Approval Date:
Fluticasone Furoate Vilanterol Inhalation Powder Instructions
Please read the instructions carefully and use under the direction of a physician
[Drug Name]
Generic name: Fluticasone furoate vilanterol inhalation powder nebulizer(II); fluticasone furoate vilanterol inhalation powder nebulizer(III)
Trade name: VANRISU/RELVAR
English name:Fluticasone Furoate and Vilanterol Trifenatate Powder for Inhalation (II);Fluticasone Furoate and Vilanterol Trifenatate Powder for Inhalation (III)
Hanyu Pinyin:Kangsuan Futikasong Weilanteluo Xirufenwuji (II) Kangsuan Futikasong Weilanteluo Xirufenwuji (IIIIII >)
[Ingredients]
This product is a compound formulation, the active ingredients of which are fluticasone furoate and vilanterol triphenylacetate.
Active Ingredient: fluticasone furoate
Chemical name:(6a,11b,16a,17a)-6,9-difluoro-17-{[(fluoromethyl)thio]carbonyl}-11-hydroxy-16-< span style="font-family:equivocal">methyl-3-oxoandrosta-1,4-diethylenetriamine-17- Methyl furoate
Chemical structure formula:
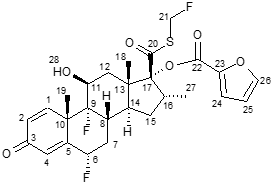
Molecular Formula:C27H29F3O6S
Molecular weight:538.58
Active ingredient: vilanterol triacetate
Chemical name: Triphenylacetic acid-4-{(1R)-2-[(6-{2-[(2,6-< span style="font-family:isochronous">dichlorobenzyl)oxygen]Ethoxy}< span style="font-family:equivocal">hexyl)aminoamines =”font-family:Times New Roman”>]-1-hydroxyethyl}-2-(< span style="font-family:equivocal">hydroxymethyl)phenol
Chemical structure formula:
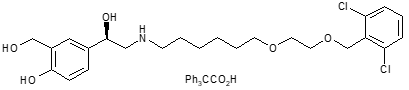
Molecular Formula:C24H33Cl2NO5-C20H16O2
Molecular weight:774.8
Excipients: Lactose (C12H22O11 -H2O), magnesium stearate.
[Properties]
This product is a multi-dose powder inhaler, fluticasone furoate and vilanterol triacetate are sealed in two aluminum foil strips in the form of a blister, and placed in a powder inhaler (easy-to-access deviceELLIPTA), the contents of the vesicles are white powder.
[Indications]
Asthma “font-family:Times New Roman”>
This product is indicated for the maintenance therapy of adults with asthma, which includes regular inhaled glucocorticoids and“on demand“inhaled short-actingbeta2-receptor agonist therapy in poorly controlled adult asthma patients.
Chronic Obstructive Pulmonary Disease (COPD)
This product100μg/25μgis indicated For FEV1as a percentage of normal expected valueafter inhalation of bronchodilators<70% of adults with a history of acute exacerbations despite regular bronchodilator therapyMaintenance therapy in patients with COPD.
[Specifications]
(1) Flutilizer furoate Carlson Velanterol inhalation powder(II): fluticasone furoate100 μgwith vilanterol triacetate (as vilanterol)25 μg;
(2)Fluticasone furoate vilanterol inhalation powder spray(III):fluticasone furoate200 μg span>with vilanterol triacetate (as vilanterol)25 μg.
[dosage]
Asthma
Adults:
One inhalation of this product per day100 μg /25 μg {Fluticasone furoate100 μg with triphenylacetic acid vilanterol (as vilanterol)25 μg} or200 μg /25 μg {fluticasone furoate200 μgwith vilanterol triacetate (as vilanterol)25 μg}.
After the patient inhaled this product15 minutes there is usually an improvement in lung function.
However, patients should be informed that in order to maintain control of their asthma symptoms, they need to take their medication regularly on a daily basis and should continue to use it even if they are asymptomatic.
If asthma symptoms occur between doses, short-acting beta2-receptor agonists for rapid symptom relief.
For patients requiring inhaled low to moderate doses of glucocorticoids in combination with long-actingβ 2-receptor agonists in adults, the use of 100 μg/25 μgas the starting dose. If patients are not well controlled with 100μg/25μgtreatment, consider Increasing the dose to 200 μg/25 μg, thus further improving asthma control.
Physicians should reassess patients periodically to keep them on the optimal dose of fluticasone furoate at all times/Vilanterol, and dose adjustments must be made according to medical advice. The dose should be adjusted to the lowest dose that will maintain symptom control.
For patients requiring higher doses of inhaled glucocorticoids in combination with long-actingβ 2-receptor agonists in adult patients, the use of 200 μg/25 μgas the starting dose.
The maximum recommended dose can be considered to be increased to200μ g/25μg once daily.
Patients with asthma should be given fluticasone furoate (FF, appropriate for the severity of the disease. Roman”>FF) dose of this product specification.
17Youth and under and children:
Not yet determined17< span style="font-family:equinox">year-old and younger adolescents and children for the treatment of asthma.
No data are available.
Chronic obstructive pulmonary disease (COPD)
Adults
Once daily inhalation of this product100μg/25μg.
Patients inhale this product after 16-17minutes there is usually an improvement in lung function.
Special Populations:
Older patients (> 65years): no dose adjustment is required (see item [Pharmacokinetics]).
Patients with renal insufficiency
: No dose adjustment is required (see item [Pharmacokinetics]).
Patients with hepatic insufficiency: study results showed systemic exposure to fluticasone furoate in subjects with mild, moderate, and severe hepatic insufficiency (including). style=”font-family:Times New Roman”>CmaxandAUC) in subjects with mild, severe hepatic insufficiency. () were elevated (see item [Pharmacokinetics]).
Patients with hepatic insufficiency should use this product with caution because of the higher risk of possible systemic adverse reactions associated with corticosteroids.
In patients with moderate or severe hepatic insufficiency, the maximum dose of this product is100 μg/25 μg =”font-family:equinox”> (see item [Precautions]).
[Adverse Reactions]
Summary of Safety Features
According to asthma andCOPD data from a large clinical trial to determine the adverse effects associated with fluticasone furoate/ Incidence of adverse reactions associated with vilanterol. In the asthma clinical development program, a total of 7034 patients were included in the pooled adverse reaction assessment. In total, the pooled adverse reaction assessments in the COPDclinical development program included6237 subjects.
with fluticasone furoate/ The most common adverse reactions after vilanterol were headache and nasopharyngitis. The safety profile was similar in patients with asthma andCOPD, except for pneumonia and fractures. In clinical studies, pneumonia and fractures were the most common adverse reactions in patients with COPD.
List of adverse reactions
Summarized by system organ classification and frequency of occurrence Adverse reaction list. The incidence is defined as:
very common (≥1/10); common (≥1/100and <1/10); occasional (≥1/1,000 and <1/100); rare (); rare (≥1/10,000and<1/1,000 ); very rare (<1/10,000); very rare (<1/10,000).
Adverse reactions are listed in decreasing order of severity within each incidence category.
|
System organ classification > |
Adverse effects |
Frequency |
|
Infection and Infection |
Pneumonia* Upper respiratory tract infection Bronchitis Influenza Oropharyngeal candidiasis |
Common |
|
Immune System Disorders |
hypersensitivity reactions. including tachyphylaxis, angioedema, rash, and urticaria |
rare |
|
Neurological Disorders |
Headache Tremors |
very common rare |
|
Ophthalmology |
Blurred vision |
occasional |
|
Psychiatric Disorders |
anxiety |
rare |
|
Cardiovascular Disease |
Premature beats Palpitations Tachycardia |
occasional Rare Rare |
|
Respiratory. Thoracic and mediastinal disorders |
Nasopharyngitis Oropharyngeal pain Sinusitis Pharyngitis Rhinitis Cough Vocal difficulties Paradoxical bronchospasm |
Very common Common
rare |
|
Gastrointestinal Disorders |
Abdominal pain |
Common |
|
Musculoskeletal and connective tissue disorders |
Arthralgia Back pain Fracture*** Muscle spasms |
Common |
|
General and Delivery Site Diseases |
Fever |
Common |
*, **, see below“part for details of adverse reactions“
Particulars of adverse reactions
*Pneumonia (see [Precautions])
2items are repeated for a period of. span>1year pooled analysis of clinical studies (n = 3255) were included in a pooled analysis of clinical studies in moderate to severe (after bronchodilator useFEV1mean percentage of expected value 45%. Standard Deviation(SD) 13%) with an acute exacerbation in the past year and -family:Times New Roman”>COPD patients in the past year. The results showed that the number of incident pneumonia cases per 1000 patient-years in fluticasone furoate/Vilanterol 200/25 μg < span style="font-family:equivocal">group for 97.9, fluticasone furoate< span style="font-family:Times New Roman">/Vilanterol 100/25 μg group for 85.7 and vilanterol 25 μg group for 42.3. For severe pneumonia, the corresponding number of events per 1000patient-years were, respectively. family:Times New Roman”>33.6, 35.5, , , and 7.6, and for severe pneumonia, each “font-family:Times New Roman”>1000patient-years of corresponding incident cases of severe pneumonia in fluticasone furoate/Vilanterol 200/25 μg group for 35.1, fluticasone furoate/Vilanterol 100/25 μggroup was 42.9 and vilanterol 25μg group was12.1. Finally, the number of cases of lethal pneumonia adjusted for exposure to fluticasone furoate/vilanterol 200/25μggroup for8.8< span style="font-family:isoline">, compared to fluticasone furoate/Vilanterol 100/25μg group for 1.5 and vilanterol 25 μg The group is 0.
A placebo-controlled study (SUMMIT ) in moderateCOPD with a history or increased risk of cardiovascular disease. family:equivocal”>(mean value of FEV1as a percentage of expected value after inhalation of bronchodilators at screening60% of subjects with fluticasone furoate/The incidence of pneumonia in the vilanterol, fluticasone furoate, vilanterol, and placebo groups was: adverse events (6%, 5% , 4%, 5%), serious adverse events (3%, 4%, 3%, 3%), deaths judged to be due to pneumonia during treatment (0.3%, 0.2%, 0.1%, 0.2% ); exposure adjustment rate (per 1000patient-years) for adverse events (39.5, 42.4, 27.7, 38.4), serious adverse events (22.4, 25.1, 16.4, 22.2), death due to pneumonia during treatment (1.8, 1.5, 0.9, 1.4).
in11summary analysis of asthma studies (7,034 patients) per span>1,000patient-years incidence of pneumonia in fluticasone furoate/Vilanterol 200/25 μggroup for 18.4, fluticasone furoate/Vilanterol 100/25 μggroup and 9.6 in the placebo group8.0.
**fracture
2items repeated in a total of12months of study3,255 COPDpatients, the incidence of fracture was low in all treatment groups, with fluticasone furoate/Vilan The incidence was higher in the trospium group (2%) than in the vilanterol25 μggroup (<1%). Although there were more fractures in the fluticasone furoate/vilanterol group than in the vilanterol25 μggroup, but fluticasone furoate/Vilanterol group and the incidence of fractures typically associated with glucocorticoid use in both the vilanterol group<1% (e.g., spinal compression fractures/, thoracolumbar fractures, hip fractures, and acetabular fractures).
SUMMITThe incidence of all fracture events in the study of incidence in each of the fluticasone furoate/vilanterol, fluticasone furoate, vilanterol, and placebo groups were2%, and the incidence of fractures usually associated with glucocorticoid use was<1%. The exposure-adjusted rates (per treatment1000patient-years) for all fracture events were13.6, 12.8, 13.2, 11.5, and the incidence of fractures usually associated with glucocorticoid use were3.4, 3.9, 2.4, 2.1.
In11summary analysis of asthma (7,034patients), the incidence of fracture <1% and was usually associated with trauma.
[Contraindicated]
This product is contraindicated in patients with severe milk protein hypersensitivity and in patients with proven hypersensitivity to fluticasone furoate, vilanterol, or any of the excipients; in patients with persistent asthma or other conditions requiring intensive measuresCOPD or initial treatment of acute exacerbations of asthma.
[Precautions]
Disease aggravation
This product is not intended for use with acute asthma symptoms orCOPDacute exacerbations, in which case treatment with a short-acting bronchodilator is required. When increased dosage of short-acting bronchodilators is required for symptom relief, this is an indication of poor disease control and the patient should be reassessed by the physician.
Asthma orCOPD. span style=”font-family:equinox”>Patients should not discontinue this product without medical advice, as symptoms may return after discontinuing the drug.
Adverse events and acute exacerbations of symptoms associated with asthma may occur during treatment with this product. Patients should be advised to seek medical advice and continue treatment if asthma symptoms remain uncontrolled or worsen after initiation of treatment with this product.
Paradoxical bronchospasm
Paradoxical bronchospasm may occur immediately after medication administration with increased wheezing. It should be treated immediately with a short-acting inhaled bronchodilator when it occurs. The product should be discontinued immediately, and a patient assessment should be performed, using alternative therapy if necessary.
Cardiovascular effects
Cardiovascular effects, such as arrhythmias (supraventricular tachycardia and premature beats), may occur with sympathomimetic drugs (including this product). In a placebo-controlled study, after use of this product in subjects with a history of cardiovascular disease or an increased risk of cardiovascular disease in moderateCOPD The risk of cardiovascular events, serious cardiovascular events, or adjudicated cardiovascular death was not increased compared to placebo (see [Adverse Reactions]), although it should be used with caution in patients with severe cardiovascular disease or arrhythmias, hyperthyroidism, uncorrected hypokalemia, or in patients prone to hypokalemia.
Patients with hepatic insufficiency
Patients with moderate to severe hepatic insufficiency should be treated with100 μg/25 μgdose and patients should be monitored for systemic glucocorticoid-related adverse reactions (see item [Pharmacokinetics]).
Systemic glucocorticoid effects
All inhaled glucocorticoids have the potential for systemic effects, especially at high doses applied over long periods of time. These effects are much less likely to occur than with the application of oral corticosteroids. Possible systemic effects include Cushing’s syndrome
, Cushing’s-like features, adrenal suppression, decreased bone mineral density, growth retardation in children and adolescents, cataracts, and glaucoma; more rarely, psychological or behavioral effects include euphoria, sleep disturbance, anxiety, depression, or irritability (mainly in children).
This product should be used with caution in patients with tuberculosis, chronic infection or untreated infection.
Local effects of inhaled glucocorticoids
In clinical trials, patients receiving fluticasone furoate/Vilanterol-treated subjects have experienced localized oral and pharyngeal Candida albicans infections. In the event of such infections, appropriate topical or systemic (i.e., oral) treatment with fluticasone furoate/vilanterol should be administered in conjunction with continued antifungal therapy, but sometimes it may be necessary to interrupt fluticasone furoate/vilanterol therapy. Please advise patients to rinse their mouth with water but not swallow after inhalation to help reduce the risk of oropharyngeal candidiasis.
Visual impairment
Visual disturbances may be reported with systemic and topical use of glucocorticoids. When a patient presents with blurred vision or other symptoms of visual disturbance, consideration should be given to advising the patient to visit an ophthalmologist for possible conditions including cataract, glaucoma, or rare conditions such as central plasmacytoid chorioretinopathy–CSCR , which has been reported after systemic and topical use of glucocorticoids) was evaluated.
Hyperglycemia
Elevated blood glucose has been reported in patients with diabetes mellitus and the risk of elevated blood glucose in patients with a history of diabetes mellitus should be considered with the application of this product.
COPDPneumonia in patients
in patients with inhaled glucocorticoidsCOPD patients, an increased incidence of pneumonia, including hospitalization due to pneumonia, has been observed.
There is some evidence that increased steroid doses cause an increased risk of pneumonia, but this has not been conclusively confirmed in all studies.
There is intrinsic variability in the extent to which inhalation of glucocorticoid-based products causes a risk of pneumonia, and there is no conclusive clinical evidence.
Since the clinical presentation of pneumonia is similar to that ofCOPDacute exacerbations, physicians should treatCOPDpatients are alert to the possibility of pneumonia.
Risk factors for pneumonia in patients with COPD include. Smoking, old age, low body mass index (BMI) and severeCOPD.
This product 200μg/25μgNot for use in COPD patients. Compared to 100μg/25μg doses,200μg/25μgdose did not provide additional benefit and may have a potentially elevated risk of systemic glucocorticoid-related adverse reactions (see item [Adverse Reactions]).
Pneumonia in patients with asthma
Pneumonia is common in patients with asthma who are on higher doses. The risk of pneumonia in asthma patients treated with this product200 μg/25 μg is numerically greater than that in patients treated with this product100 μg/25 μg or placebo (see item [Adverse Reactions]). There are no established risk factors.
Severe Asthma-Related Events
LABAmonotherapy has potential to increase the risk of asthma-related death. Available data from controlled clinical trials suggest thatLABAmonotherapy can increase the risk of asthma-related hospitalizations in pediatric and adolescent patients. When treating patients with asthma, physicians need to initiate a combination of inhaled glucocorticosteroids and LABA for patients who are not adequately controlled with long-term asthma control medications, such as inhaled glucocorticosteroids, or depending on disease severity span style=”font-family:equivocal”>treatment in patients prescribed fluticasone furoate/Vilanterol.
A one-time28 span style=”font-family:equivocal”>week U.S. placebo-controlled trial of adding another LABAto conventional asthma treatment. family:isoline”>(salmeterol) was compared with placebo for safety and showed an increase in asthma-related deaths in subjects treated with salmeterol (13,176out of 13 subjects treated with salmeterol,13,179 of the placebo-treated subjects, 33; relative risk:4.37 [95% CI:1.25, 15.34]). This increased risk of asthma-related mortality is thought to belabora (including vilanterol, fluticasone furoate/one of the active ingredients in vilanterol) with like effects.
About ICS/LABAClinical studies of compounded formulations
For evaluation withICS span>single drug compared toLABAwith >ICSin combination with LABAwhether it reduces the risk of serious asthma-related events in adult and adolescent patients3 large, 26-item study in adult and adolescent patients. style=”font-family:isoline”>week multicenter study. Its results showed that compared to ICSmonotherapy,ICS/LABAdoes not increase the risk of serious asthma-related events (including asthma-related death, tracheal intubation, and hospitalization).
Immunosuppressive effects
Patients using drugs that suppress the immune system are more likely to develop infections than healthy individuals. For example, chickenpox and measles may be more severe or even fatal in susceptible children or adults using glucocorticoids. Special care should be taken to avoid exposure to this product in such children or adults who do not have these diseases or who have received appropriate immunizations. It is not known how the dose, route of administration, and duration of glucocorticoids affect the risk of developing disseminated infections. The role of underlying disease and/ or prior glucocorticoid therapy on risk is also not known. If the patient was exposed to varicella, varicella zoster immunoglobulin (VZIG) prophylaxis may be indicated. Intramuscular mixed immunoglobulin (IG) prophylaxis may be indicated if the patient was exposed to measles. (For complete VZIG and IGprescribing information, please refer to the appropriate medication insert.) If chickenpox develops, consider antiviral medication.
Active or old tuberculosis infection; systemic fungal, bacterial, viral, or parasitic infection; or patients with ocular herpes simplex should use (if needed) inhaled glucocorticoids with caution.
Patients switching from systemic glucocorticoid therapy to this product
Patients switching from systemically active glucocorticoids to inhaled glucocorticoids need special attention because patients with asthma switching from systemic glucocorticoids to systemic death due to adrenal insufficiency has occurred during and after conversion from less bioavailable inhaled glucocorticosteroids. After discontinuation of systemic glucocorticoids, restoration of hypothalamic – pituitary – adrenal (HPA) function takes several months.
Previously maintained to receive20 mg Patients on >or higher doses of prednisone (or its equivalent) may be most vulnerable, especially with almost complete discontinuation of their systemic glucocorticoids. During thisHPAsuppression, when exposed to trauma, surgery, or infection (especially gastroenteritis) or other conditions associated with severe electrolyte loss Patients may develop signs and symptoms of adrenal insufficiency. Although fluticasone furoate/vilanterol may be useful inCOPD or control of these symptoms during an asthma attack, but at the recommended dose, fluticasone furoate/< /span>Vilanterol provides less than normal physiologic amounts of systemic glucocorticoids and does not provide the salt corticosteroid activity necessary to respond to these emergencies.
In stressful, severeCOPD >during acute exacerbations or acute exacerbations of severe asthma, patients who have discontinued systemic glucocorticoids should be instructed to immediately resume oral glucocorticoids (high dose) and to contact their physician for further instructions. These patients should also be instructed to carry a warning card indicating that during stress, severeCOPDacute exacerbations or acute exacerbations of severe asthma, they may require of systemic glucocorticoid supplementation.
Patients requiring oral glucocorticoids who are switching to fluticasone furoateVilanterol should be followed by slow withdrawal from systemic glucocorticoid administration. This can be achieved by reducing weekly during fluticasone furoate/vilanterol treatment2.5 mgprednisone daily dose to achieve prednisone taper. During oral glucocorticoid withdrawal, lung function (FEV1or maximal expiratory flow), betareceptor agonist use andCOPDor asthma symptoms. In addition, patients should be observed for signs and symptoms of adrenal insufficiency, such as fatigue, malaise, weakness, nausea, vomiting, and hypotension.
Shift patients from systemic glucocorticoid therapy to fluticasone furoateVilanterol may reveal allergic conditions previously suppressed by systemic glucocorticoid therapy (e.g., rhinitis, conjunctivitis, eczema, arthritis, eosinophilia).
During discontinuation of oral glucocorticoids, some patients may develop systemically active glucocorticoid withdrawal symptoms despite maintenance or even improvement in respiratory function (e.g., arthralgia and/ or muscle pain, malaise, depression).
Comorbidities
Like all sympathomimetic amine-containing drugs, fluticasone furoate/vilanterol should be used with caution in patients with convulsive disorders or hyperthyroidism and in patients with abnormal reactions to sympathomimetic patients with abnormal reactions to sympathomimetic amines. The related β2-adrenoceptor agonist salbutamol has been reported to exacerbate preexisting diabetes mellitus and ketoacidosis when administered intravenously.
Excipients
with galactose intolerance,Lapplactase deficiency or glucose–galactose This product should not be used in patients with rare genetic disorders with malabsorption.
Other
No studies have been conducted on the effects of this product on the ability to drive or operate machinery. Due to the pharmacological properties of fluticasone furoate or vilanterol, no adverse effects on these working abilities are expected.
Use with caution in athletes. This product contains fluticasone furoate and vilanterol (in the form of triphenylacetate) and requires verification of the World Anti-Doping Organization’s (WADA Annual Prohibited Ingredient list to determine if it is a permitted drug for an athlete to take.
[For Pregnant and Lactating Women]
Pregnancy
Animal studies have shown reproductive toxicity at non-clinically relevant exposures (see item [Pharmacologic Toxicology]). There are no or limited data on the use of fluticasone furoate and vilanterol in pregnant women.
Use in pregnant women should only be considered if the expected benefit to the mother outweighs any potential risk to the fetus
this product.
Lactation
Fluticasone furoate or vilanterol and/ or metabolites are secreted via human milk with limited information. However, other glucocorticoids and β2–receptor agonists can be detected in human milk (see item [Pharmacology and Toxicology]). The risk of breastfeeding to the neonatal/infant cannot be excluded.
A decision must be made whether to discontinue breastfeeding or discontinue the product after considering the benefits of breastfeeding in children and the benefits of treatment in mothers
treatment.
Fertility
No human fertility data are available. Animal studies have shown no effect on fertility (see item [Pharmacology and Toxicology]).
[Pediatric Use]
This product is not indicated for use in children and adolescents. The safety and efficacy of 17year-old and younger adolescents and children in the treatment of asthma have not been established.
Growth effects
Transoral inhaled glucocorticoids may result in slower growth when used in children and adolescents. Poorly controlled asthma or use of glucocorticoids, including inhaled glucocorticoids, may cause slowed growth in children and adolescents. The effect of long-term treatment with inhaled glucocorticoids (including fluticasone furoate) in children and adolescents on final adult height is unknown.
[Geriatric use] See [Dosage]
[Drug Interactions]
At the dose levels used in clinical applications, clinically significant drug interactions are unlikely due to the low plasma concentrations following inhalation administration.
withβ< /span>receptor blocker interactions
β2–< span style="font-family:equivocal">adrenergic receptor blockers may attenuate or antagonizeβ2adrenoceptor agonist effects. Concomitant use of nonselective and selectivebeta2adrenoceptor blockers should be avoided unless there is an important reason to do so.
with CYP3A4inhibitor interactions
fluticasone furoate and vilanterol both have a broad first-pass effect, mediated by hepatic enzymesCYP3A4and rapid clearance.
Due to the potentCYP 3A4 >inhibitors (e.g., ketoconazole, ritonavir) may increase systemic exposure to fluticasone furoate and vilanterol, the combination should be avoided unless the benefit outweighs systemic glucocorticoid side effects, in which case patients should be monitored for systemic glucocorticoid side effects. Inhalation administration of this product (200 μg/25 μg) and oral potent were conducted in healthy subjects style=”font-family:Times New Roman”>CYP3A4inhibitor ketoconazole ( 400 mg) in a drug interaction study with repeated dosing. Co-application resulted in a meanAUC of fluticasone furoate ( (024) andCmax
by 36%and >33%, increased exposure to fluticasone furoate caused serum cortisol of 0-24hour weighted mean decrease27%. The combined application resulted in a meanAUC for vilanterol(0-t) andCmax
increased by 65%and >22%. Increased exposure to vilanterol did not cause β2– agonist-related systemic effects (increased heart rate, blood potassium, or QTcFinterval).
withP-Interaction of glycoprotein inhibitors
Fluticasone furoate and vilanterol are bothP-glycoprotein (P-gp) substrate. In a clinical pharmacology study in healthy subjects, the combined application of vilanterol with potentP-gp and intermediate-actingCYP3A4 inhibitors (verapamil), which showed no significant effect on verantelor pharmacokinetics. Clinical pharmacology studies with specificP-gpinhibitors in combination with fluticasone furoate have not been performed.
Sympathomimetic drugs
Co-administration with other sympathomimetic drugs (alone or as part of combination therapy) may increase the adverse effects of this product. This product should be avoided in combination with other long-acting
β2–adrenergic receptor agonists or those containing β2–adrenoceptor agonists were used concomitantly.
Pediatric population
Drug interaction studies have been conducted in adults only.
[Drug overdose]
Signs and symptoms
Overdose of this product may produce signs and symptoms associated with monotherapy overdose, including knownβ2–receptor agonist class
Signs and symptoms consistent with overdose effects of inhaled glucocorticoids (see item [Precautions]).
Treatment< span style="font-family:Times New Roman">
There is no specific treatment for this overdose. In the event of an overdose, patients should receive appropriately monitored supportive therapy with appropriate monitoring, if necessary.
CardioselectiveVilanterol is considered only for severe vilanterol overdose effects that are clinically significant and for which supportive measures are ineffectivebetareceptor blockers. Cardioselectivebetareceptor blocking drugs should be used with caution in patients with a history of bronchospasm.
Further treatment should be based on clinical indications or national poison center recommendations (if available).
[Clinical Trial]
Clinical Efficacy and Safety
Asthma
In 3item randomized, double-blind, IIIphase study (HZA106827,HZA106829andHZA106837) were evaluated for safety and efficacy in the treatment of persistent asthma in adults and adolescents. At visit1prior to the visit, all subjects applied at least 12weeks ofICS (inhaled glucocorticoids), alone or in combination with LABAin combination. All patients in the studyHZA106837at visit1before1at least one acute exacerbation requiring the application of oral glucocorticoid therapy during the year. HZA106827is a study with a duration of 12week study, compared with the placebo group[n=203]compared to the placebo group evaluating this product100 μg/25 μg [n=201]< span style="font-family:Arial">and fluticasone furoate100 μg [n=205]Efficacy and safety of once-daily dosing. HZA106829is a once-daily24week study with fluticasone propionate500 μgadministered twice daily[n=195]compared with this product200μg/25μg [n=197]andand family:Times New Roman”>FF 200 μg [n=194]) for efficacy and safety when administered once daily.
In the studyHZA106827/ HZA106829, the primary effectiveness endpoint included clinical visits of subjects at the end of treatmentFEV1 valley (pre- and pre-inhaled bronchodilator) change from baseline, and change in the subgroup of subjects at the end of treatment post-dose0-24hour weighted mean continuousFEV1. Change from baseline in the percentage of on-treatment24hour periods without emergency medication was a secondary endpoint with a degree of certainty. See Table 1 for the results of the primary and key secondary endpoints in these studies.
Table1- HZA106827andResults for primary and critical secondary endpoints in HZA106829. span>
|
Study number |
HZA106829 |
HZA106827 |
||
|
FF/VItherapeutic dose*(μg) < /td> |
FF/VI200/25 once a day< span style="font-family:Times New Roman"> contrast FF 200< span style="font-family:equals">once a day |
FF/VI200/25 once a day contrastFP 500 span style=”font-family:equals”>twice daily |
FF/VI100/25 once a day contrastFF 100 span style=”font-family:equals”>once a day |
FF/VI100/25 once a day contrast |
|
FEV1Valley Change from Baseline (Last Observation Carryover Method (LOCF) span style=”font-family:equine”>) |
||||
|
Treatment differences PValue (95% CI) |
193mL p<0.001 (108, 277) |
210mL p<0.001 |
36mL p=0.405 (-48, 120) |
< span style="font-family:Times New Roman">172mL p<0.001 (87, 258) |
|
< span style="color:black">After administration0-24hour-weighted mean continuousFEV1 |
||||
|
136mL p=0.048 (1, 270) |
206mL p=0.003 (73, 339) |
116mL p=0.06 (-5, 236) |
< span style="font-family:Times New Roman">302mL p<0.001 (178, 426) |
|
|
24hour change from baseline in percentage of periods without emergency medication application | ||||
|
Treatment differences PValue (95% CI) |
11.7% p<0.001 (4.9, 18.4) |
6.3% p=0.067 (-0.4, 13.1) |
10.6% p<0.001 (4.3, 16.8) |
19.3% p<0.001 (13.0, 25.6) |
|
24hour asymptomatic period percentage change from baseline |
||||
|
Treatment differences PValue (95% CI) |
8.4% p=0.010 (2.0, 14.8) |
4.9% p=0.137 (-1.6, 11.3) |
12.1% p<0.001 (6.2, 18.1) |
18.0% p<0.001 (12.0, 23.9) |
|
AMChange in peak expiratory flow rate from baseline |
Treatment differences PValue (95% CI) |
33.5L/min p<0.001 (22.3, 41.7) |
32.9L/min p<0.001 (24.8, 41.1) |
14.6L/min p<0.001 (7.9, 21.3) |
33.3L/min p<0.001 (26.5, 40.0) |
|
PMChange in maximal expiratory flow from baseline |
||||
|
Treatment differences PValue (95% CI) |
30.7L/min (22.5, 38.9) |
26.2L/min (18.0, 34.3) |
12.3L/min p<0.001 (5.8, 18.8) |
28.2L/min (21.7, 34.8) |
*FF/VI = Fluticasone furoate/Vilanterol
FF = fluticasone furoate
FP = fluticasone propionate
HZA106837< span style="font-family:isoline">is a study with variable treatment periods (minimum24weeks and maximum76 weeks, with the majority of subjects receiving at least52weeks of treatment). In studyHZA106837, patients were randomized to receive this product100 μg/25 μg [n=1009]or fluticasone furoate 100 μg [n=1010] administered once daily. The primary endpoint of the studyHZA106837 was the time until the first severe time to acute exacerbation of asthma. An acute exacerbation of severe asthma was defined as a worsening of asthma requiring at least 3days of systemic glucocorticoid therapy or a worsening of asthma requiring systemic glucocorticoid therapy due to hospitalization or emergency room visit for asthma requiring systemic glucocorticoid therapy. The mean change in FEV1valley from baseline corrected was evaluated as a secondary endpoint.
In the studyHZA106837in comparison with fluticasone furoate alone100 μg Compared to patients on this product100μg/25μg, the risk of acute exacerbation of severe asthma was reduced20% (risk ratio0.795, p=0.036 95% CI 0.642, 0.985). The annual incidence of acute exacerbations of severe asthma per patient in the FF 100 μg group was 0.19 (approximately every5yearly), in this product100μg/25μggroup for >0.14(approximately every7 year1time). This product100μg/25μggroup was used with fluticasone furoate100 μggroup had a ratio of acute exacerbation incidence of 0.755(95% CI 0.603, 0.945). This indicates that in subjects treated with this product100 μg/25 μg, the incidence of acute exacerbations of severe asthma was higher thanFF 100μggroup by25%(p=0.014). The 24hour bronchodilator effect of this product was maintained throughout the one-year treatment period with no evidence of loss of efficacy (no rapid tolerability). At hours 12, 36 and 52 weeks and at the end of Compared with the fluticasone furoate100μggroup, this product100μg/25μggroup of FEV1 Valley improvement was maintained at 83mLto< span style="font-family:Times New Roman">95mL(p< 0.001, at the end95% CI 52,126mL). At the end of treatment this product100μg/25μgin the group44% of patients had good disease control (ACQ7 ≤0.75< span style="font-family:isoline">), while fluticasone furoate100 μg in the group >36% of the subjects had good disease control (p<0.001 95% CI 1.23, 1.82).
A randomized, double-blind, controlled study (HZA113719) in patients receiving low to moderate doses of inhaled glucocorticoid therapy or low doses ofICS/LABAcombination therapy in 12aged and older in Asian adolescent and adult subjects with persistent asthma given FF/VI dry powder inhaler100/2525 μg once daily for 12weeks to assess its association withFP 500 μgefficacy and safety compared with twice daily. A total of 311 subjects were randomized in this study (China randomized204),196 subjects completed the study (China completed113). The results of the Chinese subgroup showed that the FF/VI 100/25 group gained improved lung function compared to placebo, and the evening< span style="font-family:Times New Roman">PEFcorrected treatment difference amounted to 64.5 L/min(95% CI:54.0,,75.0;p<0.001), the morningPEFcorrected treatment difference was65.4 L/min( [95% CI< span style="font-family:equivocal">:55.4,75.4;p<0.001 ]), both clinically significant and statistically significant. Compared with placebo, the FF/VI 100/25 group also showed improvement in symptoms,24hour treatment difference in percentage correction for the period of no emergency medication application was 25.0([95% CI. 16.0, 34.0;p<0.001]), 24hour asymptomatic period with a percentage corrected treatment difference of 15.7( [95% CI:7.7,23.7;p<0.001] >), the treatment difference for AQLQis< span style="font-family:Times New Roman">0.70(95% CI) /span>:0.35,< span style="font-family:Times New Roman">1.06;p< 0.001). Overall,FF/VI 100/25 was well tolerated in a subgroup of Chinese subjects and no new safety concerns were identified.
A randomized, double-blind study (HZA113714) in patients treated with high-dose inhaled glucocorticoids or medium-doseICS/LABAcombination therapy in 12aged and older in Asian adolescent and adult subjects with persistent asthma given FF/VI dry powder inhaler200/25 μg once daily for for 12weeks to assess its efficacy and safety. A total of 313 subjects were randomized in this study (China randomized203),255 subjects completed the study (China completed164). The results for the Chinese subgroup showed that the FF/VI 200/25 group was not similar to the FP 500μg BDgroup compared with the group with improved pulmonary function in the eveningPEF< /span>corrected treatment difference was 33.3 L/min(95% CI: 23.1, 43.6; p<0.001); morning PEFcorrected treatment difference was38.4 L/min [95% CI:27.6, 49.3; p<0.001], all of which were clinically and statistically significant. In addition, compared with FP 500 μg BD,FF/VI 200/25 group also showed improvement in symptoms,24< span style="font-family:equinox">hour symptom-free period percentage corrected treatment difference was13.0% [95% CI:3.4, 22.7; p=0.008];AQLQ score-corrected treatment difference of 0.30 [95% CI:0.06, 0.53; p=0.013], all of which were statistically significant. Overall,FF/VI 200/25 μg OD was well tolerated and the adverse event profile was generally consistent with the use ofFP 500μg BD was similar to the adverse event profile seen with .
with salmeterol/fluticasone propionate combination control study
in adults and adolescents with persistent asthma24week study (HZA113091), once daily morning inhalation of this product100 μg/25 μg and twice daily inhalation of salmeterol/fluticasone propionate 50/250 μg all showed improvement in lung function from baseline. 0-24hour weighted meanFEV1mean treatment benefit from correction from baseline was 341 mL< span style="font-family:equivocal">(this product) and377 mL(salmeterol) /fluticasone propionate), which showed overall improvement with both treatments24hour lung function. The corrected mean treatment difference between the two treatment groups was 37 mL, which was not statistically significant (p=0.162) for FEV1valley, subjects in this group had a higher LSthan baseline mean change from baseline reached281 mL and salmeterol/ subjects in the fluticasone propionate group had a change of300 mL; (corrected mean difference19 mL(95% CI:-0.073, 0.034) is not statistically significant (p=0.485).
in acute exacerbations of asthma has not been compared with salmeterol/fluticasone propionate or otherICS/LABA compounded formulations have been studied in a controlled manner.
Fluticasone furoate monotherapy
A one-time24week randomized, double-blind, placebo-controlled study ( FFA112059) in adults and adolescents with persistent asthma versus placebo[n=115]< span style="font-family:Arial">compared with placebo, evaluation of fluticasone furoate100 μg once daily[n= 114]and fluticasone propionate 250 μgtwice daily[n=114] < span style="font-family:Arial">safety and efficacy. All subjects received at least1(screening visit) prior to the visit4weeks of stable doseICStreatment, not allowed prior to visit1 4weeks prior to use LABA. The primary effectiveness endpoint was the clinical visit at the end of treatment FEV1 trough (before inhaled bronchodilator and before drug administration) from baseline. During 24weeks of treatment24hour change from baseline in the percentage of periods without emergency medication application was a secondary endpoint with a degree of certainty. At the 24week time point, compared with placebo,FFandFPandmakeFEV1, respectively
valley increase146 mL(95% CI 36, 257 mL, p=0.009) and145 mL(95% CI 33, 257 mL , p=0.011). Compared with placebo,FFandFP respectively make2424242424 family:Arial”>hour period of non-application of emergency medication by 14.8%(< span style="font-family:Times New Roman">95% CI 6.9, 22.7, p<0.001) and) and 17.9%(95% CI 10.0, 25.7, p& lt;0.001).
Allergen excitation studies
in patients with mild asthma A repeated-dose, placebo-controlled,4 crossover study (HZA113126) in which this product was evaluated 100μg/25μg. /span>in early-onset and late-onset asthmatic reactions induced by inhaled allergens for bronchoprotection. Patients were randomized to receive this product100 μg/25 μg, fluticasone furoate 100 μg, vilanterol 25 μgor placebo once daily for 21 days after the last dose. span>1hour after the last administration for allergen provocation test. Allergens were house dust mites, cat dander, or birch pollen; allergen selection was based on individual screening tests of the subjects. SerialFEV1values were measured and compared with values after saline inhalation (baseline), before the allergen provocation test. Overall, the comparison with fluticasone furoate100 μg or vilanterol 25 μg administered alone compared to this product 100 μg/25 μg treatment group had the greatest effect on early-onset asthmatic response. Compared with vilanterol administered alone, this product 100 μg/25 μg and fluticasone furoate 100 μg effectively blocked the delayed asthmatic response. On day 22, as assessed by acetylcholine provocation test, it was found that this product100 μg/25 μgprotected significantly more against allergen-induced bronchial hyperreactivity than fluticasone furoate and vilanterol monotherapy.
Chronic obstructive pulmonary disease (COPD)
COPDClinical Development Program includes a 12week (clinical research and development program that will be conducted over a period of 12weeks (). span style=”font-family:Times New Roman”>HZC113107), 2items for a period of6months ( >HZC112206, HZC112207),2 items For a period of1year (HZC102970,HZC102871, ) and 1 items greater than1year of (SUMMIT) studies. These studies evaluated pulmonary function, dyspnea, and moderate-to-severe acute exacerbations.
6month study
HZC112206and< /span>HZC112207is a period of24week, randomized, double-blind, placebo-controlled, parallel-group study comparing
the effects of vilanterol and fluticasone furoate alone or in combination with placebo. HZC112206evaluated the effect of this product50/25 μg [n=206]and this product100 μg/25 μg [n=206] , with fluticasone furoate 100 μg [n=206], vilanterol 25 μg [n=205], and placebo [n = 207] compared to placebo (both administered once daily) in terms of efficacy. HZC112207 evaluated the efficacy of this product100μg/25μg [n=204] and this product200μg/25μg [n= 205] , with
fluticasone furoate100 μg [n=204], fluticasone furoate 200 μg [n=203], vilanterol 25 μg [n=203] and placebo [n = 205 ] compared to effectiveness (both administered once daily).
All patients enrolled in the study had at least10 pack-year history of smoking; after salbutamol inhalationFEV1/FVCratio less than or equal to0.70; after inhalation of salbutamol FEV1as a percentage of expected value less than or equal to70%, and modified medical study members at screening (mMRC) dyspnea score³2(rating 0-4). When filtering,HZC112206 and Pre-inhalation bronchodilator in HZC112207FEV1 as a percentage of the expected value had a mean value of 42.6% and 43.6%, respectively, and the mean airway reversibility was 15.9% and 12.0%. The synergistic primary endpoint in both studies was the first168days after dosing0-4hour weighted averageFEV1and day169after dosing FEV1Valley change from baseline.
A pooled analysis of the two studies showed that this product 100 μg/25 μg was clinically meaningful in terms of improvement in lung function. On day 169, application of this product100μg/25μgand vilanterol after application of this product, the corrected meanFEV1valley compared with placebo increased by 129 mL (95% CI:: 91, 167 mL, p<0.001) and 83 mL = “font-family:isoline”>(95% CI:: 46, 121mL, p<0.001). This product 100μg/25μg ofFEV1valley relative to vilanterol
(95% CI: 8, 83 mL, p= 0.017) increased by46 mL. On day 168, apply this product100μg/25μg and vilanterol after corrected mean0-4hour-weighted meanFEV1 compared to placebo increased by 193mL, respectively (95% CI: 156, 230 mL, p<0.001) and 145 mL (95% CI: 108, 181 mL, p< 0.001)
. This product 100μg/25μg of the corrected mean0-4hour weighted averageFEV1< span style="font-family:equivocal">compared to fluticasone furoate alone (95% CI: 112, 184 mL, p< 0.001) increased148 ml.
In AsianA randomized, double-blind, placebo-controlled study in patients with COPD( HZC113684) given to subjectsFF/VI dry powder inhaler50/25 μg, 100/25μgand200/25μg< span style="font-family:isoline">once daily for 24weeks to assess the efficacy and safety. A total of 646 subjects were randomized in this study (Chinese randomized489),537 subjects completed the study (China completed 419 subjects). The results for the Chinese subgroup showed that 3 of the FF/VIdose groups all achieved improved lung function,FEV1mean treatment difference in trough values compared with placebo (95% CI) wereFF/VI 50/25:0.158 (0.098, 0.218) L;FF/VI 100/25:0.177 (0.117, 0.236) L;FF/VI 200/25::0.228 (0.168, 0.288) L; allp< 0.001, these improvements were clinically significant and statistically significant. FF/VI 100/25 and200/25 groups of CRQ-SAS family:equivocal”> dyspnea scores also improved, with mean treatment differences (95% CI) of< span style="font-family:Times New Roman">0.31 (0.07, 0.55) , p=0.011. 0.33 (0.08, , 0.57) , p=0.009, all of which were statistically significant but did not reach the minimum clinically significant difference of 0.5. The overall safety observed in allFF/VIdose groups was similar to placebo.
12 month study
StudyHZC102970 andHZC102871 are a period of. 52week, randomized, double-blind, parallel-group study to compare the efficacy of this product200μg/25μg, this product 100μg/25μg, this product 50/25 μg, vilanterol, and /span> 25 μg (both once daily) on moderate/year incidence of severe acute exacerbations in the presence of at least10pack-year smoking history and after salbutamol inhalationFEV1/FVC ratio≤0.70 and after inhalation of salbutamolFEV1as a percentage of expected value ≤ 70% and before the visit1 span>12months documented at least one episode requiring antibiotics and/or oral glucocorticoids or required hospitalization forCOPD history of acute exacerbationsin COPD subjects were performed. The primary endpoint was the annual incidence of moderate and severe acute exacerbations. Moderate/severe acute exacerbations were defined as requiring the application of oral glucocorticoids and/ or antibiotics or hospitalization for exacerbation of symptoms. Both studies had a 4week introductory period during which all subjects received open salmeterol style=”font-family:Times New Roman”>/fluticasone propionate 50/250 μg 2 doses per day, after random assignment to < 52weeks of blinded study drug therapy prior to assignment to a standardizedCOPD drug therapy and disease stabilization. Prior to the introductory period, subjects discontinued prior COPD medications except for short-acting bronchodilators. Combination of inhaled long-acting bronchodilators (β2receptor agonists and anticholinergics is not allowed during treatment ), ipratropium/salbutamol combination, oralbeta2–receptor agonists and theophylline preparations. During the acute phase of COPDacute exacerbations, treatment with oral glucocorticoids and antibiotics was allowed according to special condition use guidelines. Subjects were allowed to use salbutamol as needed throughout the study period.
Results from two studies showed that compared with vilanterol, application of this product 100 μg/25 μg< span style="font-family:equivocal">once-daily treatment reduces moderate/severe< span style="font-family:Times New Roman">Annual incidence of acute exacerbations of COPD (Table2).
Table 2:
12 months after treatment Analysis of acute exacerbation rate
|
endpoint |
< strong>HZC102970 |
HZC102871 |
HZC102970and Summary analysis of HZC102871 |
|||
|
VI 25 μg (n=409) |
FF/VI 100μg/25μg (n=403) |
VI 25 μg (n=409) |
FF/VI 100μg/25μg (n=403) |
VI 25 μg (n=818) |
FF/VI 100μg/25μg (n=806) |
|
|
Moderate and severe acute exacerbations |
||||||
|
corrected mean annual incidence |
1.14 |
0.90 |
< span style="font-family:Times New Roman; font-size:9pt">1.05 |
0.70 |
1.11 |
0.81 |
|
< span style="font-size:9pt">to-Vilanterol 95% CI p-value Decrease in % (95% CI) |
0.79 |
0.66 <0.001 > |
0.73 |
|||
|
Absolute difference in number of times per year compared to Velantero< span style="font-family:Times New Roman"> (95% CI) |
0.24 (0.03, 0.41) |
0.36 (0.20, 0.48) |
0.30 (0.18, 0.41) |
|||
|
0.80 20 0.036 |
0.72 (0.59, 0.89) 28
0.002 |
0.76 24 p<0.001 |
||||
FF/VI: Fluticasone furoate Carbenoxolone/Vilanterol
VI: Vilantero Vilantero:
InHZC102970andHZC102871in the summary analysis of < span style="font-family:Times New Roman">52weeks, with Velanterol 25 μg compared to the application of
this product100μg/25μg after The corrected meanFEV1valley improved (42 mL 95% CI: 19, 64mL, p< ;0.001). Throughout the 1year treatment phase, this product’s 24hour bronchodilator effect persisted since the first dose and there was no evidence of reduced efficacy (no rapid tolerance).
Largely, in the pooled2 studies,2009named (< span style="font-family:Times New Roman">62%) of patients had a history of cardiovascular disease at screening//risk factors. The prevalence of cardiovascular history/risk factors was similar between treatment groups, with the most common being hypertension (46%), followed by hypercholesterolemia (29%) and diabetes mellitus (12%). In this subgroup, the reduction effect for moderate and severe acute exacerbations was similar to the overall population. In patients with a history of cardiovascular disease/risk factors, compared with vilanterol, this product 100 μg/25 μg group significantly reduced moderate/severe COPD The annual incidence of acute exacerbations ( The corrected mean annual incidence rates were1.18 and 0.83, a reduction of30%(95% CI 16, 42%, p<0.001)). At week 52, in this subgroup, the product 100 μg/25 μgto corrected meanFEV1valley improvement is better than that of vilanterol 25 μg (44 mL 95% CI:: 15, 73mL, (p=0.003)).
> 1year of research
SUMMIT is a multicenter, randomized, double-blind study in16,568 subjects to evaluate fluticasone furoate/Vilanterol100/25 μgcompared with placebo on survival. The primary endpoint was all-cause mortality, and the secondary endpoint was a cardiovascular composite event (on-treatment cardiovascular death, myocardial infarction, stroke, unstable angina, or transient ischemic attack).
Before randomization, patients were required to discontinue their previously used COPD at baselinemedications including long-acting bronchodilators combined with inhaled glucocorticoids (28%), long-acting bronchodilators (11%) and inhaled glucocorticoids alone (4%). Patients were then randomized to fluticasone furoate/Vilanterol100/25 μg, fluticasone furoate100 μg, vilanterol25 μg, or placebo groups, with a mean treatment 1.7years (SD=0, 9years).
ModerateCOPD ( The mean value of FEV1 as a percentage of the expected value after the use of bronchodilatorswas60% [SD=6%]) and patients with a history of cardiovascular disease or increased risk before the study12months, 61%patients reported noacute exacerbation of COPD,39% of patients reported≥1 sub-moderate/severeCOPDacute exacerbation.
All-cause mortality in fluticasone furoate/Vilanterol group was6.0% and the placebo group was 6.7%, and in the fluticasone furoate group6.1%, and in the vilanterol group6.4%. Exposure-adjusted per100patients/year (%/year) All-cause mortality in the fluticasone furoate/vilanterol group was3.1%/year and for the placebo group3.5%/< span style="font-family:equivocal">year, fluticasone furoate group was 3.2%/year, and vilanterol group was 3.4%/year. The risk of mortality in the fluticasone furoate/vilanterol group was similar to that in the placebo group(HR 0.88; 95% CI: 0.74 ~ 1.04; p=0.137), fluticasone furoate group (HR 0.96; 95% CI: 0.81 to 1.15; p=0.681), or the vilanterol group (HR 0.91; 95% CI: 0.77 ~ 1.09; p=0.299) compared with no significant difference.
Fluticasone furoate/< span style="font-family:equivocal">Risk of cardiovascular composite events in the vilanterol group versus the placebo group(HR 0.93; 95% CI: 0.75 ~ 1.14), fluticasone furoate group (HR 1.03; 95% CI: 0.83 to 1.28), or vilanterol group (HR 0.94; 95% CI: 0.76 ~ 1.16) compared with no significant difference .
compared with salmeterol/Study of fluticasone propionate combination control
InCOPD 12week study in patients with COPD () span>HZC113107) in which this product 100μg/25μg (daily1times morning dosing) and salmeterol/fluticasone propionate 50/500 μg (daily2< span style="font-family:isoline">doses), all showed improvement in lung function from baseline. 0-24 hour weighted meanFEV1
The mean treatment benefit from correction from baseline was 130 mL(this product) and 108 mL(salmeterol/fluticasone propionate), which demonstrated that both treatments improved overall24 /span>hour lung function. The mean treatment difference corrected between groups was 22 mL (95% CI: -18, 63mL), which was not statistically significant (p=0.282). Day85DayFEV1The mean change in trough value from baseline correction was111 mL(this group) and88 mL(salmeterol< span style="font-family:Times New Roman">/fluticasone propionate group); the difference between treatment groups was23 mL (95% CI: -20, 66), with no clinical significance or statistical significance (p=0.294).
InCOPD acute The role in exacerbation has not been studied in a controlled manner with salmeterol/fluticasone propionate or other commonly used bronchodilators.
[Pharmacological Toxicology]
Pharmacological effects
This product is a combination of fluticasone furoate and vilanterol.
Fluticasone furoate is a synthetic trifluorinated glucocorticoid with anti-inflammatory activity. The in vitro affinity of fluticasone furoate for binding to human glucocorticoid receptors is 29.9fold that of fluticasone propionate >1.7times that of fluticasone propionate. The exact mechanism of action of fluticasone furoate in improvingCOPD and asthma symptoms is not known.
Inflammation is COPD< span style="font-family:equine">and asthma as important pathogenic mechanisms. Glucocorticoids have been shown to act broadly on a wide range of cells involved in the inflammatory response (e.g., mast cells, eosinophils, neutrophils, macrophages, lymphocytes) and inflammatory mediators (e.g., histamine, arachidonic acid, leukotrienes, cytokines). Fluticasone furoate has anti-inflammatory effects in vitro and in vivo, including activation of glucocorticoid response components, inhibition of pro-inflammatory transcription factors such as NFκB, inhibition of antigen-induced pulmonary eosinophilia in sensitized rats.
Vilanterol is a selective long-actingβadrenoceptor agonist (LABA), has an activating effect on intracellular adenylate cyclase, which catalyzes the conversion of ATPto< span style="font-family:Times New Roman">3′,5′-cyclic adenosine monophosphate (cAMP), which elevates cAMPlevels, relaxing bronchial smooth muscle and inhibiting the release of tachyphylactic response mediators from cells, especially mast cells. Although the adrenergic receptors distributed in bronchial smooth muscle are mainly of theβ2 type, those distributed in the heart are mainly of the type. span>β1type, which is also distributed in the human heartβ2receptors in human heart, accounting for the totalβ< span style="font-family:isoline">of the number of adrenergic receptors10%to< span style="font-family:Times New Roman">50%, the exact function of the above-mentioned receptors has not been fully clarified. Even highly selectiveβ2receptor agonists may still act on the heart.
Toxicological studies
Fluticasone furoate
Genotoxicity: fluticasone furoateAmes< /span>test, in vitro rat lymphoma cell chromosome mutation test, and in vivo rat micronucleus test results were all negative.
Reproductive toxicity: male and female rats inhaled fluticasone furoate29 μg/kg/dand91 μg/kg/d (equivalent to AUC at the maximum clinically recommended inhaled dose, respectively, based on exposure3fold and8 (fold), no adverse effects on fertility were seen. Fluticasone furoate was inhaled during embryonic organogenesis in pregnant rats and rabbits91 μg/kg/d and8μg/kg/d (approximately the maximum clinically recommended inhaled dose based on body surface area4times and1 times), no teratogenicity was seen, but developmental delay was seen in rats and increased abortion was seen in rabbits at maternal toxic dose levels. Female rats inhaled fluticasone furoate27 μg/kg/dduring late gestation and lactation (equivalent to on a body surface area basis) ≤1times the maximum clinically recommended inhaled dose), no adverse effects on offspring development were observed.
Carcinogenicity: in2< span style="font-family:isoline">year carcinogenicity test, rats and mice inhaled fluticasone furoate9 μg/kg/dand19μg/kg/d (approximately the maximum recommended clinical inhalation dose based on body surface area >0.5 times) no increase in tumor incidence associated with administration was seen.
Vilanterol
Genotoxicity: vilanterolAmesassay, in vitro Syrian hamster embryo cell assay, in vitro rat programDNAsynthesis assay, and rat in vivo bone marrow cell micronucleus assay all showed negative results; the significance of the in vitro mouse lymphoma assay results was unclear.
Reproductive toxicity: male and female rats inhaled vilanterol31,500 μg/kg/dand37,100 μg/kg/d (equivalent to the maximum recommended clinical inhalation dose at AUC on an exposure basis5490 times) No adverse effects on fertility were seen.
Vilanterol was inhaled during embryonic organogenesis in pregnant rats and rabbits at doses as high as33700 μg/kg/d (equivalent to the maximum clinically recommended inhaled dose based on body surface area13000fold) and 5740 μg/kg/d(equivalent to AUC at the maximum recommended clinical inhalation dose on an exposure basis1000fold). In rats at the highest dose, rabbits at 591 μg/kg/d (equivalent to the maximum recommended clinical inhalation dose at exposure AUCof160dose did not show any embryonic– fetal malformation. Vilanterol was given by inhalation or subcutaneous injection to pregnant rabbits at doses as high as 5740 μg/kg/d or 300μg/kg/d (equivalent to the maximum clinically recommended inhalation dose at exposureAUCof1000fold) can lead to skeletal malformations in fetuses, as seen by incomplete ossification of the cervical vertebrae and metacarpals. Inhalation of vilanterol in rabbits can also lead to skeletal deformities associated with other b2b =”font-family:equilibrium”>receptor agonist-like typical reproductive toxicities such as cleft palate, open eyelids, sternal fusion, and limb flexion/Rotational barriers.
In a perinatal toxicity test, pregnant rats were given orally vilanterol10,000 μg/kg/d (equivalent to the maximum clinically recommended inhaled dose based on body surface area3900). span>fold), no offspring developmental abnormalities were observed.
Carcinogenicity: in2< span style="font-family:isoline">year carcinogenicity test, mice inhaled vilanterol29,500 μg/kg/d< span style="font-family:equivocal">(Based on exposure, equivalent to the maximum recommended clinical inhalation dose atAUCof8750fold), a significantly higher incidence of ovarian tubular stromal adenocarcinoma was seen in female mice at615 μg/kg/dno abnormal change in tumor incidence was seen at dose (at the exposed dose, equivalent to the maximum recommended clinical inhalation doseAUCof530< span style="font-family:isoline">fold); rats inhaled vilanterol at ≥84.4 μg/kg/ddose (equivalent to AUC at the maximum recommended clinical inhalation dose on a dew-dose basis = “font-family:Times New Roman”>45 times), a significantly higher incidence of ovarian tract smooth muscle tumors in female rats was seen, and the latency period of pituitary tumors was shortened in family:Times New Roman”>10.5 μg/kg/ddose did not show abnormal changes in tumor incidence (at the exposed dose, which is approximately the maximum recommended clinical inhalation doseAUCof2fold). The above rodent tumors are similar to other previously reported βadrenergic receptor agonist-induced tumors, and the human The relevance is unclear.
Compounding studies
No new toxicity was added by coadministration of fluticasone furoate and vilanterol compared to single agents in nonclinical safety trials.
Reproductive toxicity: Inhalation of fluticasone furoate or vilanterol alone during embryonic organogenesis in pregnant rats (equivalent to the maximum recommended clinical inhalation dose of the single drug, respectively, based on body surface area200 μg and 25 μgof5fold and40times), or combined inhalation of fluticasone furoate and vilanterol95 μg/kg/d, no structural deformities were seen.
[Pharmacokinetics]
Absorption
The mean absolute bioavailability of fluticasone furoate and vilanterol after inhalation administration of this product was15.2%and27.3%. The average oral bioavailability of fluticasone furoate and vilanterol was lower at 1.26% and <2%. Given the low oral bioavailability, the systemic exposure of inhaled administration of fluticasone furoate and vilanterol comes primarily from drug absorption through the lungs.
Distribution
After intravenous administration, fluticasone furoate and vilanterol were widely distributed in vivo, with a mean steady-state volume of distribution was 661 L and 165 L.
Fluticasone furoate and vilanterol bind less to red blood cells. In vitro, fluticasone furoate and vilanterol bind to human plasma
protein with high binding rates, averaging >99.6%, respectivelyand93.9%. There was no reduction in in vitro plasma protein binding in subjects with renal or hepatic insufficiency.
Fluticasone furoate and vilanterol are bothP-glycoprotein (P-gp) substrate, but because of its good molecular uptake, it is unlikely that either in combination with P-gp inhibitors would alter the The systemic exposure to fluticasone furoate or vilanterol.
Metabolism
According to in vitro data, the important metabolic pathways of both fluticasone furoate and vilanterol in humans are mainly mediated by CYP3A4mediated.
Fluticasone furoate is mainly mediated viaS-fluoromethylthioate group
Hydrolysis metabolizes the metabolites, and the cortisol activity of the metabolites is significantly reduced. Vilanterol is mainly metabolized by Odealkylation, which produces a series of metabolites whoseb1and >b2receptor agonist activity was significantly reduced.
elimination
After oral administration, fluticasone furoate is primarily cleared by metabolism in humans, with metabolites excreted almost entirely from the feces, <1% of the recovered radiolabeled dose was excreted via urine.
After oral administration,
Vilanterol is primarily cleared by metabolism, and studies of oral radioactive markers in humans have shown that approximately70% =”font-family:equinox”> and 30% of the radiolabeled dose is excreted as metabolites in the urine and feces. The apparent plasma elimination half-life of vilanterol after a single inhalation administration of this product averaged 2.5 hours. The effective half-life of vilanterol accumulation, as measured by repeated dose inhalation administration of vilanterol 25 μg, is16.0 hours (in asthmatic subjects) and 21.3 hours (COPD subjects ).
Adolescent and pediatric populations
Not yet in17adolescent and pediatric patients years of age and younger in which the pharmacokinetics of this product have been studied. The safety and efficacy of this product in adolescents and children aged 17 years and younger have not been established.
Special Populations
Older patients (> 65> 65) = “font-family:Arial”> years)
InIIIphaseCOPDand asthma studies evaluated the effect of age on the pharmacokinetics of fluticasone furoate and vilanterol. There was no evidence that age (12-84) could affect the pharmacokinetics of fluticasone furoate and vilanterol in subjects with asthma.
InCOPD span style=”font-family:isoline”>subjects there is no evidence that age can influence fluticasone furoate pharmacokinetics, although in41to84years of age range, vilanterol was observedAUC(0-24) by 37%. In light weight (35 kg) elderly subjects (84 years old) in whom the expected vilanterolAUC(0-24) than the estimated population35%(60years old, weighing 70 kgof = “font-family:Times New Roman”>COPD subjects), while Cmax >did not change. These differences are unlikely to be clinically meaningful.
in asthmatic subjects and COPDsubjects, no dose adjustment is recommended.
Patients with renal insufficiency
Clinical pharmacology studies of this product have shown that compared to healthy subjects, severe renal insufficiency (creatinine clearance<30mL/min) did not result in a significant increase in fluticasone furoate or vilanterol exposure, nor did it produce more pronounced glucocorticoid orβ2receptor agonist systemic effects. Dose adjustment is not required in patients with renal insufficiency.
No studies of hemodialysis effects have been performed.
Patients with hepatic insufficiency
Multiple doses of fluticasone furoate/Vilanterol continuously7day, compared to healthy subjects, subjects with hepatic insufficiency (Child-Pugh A, BorC ) increased systemic exposure to fluticasone furoate (AUC(0-24) elevated up to 3fold). Compared with healthy patients, subjects with moderate hepatic insufficiency (Child-Pugh B; fluticasone furoate/Vilanterol200μg/25μg ) Increased systemic exposure to fluticasone furoate was associated with a mean decrease in serum cortisol34%correlated. Subjects with moderate and severe hepatic insufficiency (Child-Pugh BorC) dose-standardized systemic exposure of fluticasone furoate was similar.
This product7after 7days of repeated dosing, mild, moderate or severe hepatic insufficiency (Child-Pugh A, Bor C) subjects in the Villantero family:Times New Roman”>
(Cmaxand< span style="font-family:Times New Roman">AUC) whole-body exposure did not increase significantly.
Mild or moderate hepatic insufficiency compared with healthy subjects (vilanterol, 25 μg) or severe hepatic insufficiency (vilanterol, 12.5 μg) in subjects with fluticasone furoate/vilanterol< span style="font-family:Times New Roman">
Co-application on badrenergic drugs Systemic effects did not produce clinically meaningful effects.
Race
In subjects with asthma, East Asian (mainly Japanese) and Southeast Asian subjects (who make up the total population >12-13%) of fluticasone furoate AUC(0-24)
estimates were on average 33% higher than other ethnic groupsto53%. However, there was no evidence that higher systemic exposure in these populations was accompanied by a greater24hour urinary cortisol excretion effect. For vilanterol, sub-state subjects compared with other ethnic subjects
Estimated Cmax
higher220 to< span style="font-family:Times New Roman">287%, whileAUC(0-24) were similar. However, there was no evidence that higher vilanterol Cmax had a clinically meaningful effect on heart rate.
inCOPD. span style=”font-family:isoline”>subjects, an estimated 13-14% of the total populationin East Asian (mainly containing Japan) and Southeast Asian subjects) of fluticasone furoate AUC (0-24) estimates were on average higher than in Caucasian subjects23% to30%. However, there is no evidence that higher systemic exposure in this population is associated with a greater24hour urinary cortisol excretion effect. There was no evidence that race affected the estimated pharmacokinetic parameters of vilanterol in COPD subjects.
Gender, weight, andBMI
Phase IIIPhase III study of population pharmacokinetic Kinetic Analysis [According to1213 asthmatic subjects (712females),12251225femalesCOPDsubjects (392female)] showed no evidence of sex, weight, or span>BMI (body mass index) on fluticasone furoate pharmacokinetics.
Population pharmacokinetic analysis showed [based on 856 asthmatic subjects (500females),1091 COPD subjects (Data from subjects (340females) ], there was no evidence that sex, weight, orBMI = “font-family:equine”> had an effect on vilanterol pharmacokinetics.
No need to base the dose on sex, weight, orBMIdose adjustment.
[Storage]
Sealed, not to exceed25°C for storage in a dry place. Keep the inhaler in a sealed box to avoid moisture and remove it only before starting to use.
If refrigerated, remove the inhaler at least 1 before first use. family:equinox”>hour to bring the inhaler to room temperature and store in a dry place no more than 25C after use.
[Package]
Each box contains1 easy ner (ELLIPTA), sealed in a laminated aluminum foil box with a silica gel desiccant bag inside.
Enerator has built-in2 strips of Aluminum foil blister strips, each arranged 14pcs or30 blisters, one containing fluticasone furoate100 μgor200μg, and one containing vilanterol triacetate (as vilanterol )25μg/ blister.
14Suction/box, 30suctionbox, suction /box.
[Expiration date]
24months.
This product has been opened in a sealed box for 6week or when the counter reads “0”(all blisters are used), whichever is earlier, discard this product. The easy-access device should not be reused and should not be disassembled.
[Executive Standard]
Imported drug registration standards:JX20160169
[Imported drug registration certificate number]
Fluticasone furoate vilanterol inhalation powder (II):
Fluticasone furoate vilanterol inhalation powder (III):
[Manufacturer]
Company Name: Glaxo Group Limited
Company Address:980 Great West Road, Brentford, Middlesex TW8 9GS, United Kingdom(UK)
Production facility:Glaxo Operations(UK)Ltd. (trading as Glaxo Wellcome Operations)
Manufacturing Address:Priory Street, Ware, Hertfordshire, SG12 0DJ, United Kingdom (UK)
Office in China Address: Middle Xizang Road, Shanghai168Metropolitan Headquarters Building6Floor; >
Postal Code: 200001
Phone Number: (86 21 ) 23019800
Fax Code: (86 21) ) 23019801
GSKService Hotline: 400-183-3383/800-820-3383
Trademarks are owned by or used under license by GlaxoSmithKline.
©[2018]Glaxo Schick Group or its licensors
[Usage Guidelines]
This product is intended for administration by the inhalation route only.
Should be administered at the same time each day.
To be given in the evening or in the morning at the physician’s discretion.
If a dose is missed, the next dose should be inhaled the following day at the usual dosing time.
If storing the easy-to-use device in the refrigerator, leave it at least at room temperature before use1hour before use.
Use and Handling Instructions
When using the Easy Nano for the first time, there is no need for prior The device does not require any special preparation. The Enner is ready for immediate use. Just follow the step-by-step instructions.
The parts included in the outer case of the Easy Nano are shown in the figure below:
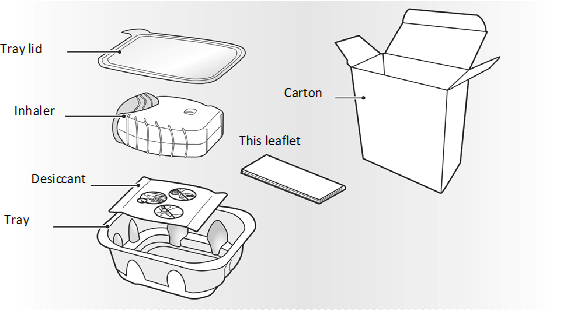






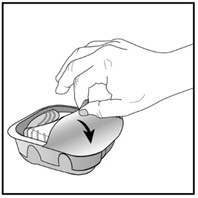
Energy comes in a foil case. Open the foil case only when you are ready to inhale a dose of medication. When you are ready to use the Enactor, remove the lid and open the foil box. The foil cassette contains a desiccant sachet for dehumidification. Discard this desiccant sachet – do not open, eat, or inhale the desiccant.


Only turn on the Easy Nasal when you are ready to inhale a dose of medication.
When you remove the easy-access device from the cassette, it is in “font-family:Times New Roman”>’off‘‘ =”font-family:equals”> status. Please write “Discard“Date. “Discard “date is 6 weeks after first opening the foil box . After that date, the inhaler may not be used again. The foil box can be discarded after the first opening.
After inhalation administration, the patient should rinse the mouth with water and should not swallow the mouthwash.
as follows30Dose Enactor step-by-step instructions are also applicable to14 Dose Enactor.
-
Please read the following instructions before use
If you open and close the easy-access lid when you are not inhaling medication, you will lose your medication dose.
The lost dose will be safely stored in the epidural, but cannot be reused.
The easy-access device is designed to prevent accidental inhalation of additional medication or 1double dose inhalation.




-
Preparing for medication
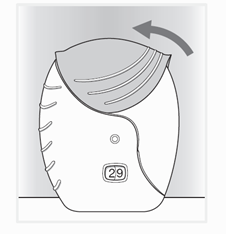
Open the cap when you are ready to inhale the medication. Do not shake the easy-napper.
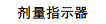
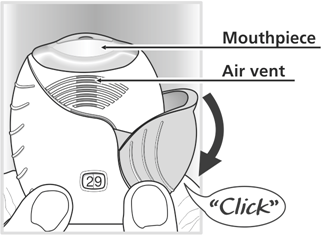
Follow the example diagram and slide the cover down until you hear ““click“” sound. Prepared for inhalation medication. Decrement1by the dose counter to confirm that the medication has been released.
If you hear‘ click‘sound, but the dose indicator does not decrement, then the easy-napper is not released1aspiration of the drug. They should be returned to the physician and counseled.The epidural should not be shaken at any time.



3. Inhaled medications
Please keep the easy-to-use device away from the mouth and nose and exhale as much as possible.
Do not exhale into the easy-access device.
Place the nozzle between the upper and lower lips with both lips wrapped tightly around the nozzle.
Do not block the vent hole with your fingers during use.
Inhale slowly and smoothly and deeply. Hold your breath as long as possible
(at least3-4seconds) .
- Withdraw the easy-access device from the mouth.
- Exhale slowly and gently

You should not be able to taste or feel the medication, especially if you are using an epidural correctly.
To clean the nozzle, wipe it clean with a dry tissue before closing the easy-access lid.
4. Close the easy-napper and gargle
Please slide the easy access cover up as far as possible until it covers the mouthpiece.
Please rinse your mouth with water after using the Easy-Napkin and do not swallow.
This will reduce the possibility of sore mouth or throat side effects.