
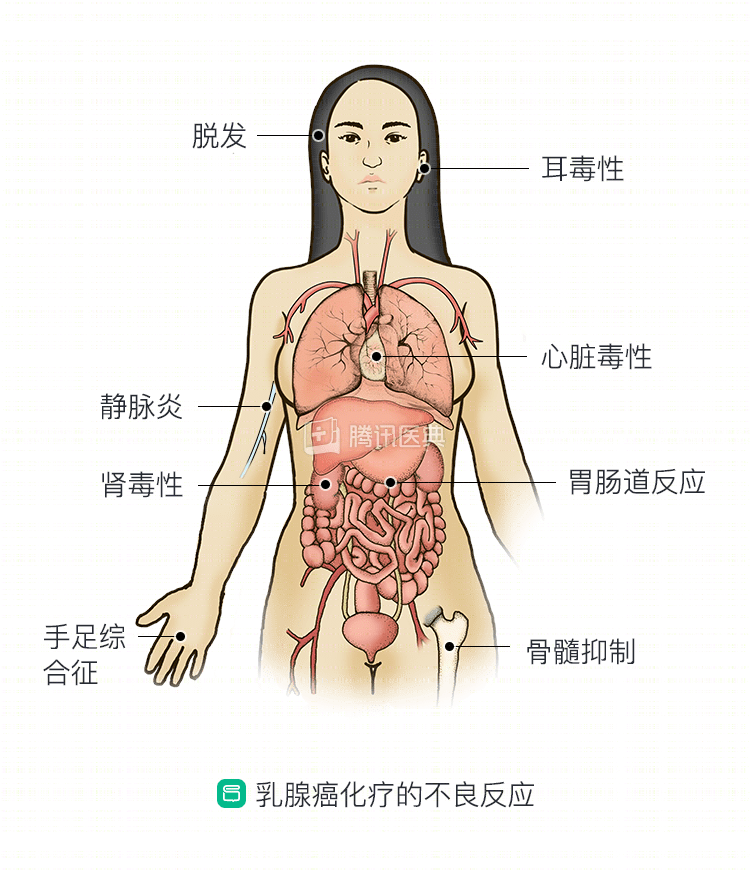
When it comes to chemotherapy, most people’s first reaction is pain, because chemotherapy can cause a number of adverse reactions. The following is a description of these adverse reactions and how to deal with them.
Common adverse reactions
Bone marrow suppression
Bone marrow suppression is the most common side effect of chemotherapy.
- Leukocyte (neutrophil) reduction is the most frequent manifestation and appears early, often starting 1 week after chemotherapy discontinuation, with leukocytes reaching a nadir 10 to 14 days after discontinuation, remaining low for 2 to 3 days and then slowly rebounding to normal by day 21 to 28. A decrease in leukocytes can lead to weakness, reduced resistance and susceptibility to infection. A severe decrease in leukocytes (clinically known as degree IV myelosuppression) can lead to fever, fungal or bacterial infections, and even life-threatening conditions. Therefore, during chemotherapy, doctors will request regular blood tests and apply drugs (recombinant human granulocyte colony-stimulating factor) to improve bone marrow hematopoiesis when needed, or infuse leukocyte suspension to increase white blood cell levels to prevent severe myelosuppression and related complications. Patients should also follow the doctor’s instructions to review blood tests regularly, avoid meeting guests, and pay attention to room air disinfection. Those who have experienced severe myelosuppression will need to change or reduce the dose when receiving chemotherapy again.
- The platelet reduction occurs slightly later and also drops to a minimum in about 2 weeks, with a rapid decline and a short time at the bottom before rebounding. The few chemotherapeutic agents that can cause a severe reduction in platelets are gemcitabine and carboplatin. Decreased platelets can be treated with drugs (thrombopoietin) and component transfusions. Those with significant reduction also need special care, such as reducing activity, preventing injury, absolute bed rest if necessary; avoiding actions that increase abdominal pressure, paying attention to laxation and cough suppression; reducing the chance of mucosal injury, eating soft food, prohibiting behaviors such as nose and ear picking, prohibiting tooth brushing, using oral care instead, etc. Attention should also be paid to the management of nosebleeds and consultation with ENT if necessary. Doctors should also be informed when there are changes in mental, sensory and motor changes and respiratory rhythm to prevent intracranial hemorrhage.
- Red blood cell decline occurs much later and to a lesser extent, and patients who have multiple courses of chemotherapy usually have mild to moderate anemia only, and severe anemia is rare. It can be treated with drugs (erythropoietin) and component transfusions.
Gastrointestinal reactions
Nausea and vomiting are the most common early toxic reactions to chemotherapy drugs, and severe vomiting can even lead to inability to eat, followed by dehydration and electrolyte disturbances. Chemotherapy-induced vomiting can be divided into acute vomiting (within 24 hours of chemotherapy) and delayed vomiting (within 1 week of chemotherapy). Regimens containing platinum (especially cisplatin) and anthracycline (doxorubicin, etc.) drugs cause more severe nausea and vomiting. Nausea and vomiting are more likely and more severe in younger patients than in older patients.
Medications commonly used to prevent and treat chemotherapy drug-induced vomiting include hormones (eg, dexamethasone), metoclopramide, 5-hydroxytryptamine receptor antagonists (toltestrone, ondansetron, etc.), and neurokinin (NK)-1 receptor antagonists (arrepitant, lorapitant, etc.). These drugs are usually used on the day of chemotherapy, but may be prolonged at the discretion of the physician in cases of severe reactions. Antiemetic drugs should not be used for longer periods of time. For those who have difficulty eating during chemotherapy, the doctor will supplement nutrition through intravenous infusion. The diet during chemotherapy should be light and refreshing, moderate in temperature, small and frequent, easy to digest, and then gradually increase nutrition after the digestive reactions have disappeared.
Mucosal injury is also common during chemotherapy, mostly manifested as stomatitis, esophagitis, and mouth ulcers. Fluorouracil analogs are most likely to cause mucosal inflammation and oral ulcers, with a higher incidence with sequential applications than with single applications. The main discomfort of patients is pain and inability to eat. In addition to B vitamin supplementation, topical symptomatic treatment is available through mucosal anesthetics, frequent mouth rinses to keep the mouth clean, and bulk or patch for oral ulcers. When unable to eat, the doctor will consider necessary nutritional support through intravenous fluids.
Hair loss
Chemotherapy drugs usually cause hair loss, with anthracyclines, cyclophosphamide, paclitaxel, and vincristine most likely to cause hair loss, often occurring 2 to 3 weeks after the start of chemotherapy. A tourniquet or ice cap can be used during chemotherapy if available and may reduce the degree of hair loss. After hair loss, pay attention to scalp care, preferably wearing a soft hat or silk scarf, gently clean the scalp, and try to avoid friction, sunlight and other stimuli. Hair loss caused by chemotherapy is generally reversible, with hair regrowth beginning 1 to 2 months after stopping the drug.
Phlebitis
Phlebitis caused by chemotherapeutic agents is still inevitable in recent years, despite significant improvements in superficial venipuncture equipment and techniques. Commonly used chemotherapeutic drugs such as anthracyclines, vincristine, cyclophosphamide, fluorouracil, and cisplatin can lead to varying degrees of phlebitis, which first manifests as local discomfort or mild pain, followed by local redness, swelling, burning, pain, and striated red lines along the course of the vein, with hard striated nodes palpable on pressure, and in severe cases, pus at the puncture site, accompanied by systemic symptoms such as chills and fever.
The most fundamental way to avoid phlebitis is to perform central venous catheterization (PICC), which allows the drug to be injected directly into the deep superior vena cava without causing vascular irritation without passing through a peripheral superficial vein. Those who are not eligible for PICC may be able to do the following.
- More massage and rubbing of the extremities to promote circulation and maintain vascular elasticity.
- When infusing highly concentrated, stimulating medications, your doctor may ask to control the infusion rate from being too fast. You can also cut a potato into slices 2 to 4 mm thick, cover it with a layer of plastic wrap and place it on the end of the puncture site near the heart, changing it once an hour until the infusion is complete and removing it.
- The nurse will do the following before and after the infusion, using saline puncture before the infusion, followed by a successful infusion of chemotherapy drugs, and then at least 25 ml of saline to flush the blood vessels after the infusion to prevent irritation from the residual drug.
For those who have developed phlebitis, your doctor may recommend the following treatment.
- Cold compresses. In cases of phlebitis or extravasation, a topical cold compress of a 50% magnesium sulfate solution covered with a soft film may be applied 2 to 3 times a day after consultation with your doctor. Alternatively, ice, saffron alcohol, and ethanol (50% concentration) may be applied cold.
- Local closure. Ask your healthcare provider to apply local closure with 0.25% procaine and dexamethasone, followed by a cold compress with magnesium sulfate.
- Use creams. Consider using mucopolysaccharide polysulfate cream applied directly to the affected area, massaged with a cotton swab for 5 minutes, and then applied 5 times daily once the swelling has resolved. If extravasation has not occurred, applying cream to the injection site before infusion can also prevent phlebitis.
Severe chemical skin inflammation or even skin necrosis can occur if subcutaneous leakage occurs when vincristine is infused through a superficial vein, so it is best to follow your doctor’s recommendation to receive a central venous line when receiving a chemotherapy regimen containing vincristine.
Specific adverse reactions
Cardiac toxicity
Anthracyclines and trastuzumab, the most commonly used drugs for breast cancer patients, have been associated with more significant cardiotoxicity, as have cyclophosphamide, cisplatin, paclitaxel, and vincristine drugs. Cardiotoxicity caused by chemotherapy drugs is usually manifested by arrhythmias (including conduction block), changes in ST-T or T wave of ECG, angina pectoris, myocardial infarction and even heart failure. A previous history of heart disease and hypertension are risk factors for cardiotoxicity in chemotherapy patients. Anthracyclines will cause irreversible myocardial damage, which can be fatal in severe cases, after the total dose of anthracyclines exceeds a certain maximum, and physicians will prevent this by limiting the cumulative dose of doxorubicin and epirubicin. The cardiotoxic effects of epirubicin and liposomal doxorubicin are relatively mild.
For cardiotoxicity caused by chemotherapy drugs, timely detection is most critical, so physicians monitor electrocardiographic changes during drug administration, perform regular echocardiography, detect changes in left ventricular ejection fraction (LVEF), etc., and may also use cytoprotective agents (dexrazoxane, amphotericin, etc.) to protect the myocardium.
In conclusion, the immediate and long-term toxic effects of chemotherapy drugs on the heart have a significant impact on patient survival and outcome, and recovery is usually good if detected and managed early during chemotherapy.
Ototoxicity and nephrotoxicity
Ototoxicity is a relatively specific toxic reaction to cisplatin, mainly in the form of tinnitus and reduced high-frequency hearing, which is mostly reversible at therapeutic doses and does not require special management. However, it is important to note that those with otitis media should inform their physicians that cisplatin should not be used in general. Care should also be taken to avoid aminoglycoside antibiotics (streptomycin, gentamicin, etc.) during the use of cisplatin to avoid irreversible deafness.
Cisplatin and gemcitabine are both nephrotoxic, but the nephrotoxicity of cisplatin is more pronounced, occurring 7 to 12 days after dosing, as evidenced by increased urea nitrogen and creatinine on tests and decreased glomerular filtration rate. It usually recovers in about 1 month, but irreversible kidney damage may occur in a few patients. Doctors usually use the following measures to prevent kidney injury.
- Hydration. Drink as much water and rehydrate intravenously as possible during drug administration (from the day of chemotherapy to 2-3 days after chemotherapy), with a daily infusion of 2000-3500 mL to ensure a 24-hour urine output of >2500 mL. If this is not enough, your doctor may increase the amount of rehydration and use diuretics to promote drug excretion and reduce drug kidney injury.
- Use diuretics. Mannitol and furosemide may enhance renal excretion and reduce renal injury without affecting the antitumor activity of cisplatin.
- Protection of renal function with cytoprotective agents (amphotericin, reduced glutathione, and magnesium) prior to chemotherapy.
- Switch to other less nephrotoxic platinum drugs, such as oxaliplatin and nedaplatin.
.
Allergic reactions
Allergic reactions caused by chemotherapeutic drugs are classified as local and systemic. Both cisplatin and paclitaxel chemotherapeutic agents may cause systemic allergic reactions that manifest as dyspnea, bronchitis or laryngospasm, facial flushing, and decreased blood pressure.
The incidence of allergic reactions due to cisplatin is low.
Paclitaxel drugs may cause significant systemic allergic reactions in some patients after injection due to the use of co-solvents, which can be fatal in severe cases. Therefore, before using paclitaxel drugs, doctors usually recommend taking anti-allergy medication in advance and performing cardiac monitoring during the medication in addition to continuing the anti-allergy medication. Once an allergic reaction occurs, the doctor will immediately stop the drug, give oxygen, inject dexamethasone, epinephrine, atropine and other drugs for resuscitation. If an allergic reaction occurs with the application of paclitaxel, the physician will generally not use the drug again on the patient.
Hand-foot syndrome
Hand-foot syndrome is a cutaneous toxic reaction that can begin 11 to 360 days after starting chemotherapy (median time of appearance 79 days), mainly in the pressure areas of the hands and feet, and manifests as numbness, dullness, abnormal sensation, tingling, painlessness, or pain in the hands and feet, swelling or erythema of the skin, flaking, cracking, hard node-like blisters, or severe pain. Breast cancer patients taking capecitabine have nearly 50% chance of developing hand-foot syndrome. Scientific care can prevent its occurrence, reduce symptoms, and promote recovery.
- Try to avoid friction, pressure, heat and sunlight on the hands and feet, for example, by wearing appropriate shoes, avoiding long walks and heavy work and exercise, not washing hands and feet in hot water, elevating hands and feet at rest, and using sun protection.
- Take vitamin B6 and celecoxib orally as directed by your doctor.
- Keep the skin of hands and feet moist with petroleum jelly and emollient cream.
- Avoid spicy and irritating foods.
- Treat the blisters with medical attention. Do not tear them with your hands when there is peeling skin, you can cut off the lifted part with sterile scissors.
Life can be inconvenient for those who develop hand-foot syndrome, but current clinical data show that those who develop hand-foot skin reactions have better outcomes.
The right choice is to treat chemotherapy scientifically and rationally, to communicate more with your medical oncologist, and to follow medical advice to prevent and manage complications.