will examine it thoroughly and carefully and give a final diagnosis.
- If the final pathology diagnosis confirms that the cancer is within the mucosal layer and the lesion is cut cleanly, then you are considered to have had a complete resection. If there are no other risk factors for lymph node metastasis, such as vascular thrombosis, poor differentiation, etc., then you do not need additional treatment.
- If the pathologic diagnosis is submucosal invasive carcinoma, meaning that the cancer is beyond the submucosa, the subsequent treatment options are different depending on the depth of infiltration. The deeper the cancer infiltration, the higher the rate of lymph node metastasis. In medicine, the submucosa is further subdivided into 3 layers: upper, middle, and lower.
- To clarify whether the lymph nodes are metastatic or not, that is, to clarify the final staging of the tumor;
- Even if there are lymph node metastases, surgery also allows for regional lymph node dissection, which can also lead to radical resection.
If the lesion is located close to the pharynx or in elderly patients with severe underlying comorbidities, the risk of surgery is high enough to receive radiation therapy.
Co-written by Dr. Wang Police, Endoscopy Center, Peking University Cancer Hospital