- Tumors can become “resistant” to drugs after multiple “encounters” with them during chemotherapy, resulting in a decrease in effectiveness, a phenomenon called “drug resistance”. Some tumor cells are more “resistant” and develop multiple drug resistance, which is a major reason why chemotherapy is not effective or fails.
The development of multi-drug resistance to chemotherapy is a major cause of poor or failed chemotherapy.
After chemotherapy resistance occurs, it is usually addressed by combining or changing chemotherapy regimens, combining radiation therapy, anti-vascular therapy, biologic therapy, or re-biopsy to try targeted therapy.
Chemo “fails” after a period of time
A tumor that has been “treated” with a drug many times during chemotherapy may become “resistant” to the drug, causing it to become less effective, a phenomenon called “drug resistance.
In general, drug resistance is considered when the disease progresses after a short period of treatment or after a few cycles, or when the disease worsens during a break in the chemotherapy cycle. Once drug resistance occurs, treatment is also declared a failure.
Why does drug resistance occur?
This is because of genetic changes in daughter cells during multiple divisions and proliferation of tumors that affect the sensitivity of the tumor to the drug; combined with the tumor’s own ability to evolve, it is almost inevitable that chemoresistance will occur, it is just a matter of time.
Not only do tumors become resistant to one drug, but they also become “cross-resistant” to drugs with similar structure and function, such as cisplatin and carboplatin. Some tumor cells are even more “aggressive,” developing resistance not only to the chemotherapy drugs they have been exposed to, but also to other drugs with unrelated structures and different mechanisms of action, resulting in multidrug resistance (MDR). This is a major cause of poor chemotherapy outcomes or failure.
How to deal with chemoresistance?
After tumor resistance, your doctor may choose to respond as follows, so please understand and work with your doctor:
Combining or changing chemotherapy regimens
Combining chemotherapy with other drugs that have a different mechanism of action and do not cross-resist is called “rescue chemotherapy,” such as drugs that act on dormant, rather than rapidly proliferating, cells. This is often an easy and effective route.
Combining other treatments
Doctors may consider combining other therapies, such as radiation therapy and anti-vascular therapy, to work together to combat drug resistance.
Combining biological therapies
“Knock out” the chemo-resistant “target” and make the tumor sensitive to chemotherapy again.
Rebiopsy to see if there is a chance of using targeted therapy
For non-small cell lung cancer, a second biopsy can be taken for genetic testing to look for genes that can be targeted for targeted drug therapy.
At present, there is no perfect approach to chemotherapy resistance. Scientists have worked hard to find the right biomarkers to screen for “susceptibility” to chemotherapy, but the results of most of the relevant clinical trials have been unsatisfactory, and further research is expected.
Extended reading
Why do tumors become drug resistant?
Research has shown that tumors develop chemoresistance by multiple mechanisms involving various aspects of cell biology (such as proteins, enzymes, or parts of the cell structure), and as a result of multiple genes and steps working together.
The mechanisms of resistance that are currently “hot” in the professional community are shown in the figure below:
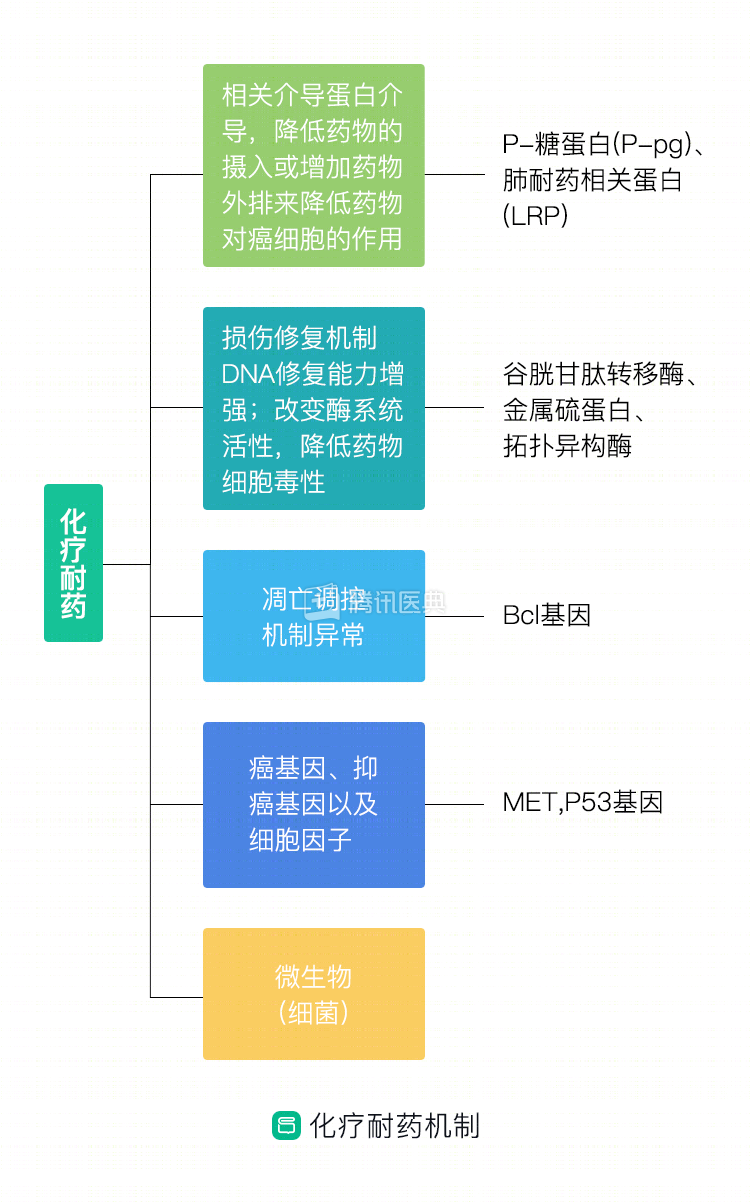
1. Decreased drug uptake or increased drug excretion, mediated by specific proteins, to reduce the effect of drugs on cancer cells;
2.
2. The tumor is damaged by the drug and has an increased ability to repair itself; in addition, the activity of the enzyme system is changed to reduce the cytotoxicity of the drug;
3. Abnormalities in the control mechanism of tumor apoptosis prevent cancer cells from “dying” normally;
4.
4. Regulation of oncogenes/oncogenes:
Oncogenes are a class of nucleotide sequences found in viral or cellular genomes, whose expression products can transform normal cells into malignant cells under certain conditions. We all have such genes in our cells, but they are not activated and are called proto- oncogene.
Oncogenes, also known as tumor suppressor genes, are found in normal cells and play a very important negative regulatory role in controlling cell growth, proliferation, and differentiation, with potential cancer suppressive effects. When mutations, deletions or inactivation of these genes occur, they can cause malignant transformation of cells and lead to tumorigenesis. The most studied oncogenes are P53 and Rb.
Oncogenes and oncogenes regulate each other to maintain the relative stability of cell growth. If oncogenes are the “growth gas pedals” that are difficult to control, then oncogenes are the “brakes” that inhibit the growth of malignant cells. For example, EFGR mutations, which are common in lung cancer, tend to have a good response rate to EGFR-targeted drugs, but the presence of Met amplification of the proto-oncogene can lead to resistance to targeted drugs.
5. Microbes are also relevant to the evolution of cancer, and gamma-transforming bacteria can cause chemoresistance by metabolizing and converting gemcitabine, a common chemotherapy drug for lung cancer, into an inactivated form.
Co-authors: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Yue-Li Sun Dr. Lun-Xi Peng