According to the 2015 China Cancer Statistics, lung cancer is the cancer with the highest number of incidences and also the highest number of deaths in China. The incidence of lung cancer in China is more than 1/3 of the global total, even though it accounts for 1/5 of the global population. worse, the incidence trend shows that the incidence of lung cancer in China is still increasing, and the incidence of certain cancers is related to ethnicity, for example, melanoma is more prevalent in whites. So, is lung cancer related to ethnicity? With the high incidence of lung cancer in China, are Chinese people more likely to get lung cancer?
Chinese are not more likely to develop lung cancer than other ethnic groups
To answer this question, we compared the incidence of lung cancer among Chinese Americans with other ethnic groups.
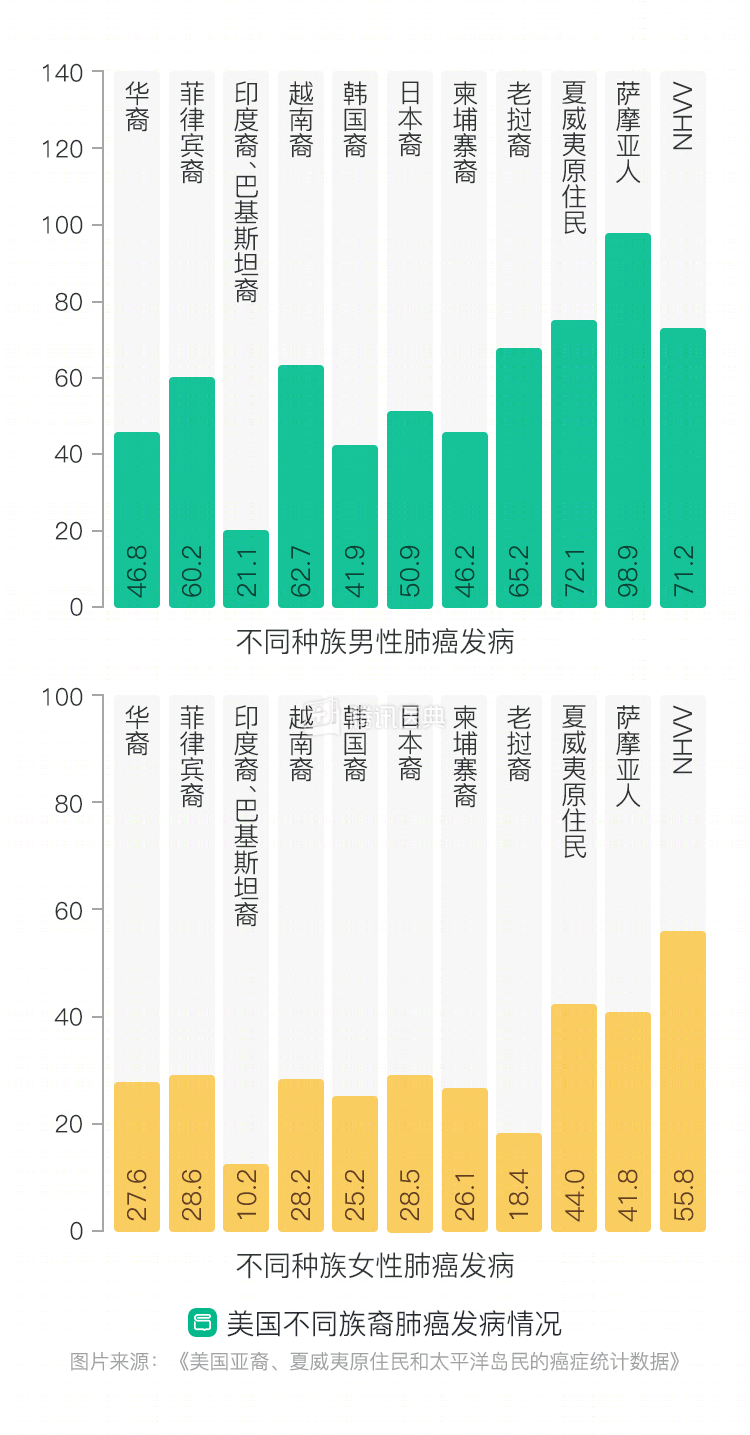
According to the Chinese data in Cancer Statistics for Asian Americans, Native Hawaiians, and Pacific Islanders, there are 744,000 new cases of lung cancer each year, which is in the middle of the range of lung cancer incidence rates among Asian Americans (Indian, Cambodian, Filipino, Chinese, Japanese, Korean, Pakistani, and Vietnamese, among others).
And in the Centers for Disease Control and Prevention (CDC) data, Asians, including Chinese (Figure A/PI), do not have significantly higher rates of lung cancer compared to whites, African Americans, Hispanics, Indians/Alaska Natives, etc.
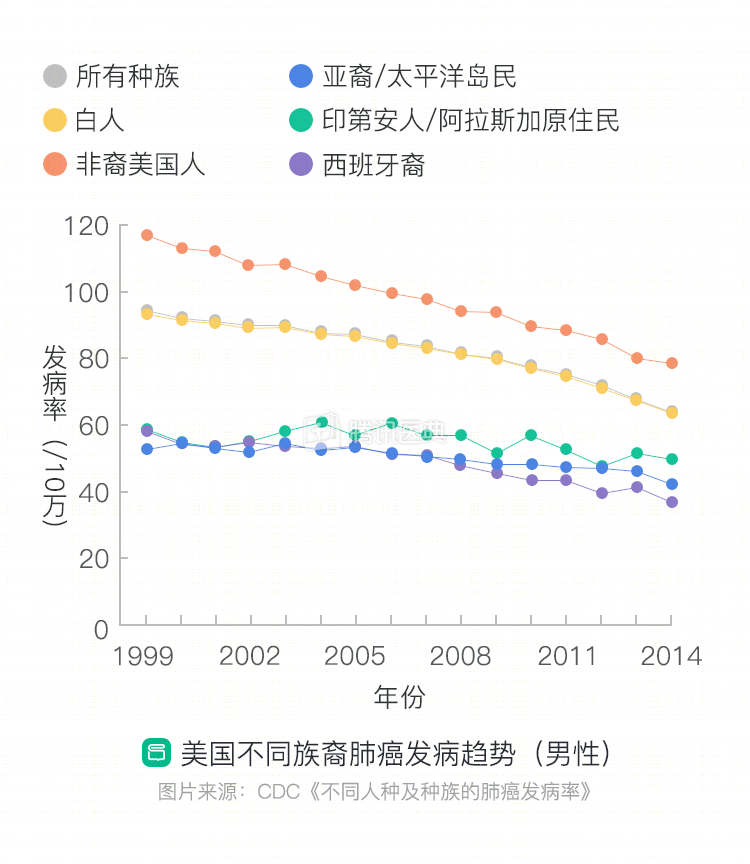
In summary, we can conclude that – Chinese are not more likely to develop lung cancer than other ethnic groups.
Lung cancer in Chinese has a higher rate of EGFR mutations
There are multiple pathological types of lung cancer, and the treatment options and prognosis for different types of lung cancer vary. In clinical practice, physicians primarily use pathological typing, disease staging, and molecular genetics (mainly gene mutations) to develop treatment plans. The rate of EGFR mutations is significantly higher in Asians compared to European and American populations.
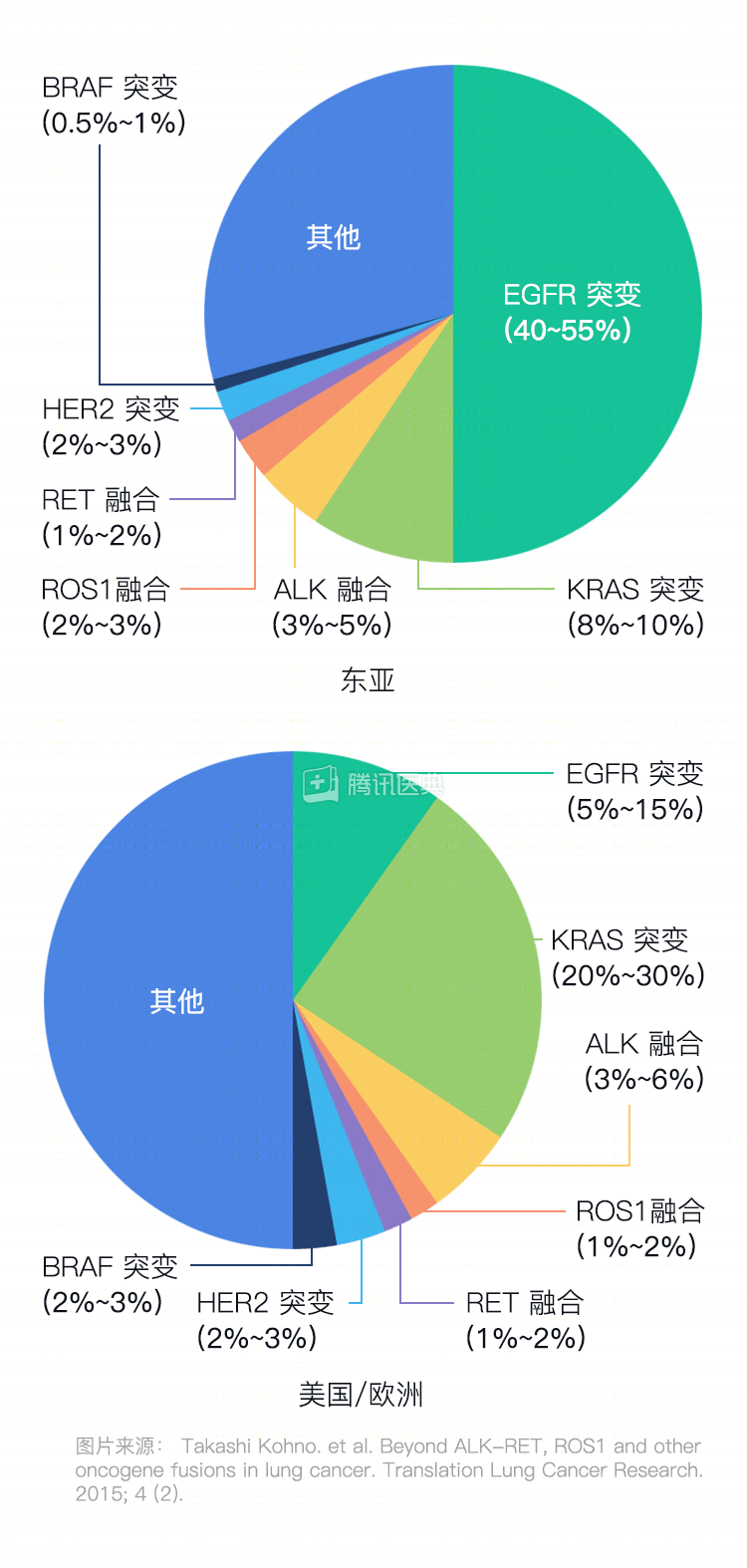
The graph above (left) lists the incidence of common mutations in Asian patients. Compared to the European and American populations (above, right), the mutations in Asians are markedly different
Among them, the rate of mutations in the epidermal growth factor receptor (EGFR), a gene that controls the growth of many cells, is nearly 50%. It is responsible for the healing of wounds in our daily lives. The EGFR gene is mutated, and it stimulates endless cell growth, which eventually leads to cancer.
Epidemiological surveys have shown that even among Chinese patients, the rate of EGFR mutations varies by population: higher in women than in men, higher in nonsmokers than in smokers, and higher in adenocarcinoma.
Fortunately, three generations of EGFR-tyrosine kinase inhibitors (TKI) have been developed, which significantly prolong the survival of such patients.
In summary, EGFR mutations are significantly more common in Asian lung cancers than in Europe and the United States, and effective targeted agents can prolong patient survival.
The large number of smokers makes lung cancer more difficult to control in Chinese
Smoking is the most common cause of lung cancer (smoking increases the risk of lung cancer by 151%, while secondhand smoke is a major cause of disease in nonsmokers).
According to data published by The Lancet in 2015, China has more than a third of the world’s smokers and is the world’s leading smoker, with more smokers than the 29 countries ranked 2nd to 30th combined. At this level, it is projected that by 2050, about 3 million people could die each year from smoking-related diseases in China.
The 2010 National Survey of National Smoking Prevalence and Patterns in China [officially published in the British Medical Journal (BMJ) in 2016] showed that 62.4% of adult Chinese men smoke, with a higher prevalence of smoking among rural men than urban men (63.9% vs 58.4%). Among current smokers, only 17.3% intend to quit. Compared with a similar survey in 1996, the smoking population was significantly larger and began smoking at an earlier age.
There is no doubt that the widespread tobacco epidemic is making our smoking-related disease challenges even more severe – leading to more lung cancers, and significantly more squamous lung cancers among smokers than nonsmokers, with lower rates of mutations such as EGFR and no targeted drug therapy, making clinical treatment more difficult.
Lung cancer remains the number one killer of tumor patients in China
Lung cancer is the leading cause of death among oncology patients in China, with a high estimated number of lung cancer deaths in 2015 of 610,200 cases (men: 432,400, women: 177,800) (1). Compared with the incidence rate, the mortality rate of lung cancer patients is as high as 84.9% (43.24/50.93) for men and up to 79.4% (17.78/22.40) for women, with a combined mortality rate of 83.2% (61.02/73.33) for both sexes; where the numbers in parentheses are in “10,000 cases”.
Inquiry into the reasons for this may include:
① Inadequate tobacco control, leading to a continued rise in incidence;
② Insufficient prevalence of screening, with many patients clinically detected at advanced stages;
③ Unequal distribution of medical resources, varying levels of medical care, and the lack of clinical guidelines and norms based on the disease characteristics of our patients;
④ Poor accessibility of new drugs that can provide effective treatment for lung cancer, etc.
Happily, these issues have gradually gained more and more attention, and now China’s tobacco control policies are being strengthened and early screening with low-dose spiral CT is becoming popular. As we learn more about the characteristics of lung cancer in China, researchers are increasingly exploring the most appropriate treatment for lung cancer in China, and these explorations will provide evidence-based evidence for the development of clinical guidelines and norms.
I hope that in the future, we will see the incidence and mortality rates of lung cancer in China decline as they have in Europe and the United States.
Co-reviewed by: Dr. Haiyan Tu, Deputy Chief Physician, Guangdong Provincial People’s Hospital, Guangdong Lung Cancer Institute Dr. Yue-Li Sun, Dr. Jiangtao Cheng