- More minimally invasive: Minimally invasive lung cancer surgery has evolved from the traditional three incisions to double-hole versus single-hole surgery. With the help of modern TV camera technology, only about 1 cm of observation hole is needed to see inside the body, while with the help of advanced surgical instruments, the operation can be basically completed through a 3-5 cm incision.
- More precision: Lobectomy is still the routine procedure for lung cancer surgery, which involves cutting off at least half of the left lung or 1/3 of the right lung, which is obviously more damaging. Usually a lobe contains 2 to 5 lung segments, and removing one lung segment is less invasive than removing the entire lobe, with more lung tissue remaining and more function preserved.
While there are a variety of treatments available for lung cancer, surgery remains the only treatment option that has a chance of curing the disease in early to mid-stage non-small cell lung cancer (NSCLC) and is the first treatment option that doctors consider.
I. Our lungs – a breathing tree
To understand lung cancer surgery, first understand the structural features of the lung.
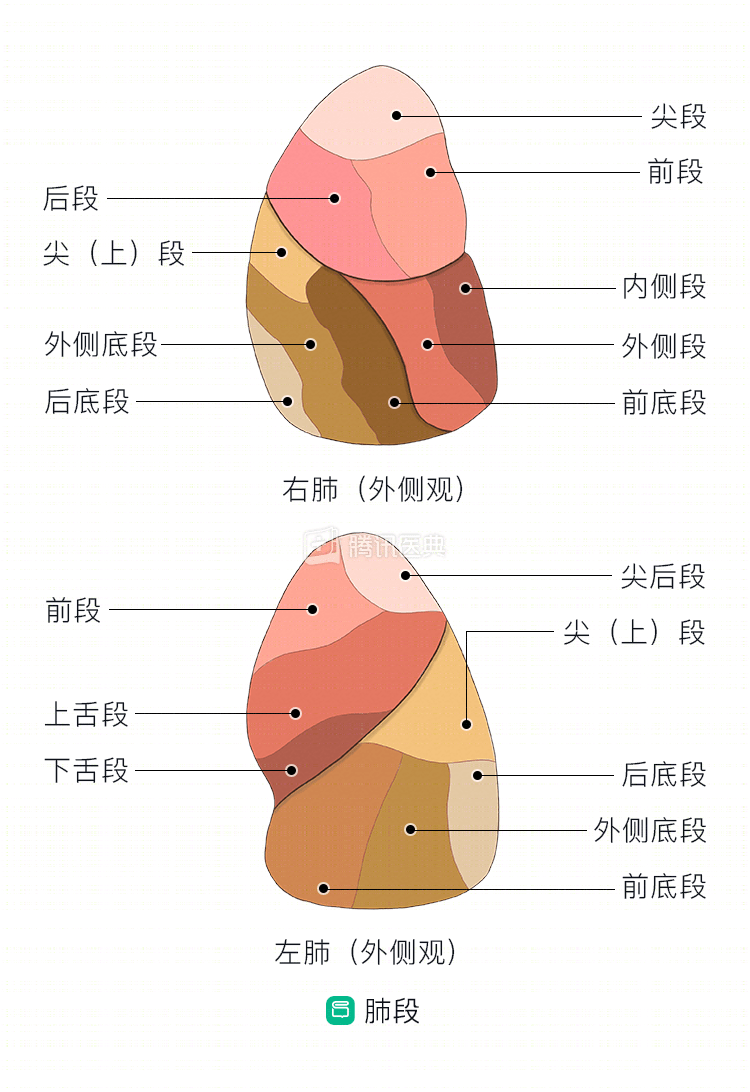
Our lungs are like a breathing “tree” that divides from the trachea into two “main bronchi” (primary), then into lobes (2 on the left and 3 on the right) and bronchi (secondary), and then into segments (8 on the left and 10 on the right). The bronchi (tertiary) become more and more subdivided (figure below). The term “lung segment” refers to a lung segment bronchus + its branches + the lung tissue to which it belongs.

The lung segments are wedge-shaped, with the base on the surface of the lung and the tip at the root. Each lung segment has a relatively independent blood supply system and bronchial branches, and thus can function as a relatively independent unit (Figure).
II. New trends in lung cancer surgery – more precise and minimally invasive
Traditional lung surgery is often intimidating. Many patients have images in their minds of doctors cutting through the chest wall, severing ribs, and operating in a bloody mess; after surgery, patients are put on ventilators, have all kinds of tubes inserted, and lie in the intensive care unit for many days before they can resume normal activities. This image even frightened some patients to resist the surgery, and unfortunately missed the best time for treatment.
In fact, this is already history. Under the concept of precision minimally invasive and rapid recovery, most lung cancer surgery patients can now be discharged within a week after surgery, or even on the day of surgery. The precision and minimally invasive nature of lung cancer surgery is reflected in two main areas.
1. Minimally invasive surgical approach
Video-assisted thoracoscopic surgery (VATS) was first used for lung cancer in 1994. With the help of modern television camera technology, only about a 1 cm viewing hole is needed to see inside the body, while the operation can be largely completed through a 3-5 cm incision with the help of advanced surgical instruments.
Many comparative studies between VATS and traditional open-heart surgery have been done in the professional community, showing that VATS is naturally more acceptable to patients and families because of its advantages of less trauma, less bleeding, less postoperative pain, less impairment of lung function, fewer postoperative complications, and faster recovery.
VATS has performed well while it continues to progress: from the traditional three incisions, it has gradually evolved into a double-hole versus single-hole procedure. The traditional 3 small-incision thoracoscopic procedure, in which the posterior axillary line incision is made, has several disadvantages:
(1) The incision here tends to bleed more because of the many layers of dorsal muscle and the rich blood supply;
(2) Damage to the muscles and nerves in this incision often results in significant pain and abnormal sensation and mild motor deficits;
(3) Excessive incisions can also be “psychological” for the patient.
The resulting “single-port procedure” eliminates the posterior axillary incision and extends the anterior axillary incision relative to the anterior axillary incision, with all operating instruments entering and exiting through a single port, solving these problems to some extent.
Of course, the single-port operation is not perfect: the instruments tend to interfere with each other, and if the lesion is close to the dorsal side or near the diaphragm and cannot be adequately visualized, it can make the operation difficult and increase the operative time. In addition, severe tissue adhesions and intraoperative bleeding may not be managed. This also raises the “bar” for the operating surgeon, and improper handling can easily result in damage to surrounding organs and tissues.
Related reading
.
2. More precise extent of resection
At present, lobectomy is still the routine procedure for lung cancer surgery, which is equivalent to cutting off at least half of the left lung or 1/3 of the right lung, which is obviously more damaging. Usually a lobe contains 2 to 5 lung segments, and removal of one lung segment is less invasive than removal of the entire lobe, with more lung tissue remaining and more function preserved. And, as previously described, each lung segment is a relatively independent functional unit, and resection of a lung segment is anatomically feasible.
So, is it possible to remove only the diseased lung segment without cutting the lobe?
There has been a lot of professional research on this. On the one hand, for small nodules that meet certain criteria, it is possible to do a segmental lung resection instead of removing the entire lung lobe; on the other hand, for older, frail patients with lung cancer, or those with other cardiopulmonary disease, who may not tolerate lobectomy, it is possible to do a segmental lung resection instead.
Currently, the National Comprehensive Cancer Network (NCCN) guidelines for NSCLC recommend that “less than lobectomy” (segmental lung resection and wedge lung resection) be considered in the following situations:
- Poor lung function or other severe comorbidities that do not tolerate lobectomy;
- Nodules located in the peripheral parts of the lung, not larger than 2 cm in diameter, and meeting certain specific histological and imaging criteria.
Will “less than lobar” resection achieve the same long-term outcomes as lobectomy for early-stage lung cancer? This is still controversial, and several studies are underway to verify this. Until a definitive conclusion is reached, patients should communicate closely with their physicians and work with them to choose their surgical approach carefully.
In summary, “more precise and minimally invasive” lung cancer surgery has brought real benefits to many patients and will continue to be the direction of lung cancer surgery for some time to come.
Related reading:
Co-authors: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Zheng Shaopeng Dr. Huang Lu Yu Dr. Xia Jin