PrefacePreface
This document was drafted in accordance with the provisions of GB/T 1.1-2020 “Guidelines for Standardization Work Part 1: Structure and Drafting Rules for Standardization Documents”.
This document was proposed by the National Cancer Center.
This document is attributed by the Chinese Society of Preventive Medicine.
This document is drafted by: National Cancer Center, Nanjing Medical University, Peking Union Medical College, Cancer Hospital Shenzhen, Chinese Academy of Medical Sciences, China Medical University, Lanzhou University, Yunnan Cancer Hospital, Shanxi Cancer Hospital, Shandong Cancer Hospital, Zhejiang Cancer Hospital.
The main drafters of this document: He Jie, Shen Hongbing, Chen Wanqing, Wu Ning, Jiang Yu, Zhou Baosen, Li Ni, Huang Yunchao, Gong Jiyong, Liu Shiyuan, Chen Qihang, Zhao Shaohong, Guo Youmin, Wu Jianlin, Tan Fengwei, Ma Hongxia, Ying Jianming, Huang Yao, Tang Wei, Li Wenbin, Zhao Shijun, Li Jiang, Wang Fei, Zhang Juan, Tian Jinhui, Du Lingbin, Zhang Yongzhen.
IntroductionIntroduction
Lung cancer is one of the most common malignant tumors, ranking first in incidence and death from malignant tumors worldwide and in China. Recent studies have shown that lung cancer mortality is reduced by 24% in men and 33% in women with low-dose spiral CT screening. Currently, most of the scientific evidence guiding lung cancer screening comes from studies in Europe and the United States, while the epidemiological characteristics of lung cancer in China are different from those in Europe and the United States, such as the high proportion of non-smoking women, so it is not appropriate to copy foreign experience in lung cancer screening in China. The establishment of this document will greatly promote the homogeneity and quality of lung cancer screening in China, improve the efficiency and effectiveness of lung cancer screening, and is the basis and guarantee of lung cancer prevention and control in China.
Lung Cancer Screening Standards in China
1 Scope
This document specifies the requirements related to the screening population, technology, process, quality control and the establishment of a screening resource base in the process of lung cancer screening.
This document applies to lung cancer screening conducted by medical institutions at all levels nationwide.
2 Normative References
The contents of the following documents constitute essential provisions of this document through normative references in the text. Among them, the reference document with the date, only the version corresponding to the date applies to this document; the reference document without the date, its latest version (including all the revision sheets) applies to this document.
GB/T 37864-2019 General requirements for the quality and capacity of biological sample repositories
T/CPMA 002-2019 Technical specifications for long-term follow-up of endpoint events in large population cohorts
T/CPMA 001-2018 Technical Specification for Data Processing of Large Population Cohort Studies
3 Abbreviations
The following abbreviations apply to this document.
DICOM: Digital imaging and communications in medicine (Digital imaging and communications in medicine)
LDCT: low-dose computed tomography (low-dose spiral CT)
MIP: maximum density projection (Maximum intensity projection)
MPR: Multi-planar reformation (MPR)
PACS: Picture archiving and communication systems (Picture archiving and communication systems)
PET-CT: Positron emission tomography- computed tomography (PET-CT)
VR: Volume rendering (VR)
4 Screening populations
Screening for lung cancer should be performed in a population at high risk for lung cancer. People at high risk for lung cancer are between (50 and 74) years of age and meet at least one of the following criteria.
a) Have smoked for not less than 30 (pack-years), including having smoked for not less than 30 (pack-years) but quit for less than 15 years.
b) Have lived with or worked in the same room as a) Passive smoking for more than 20 years.
c) Have chronic obstructive pulmonary disease (COPD).
d) Have a history of occupational exposure for not less than one year, including exposure to asbestos, radon, beryllium, chromium, cadmium, silica, soot and soot.
e) Have a first-degree relative with a confirmed diagnosis of lung cancer.
Note 1: Number of pack-years of smoking = number of packs smoked per day (20 packs per day) x number of years of smoking
Note 2: First-degree relatives refer to parents, children and siblings (same parents)
5 Screening TechniquesLung cancer screening should be performed with low-dose spiral CT (LDCT) and should not be performed with chest x-ray.
6 Screening process (see Appendix A)
6.1 Informed Consent
6.1.1 All screening participants should sign the informed consent form on a voluntary basis.
6.1.2 The content of the informed consent form should include, at a minimum
a) The purpose of the screening.
b) the significance of the screening.
c) the screening process.
d) the possible benefits and risks of participating in the screening.
e) the cost of the screening.
f) the principles of confidentiality and voluntariness
g) Signature and date.
6.2 Questionnaires
All screening participants should complete the lung cancer risk assessment questionnaire, which is included in Appendix B.
6.3 Risk Assessment
6.3.1 Risk assessment of screening participants is based on the results of the questionnaire.
6.3.2 The risk assessment can be conducted at a medical institution or through information technology for residents to provide a self-assessment service with necessary consultation and answers from the medical institution staff.
6.3.3 Personnel responsible for assessing or interpreting assessment results should be trained in lung cancer screening-related expertise before taking up their duties.
6.4 LDCT screening6.4.1 Implement LDCT screening for those whose risk assessment is high risk for lung cancer.
6.4.2 Healthcare institutions undertaking lung cancer screening should meet the following requirements.
a) Have lung cancer screening, diagnosis and/or treatment capabilities.
b) It is desirable to use multi-row spiral CT with 16 rows and above, with regular maintenance and calibration by dedicated personnel.
6.4.3 Screening is done by multidisciplinary staff, including physicians and staff from relevant disciplines such as imaging, respiratory medicine, thoracic surgery, oncology, laboratory and pathology.
6.4.4 LDCT scans should be performed in accordance with the following regulations.
a) The patient shall lie supine with hands up and take a single breath-hold scan at the end of inspiration.
b) The scan should be from the lung apex to the level of the tip of the posterior rib diaphragm angle (including the whole lung and both chest walls, and in female subjects, the whole breast).
c) Spiral scanning mode with a pitch setting of no greater than 1 and a frame rotation time of no greater than 0.8 s. The shortest scan time of the device is preferred, and the scan matrix setting should be no less than 512 x 512.
d) Scanning parameters of 120 kVp, (30-50) mAs may be used for those without iterative reconstruction techniques; those with new generation iterative reconstruction techniques may use (100-120) kVp, less than 30 mAs as scanning parameters.
e) Reconstruction with lung algorithm and standard algorithm, or only with standard algorithm, the reconstruction layer thickness between (1.00~1.25) mm is more appropriate. If the reconstructed layer thickness is between (1.00 and 1.25) mm, the reconstruction interval should not be greater than 80% of the layer thickness; if the reconstructed layer thickness is not greater than 0.625 mm, reconstruction without interval is possible.
f) It is advisable to turn on the “dose report” function when scanning.
6.4.5 LDCT reading shall comply with the following regulations.
a) Use DICOM format, read films at workstations or PACS, and use professional monitors.
b) Use lung windows with window width (1500-1600) HU and window position (-650-600) HU and mediastinal windows with window width (350-380) HU and window position (25-40) HU to read films separately.
c) Multiplanar reorganization (MPR) and maximum density projection (MIP) are used to view the morphologic features of pulmonary nodules in cross-sectional and MPR coronal and sagittal planes in multiple directions.
6.4.6 Nodule analysis and documentation should be in accordance with the following provisions.
a) The use of mean diameters is desirable.
b) Label the sequence and layer number where the nodule is located, report the complete lung nodule site, density, size, morphology, etc., and give recommendations for follow-up (including specific follow-up intervals).
c) Follow-up CT requires comparison of nodal changes in the same display orientation (cross-sectional or coronal or sagittal).
d) Concurrent measurement of nodal volumes to calculate nodal multiplication times is desirable.
e) It is desirable to also record other abnormalities such as emphysema, other lung diseases such as pulmonary fibrosis, coronary artery calcification and other abnormal findings within the scan.
6.4.7 Measurement of the solid component of partially solid nodules can be done by mean diameter and volume measurement.
Note 1: For mean diameter, measure the sum of the maximum longest diameter and the longest shortest diameter perpendicular to the maximum longest diameter (maximum shortest diameter) of the solid portion of the nodule divided by 2
Note 2: For volume measurement, the CT threshold range was selected for solid component separation in volumetric reproduction (VR) image reconstruction, and volume was measured using volumetric software
6.5 Outcome management and follow-up6.5.1 Baseline screening
Management and follow-up of baseline screening results should be in accordance with the following (see Figure C.1 in Appendix C).
6.5.1.1 If no intrapulmonary non-calcified nodules are detected (negative), proceed to the next year of screening.
6.5.1.2 Non-solid nodules average diameter <8.0 mm or solid nodules/partial solid nodules with a solid component <6.0 mm average diameter detected, then proceed to the next year of screening.
6.5.1.3 If the average diameter of the solid nodules or partially solid nodules with a solid component is not less than 6.0 mm and less than 15.0 mm, or the average diameter of non-solid nodules is not less than 8.0 mm and less than 15.0 mm, it is appropriate to review them after 3 months; for those solid nodules or partially solid nodules with definite malignant features in the opinion of the imaging physician, a multidisciplinary consultation is appropriate. The management and follow-up after 3 months will be based on the following conditions.
a) if the nodule has increased in size, a multidisciplinary consultation should be performed and the decision to perform clinical intervention should be based on the consultation.
b) If there is no change in the nodule, the nodule will be screened in the next year.
6.5.1.4 For detected solid nodules, solid components of partially solid nodules, or non-solid nodules with an average diameter of not less than 15.0 mm, the following two options are appropriate:a) Review 1 month after anti-inflammatory therapy or 1 month without anti-inflammatory therapy, and management and follow-up at the time of review according to
1) complete nodule resorption, then proceed to the next annual screening.
2) If the nodule is partially resolved, it is advisable to review it after 3 months. If the nodule is partially resolved and does not increase in size again, the patient will be screened the following year; if the nodule is partially resolved and increases in size again, a multidisciplinary consultation will be held to determine whether clinical intervention should be performed.
3) if the nodule does not shrink, a multidisciplinary consultation is appropriate and the decision to perform clinical intervention or to reexamine in (3-6) months is based on the consultation’s opinion.
b) Solid and partially solid nodules for biopsy or PET-CT, with management and follow-up according to
1) Positive, where a multidisciplinary consultation is appropriate and the decision to perform clinical intervention is based on the consultation’s opinion.
2) Negative or indeterminate mass, it is advisable to review after 3 months. If the nodule remains unchanged or increases in size at the time of review, a multidisciplinary consultation should be conducted to decide whether to perform clinical interventions based on the consultation; if the nodule decreases in size, the patient should proceed to the next year’s screening.
6.5.1.5 Suspected airway pathology, such as lumen occlusion, lumen narrowing, wall irregularities and wall thickening; abnormal soft tissue shadow in the hilum in close relationship with the bronchus; suspected obstructive inflammation, pulmonary atelectasis and bronchial mucus plug, etc., sputum cytology or fiberoptic bronchoscopy is appropriate and management and follow-up is based on
a) Positive, multidisciplinary consultation is appropriate and the decision to perform clinical intervention is based on the opinion of the consultation.
b) Negative, proceed to next year’s screening.
6.5.1.6 The principles of management of multiple pulmonary nodules are based on the principles of management of the most severe of these lesions.
6.5.2 Annual screening
The management and follow-up of annual screening results should be in accordance with the following (see Figure C.2 in Appendix C).
6.5.2.1 No intrapulmonary non-calcified nodules are detected (negative) or nodules do not grow, then proceed to the next year of screening.
6.5.2.2 An increase in the size or solid component of a pre-existing nodule makes it appropriate to consider clinical intervention.
6.5.2.3 For newly identified airway lesions, sputum cytology or fiberoptic bronchoscopy is appropriate, and management and follow-up are based on
a) Positive, multidisciplinary consultation is appropriate, and clinical intervention is decided based on the consultation opinion.
b) Negative, proceed to next year’s screening.
6.5.2.4 New non-calcified nodules with a mean diameter greater than 3.0 mm should be reviewed after 3 months of anti-inflammatory treatment or after 3 months without anti-inflammatory treatment.
a) complete nodule resorption, then proceed to the next annual screening.
b) If the nodule is partially resorbed, it is advisable to review it after 6 months, and the management and follow-up will be based on the following conditions at the time of review.
1) if the nodule is partially resolved and does not increase in size again, then proceed to the next annual screening.
2) partial nodule resorption followed by enlargement, clinical intervention should be considered.
c) if the nodule increases in size, clinical intervention should be considered.
6.5.2.5 If a new non-calcified nodule is found and the mean diameter of the nodule is not greater than 3.0 mm, it is appropriate to review the nodule after 6 months. The review should be handled and followed up according to the following conditions.
a) if the nodule does not increase in size, proceed to the next year of screening.
b) nodule enlargement, clinical intervention should be considered.
Note 1: Non-solid nodules refer to pure ground glass density nodules
Note 2: Nodule enlargement refers to a diameter line increase of not less than 2.0 mm
Note 3: Positive PET-CT examination refers to increased metabolism and higher radioactivity uptake than the lung background
Note 4: Positive sputum cytology means suspicious malignant cells are found in the sputum
Note 5: Positive fiberoptic bronchoscopy refers to bronchoscopic findings of neoplasia, mucosal abnormalities, or sampling results suspicious or suggestive of tumor
7 Quality control
7.1 The following measures are appropriate for quality control of LDCT scans.
a) Training screening subjects to hold their breath prior to scanning.
b) Deposit all images in DICOM format to PACS.
7.2 The following measures are desirable for quality control of LDCT screening results.
a) Each screening report should be issued by an imaging physician with the title of attending or above.
b) For cases with suspected lung cancer or “malignant lesions”, detected intrapulmonary nodules of not less than 15.0 mm, or airway lesions requiring bronchoscopy and further tests such as puncture biopsy, at least one imaging physician with associate or full senior title should be involved.
c) When invasive diagnostics (e.g. bronchoscopy, percutaneous lung aspiration biopsy, etc.) and open-heart surgery are required, the images are discussed by two or more imaging physicians with associate or full senior title and the case is brought to the multidisciplinary expert group for discussion.
7.3 Periodically, 100% of cases with suspected lung cancer or “malignant lesions”, nodules no smaller than 15.0 mm, or airway lesions requiring bronchoscopy will be reviewed by an associate or senior imaging physician, and 1% of other cases will be randomly selected.
7.4 Quality control of screening subjects at follow-up should refer to Section 7 “Quality Control and Evaluation” in T/CPMA 002-2019.
8 Screening Resource Library
Where available, a lung cancer screening resource bank should be established, which should include a screening database, an imaging database, and a biospecimen bank. It is appropriate to establish the following requirements.
a) The screening database should include risk assessment data, LDCT screening data, clinical diagnosis and treatment data, and follow-up data. The type of data and privacy protection should refer to the fourth part of T/CPMA 001-2018 “Privacy Protection of Data from Large Cohort Studies”.
b) Screening LDCT images should be stored in DICOM format in the appropriate image repository; LDCT images should include 5 mm thick conventional images, (1.00-1.25) mm thin layer images, and “dose report” images.
c) For screening participants, it is appropriate to collect and store blood samples. If a biopsy is performed, it is advisable to keep the tissue sample, etc. The collection, transport and storage of specimens should refer to the requirements in GB/T 37864-2019.
Appendix A
(informative)
Lung cancer screening processThe flow of lung cancer screening is given in Figure A.1.

Figure A.1 Lung cancer screening process
# of pack-years of smoking = # of packs smoked per day (20 packs per day) x # of years of smoking
#first-degree relatives refer to parents, children, and siblings(same as parents)
Appendix B
(informative)
Lung Cancer Risk Assessment QuestionnaireLung Cancer Risk Assessment Questionnaire
Name: ____________________ Sex: 1. Male 2. Female
Date of birth: _______ ______ _______ (please fill in the solar birthday)
National origin: ________ province ______ city _______ county (district)
Ethnicity: 1. Han Chinese 2. Mongolian 3. Hui 4. Manchu 5. Zhuang < strong>6. Uyghur 7. Kazakh 8. Other, please specify ________
ID number: ________________________________
Personal contact number: __________________________ (mobile)
Emergency contact phone number: __________________________ (mobile)
Permanent address: ________________________________________________________________________________
Workplace: ________________________________________________________________________________
(informative)
Lung Cancer Risk Assessment QuestionnaireLung Cancer Risk Assessment Questionnaire
Name: ____________________ Sex: 1. Male 2. Female
Date of birth: _______ ______ _______ (please fill in the solar birthday)
National origin: ________ province ______ city _______ county (district)
Ethnicity: 1. Han Chinese 2. Mongolian 3. Hui 4. Manchu 5. Zhuang < strong>6. Uyghur 7. Kazakh 8. Other, please specify ________
ID number: ________________________________
Personal contact number: __________________________ (mobile)
Emergency contact phone number: __________________________ (mobile)
Permanent address: ________________________________________________________________________________
Workplace: ________________________________________________________________________________
| A. Smoking status | |
| A. | A1. Do you smoke (defined as smoking if you smoke more than one cigarette a day for more than 6 months continuously or cumulatively)? 0. no, never smoked (skip to B1) 1. yes, currently still smoking 2. used to smoke, now quit |
| A1.1. | A1.2. If you still smoke or have smoked, how many cigarettes per day (1 tael of tobacco ≈ 50 cigarettes)? |
| A1.3. If you still smoke or have smoked, how long have you smoked in total, minus the number of years you have quit smoking? | |
| B1 A1.4. | B1 A1.4. If you currently quit smoking, how long has this quit lasted? |
| B. | B. Passive smoking status |
| B1. For nonsmokers, have you lived with a family member who smokes for more than 20 years? 0. no (skip to B2) 1. yes | |
| B2. For non-smokers, has the family worked in the same room with a co-worker who smokes for more than 20 years? 0. No (skip to C1) 1. Yes |
B2.2. If yes, has the colleague quit smoking for less than 15 years? 0. no 1. yes
B2.3. How many cigarettes does this colleague smoke on average per day?
B2.4. How many years has this coworker smoked in total, minus the number of years he or she has quit?
.
0. no (skip to E1) 1. yes
D1.1. Occupational exposure to what hazardous substances (multiple choice)?
1. asbestos
2. radon, beryllium, chromium, cadmium, silicon
3. soot and soot ash
4. other, please specify
Signature of person completing: ________________
Date filled in:________Year_______Month________Day
Appendix C
(informative)
Outcome management and follow-up
The management and follow-up protocols for baseline and annual screening results are given in Figures C.1 and C.2.![]()
Figure C.1 Management and follow-up of baseline screening results
S (Solid nodule): solid nodule; PS (Part-solid nodule): partially solid nodule; NS (Non-solid nodule): non-solid nodule (pure ground glass density nodule)
*: solid nodule or solid component of a partially solid nodule; #: positive means increased metabolism (radioactive uptake above the lung background); ☨: nodule enlargement means an increase in diameter of not less than 2.0 mm; ★: positive sputum cytology means suspicious malignant cells found in sputum, positive fiberoptic bronchoscopy means new organisms seen on bronchoscopy, mucosal abnormalities or sampling results suspicious or suggest tumor
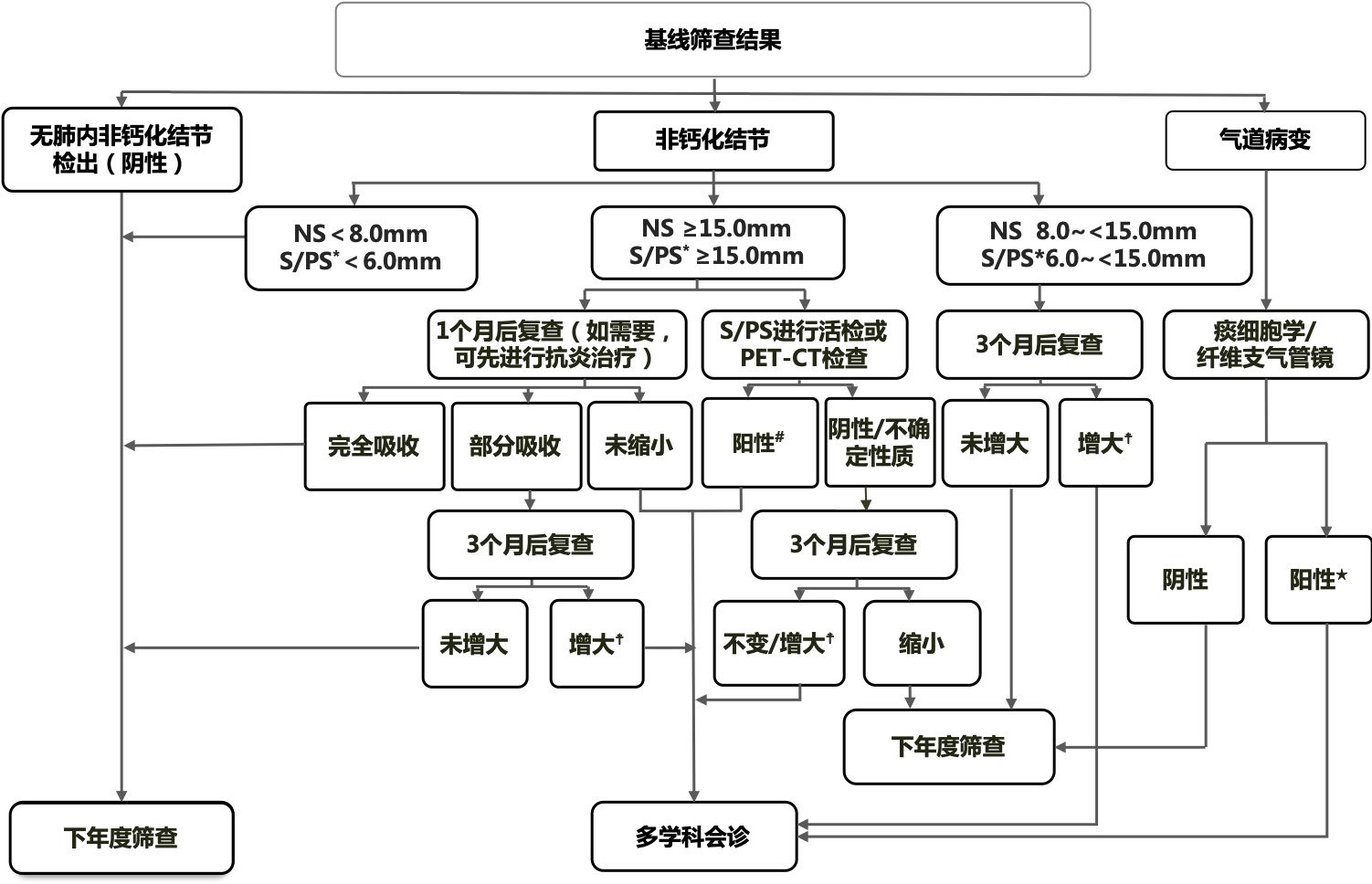
Figure C.2 Annual screening results management and follow-up
*: positive sputum cytology means suspicious malignant cells were found in sputum, positive fiberoptic bronchoscopy means new organisms, mucosal abnormalities or sampling results suspected or suggestive of tumor were seen on bronchoscopy; #: nodule enlargement means diameter line enlargement not less than 2.0 mm