You may have heard of targeted therapies, which are more effective and have fewer side effects for the “right” patients than chemotherapy. So, who can use targeted therapy?
First, only patients with non-small cell lung cancer (NSCLC) can be considered for targeted therapy; small cell lung cancer (SCLC) generally cannot be used.
Secondly, it is important to check for “mutations”, which is the molecular typing of lung cancer. Only patients with specific mutations can choose the corresponding targeted drugs.
Finally, after resistance to targeted therapy occurs, doctors usually recommend molecular typing again to see if there are new “targets” to choose more effective targeted therapy.
Here’s what we know about molecular typing and how doctors choose treatment options based on typing.
Basics of molecular staging of lung cancer
1. Do all lung cancer patients need molecular staging?
.
No.
Currently, China’s guidelines recommend that patients with advanced NSCLC (whether initially diagnosed as advanced or early-stage patients evolving to advanced) undergo genetic testing, focusing on 3 loci: EGFR mutations, ALK fusions, and ROS-1 fusions. 2018 saw the release of new lung cancer guidelines, which also recommend that patients with early to mid-stage, hilar mediastinal lymph node metastases for non-squamous NSCLC patients to undergo EGFR mutation testing.
For patients with SCLC and early-stage NSCLC, molecular typing testing is not mandatory.
2. How is molecular staging of lung cancer done?
.
- The main techniques for detection of EGFR gene mutations are direct sequencing and the Amplification Refractory Mutation System (ARMS);
- The common detection methods for ALK fusion genes are Fluorescence in situ hybridization (FISH), immunohistochemistry (IHC) and Reverse transcription polymerase chain reaction (RT-PCR). polymerase chain reaction (RT-PCR);
- The ROS1 fusion gene is commonly detected by RT-PCR or FISH.
Of course, you don’t need to understand these complex techniques in detail, just that your doctor will recommend that you keep the tumor tissue for testing if you are eligible for the test.
3. How do I get a specimen for testing?
.
The “quality” of the tumor specimen determines the accuracy of the test results. Commonly used specimens include surgical resection specimens, biopsy specimens (fine needle aspiration, fiberoptic bronchoscopy biopsy), cytology specimens (malignant pleural fluid, pericardial effusion, bronchoscopic brushings), sputum, and blood specimens.
It is best to use fresh, tumor cell-rich specimens for genetic testing. When sufficient tissue specimens are not available or cannot be obtained, peripheral blood can be drawn to detect EGFR mutations. However, the technology for blood testing for ALK and ROS1 fusions is not yet mature.
Common Molecular Typing of Lung Cancer and Corresponding Treatments
EGFR
Patients with lung adenocarcinoma of Asian descent (including China) have a 40% to 50% positive rate for EGFR-sensitive mutations.
There are 4 main types of EGFR mutations: exon 19 deletion mutation (19DEL), exon 21 point mutation (21L858R), exon 18 point mutation, and exon 20 mutation. The first two are the most common, and patients with these two mutations are sensitive to EGFR-targeted drugs [scientifically known as EGFR-tyrosine kinase inhibitor (TKI)]. In addition, exon 18 G719X, exon 20 S768I and exon 21 L861Q mutations are also sensitive to targeted drugs, which are all “sensitive mutations”.
The T790M mutation in exon 20, however, is insensitive to first- and second-generation EGFR targeting agents and is a common cause of drug resistance during treatment.
For other types of mutations, we are currently unaware of their clinical significance.
How to treat EGFR mutation-positive advanced NSCLC? We summarize the presentation with the following diagram.
ALK fusion gene
How to treat ALK-positive advanced NSCLC? The following chart gives you a brief summary.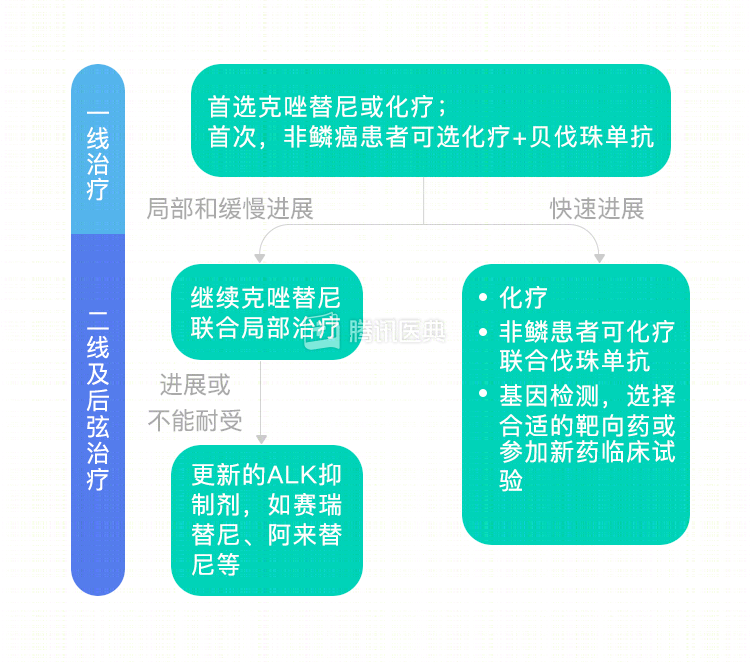
ROS1 fusion gene
ROS1-positive advanced NSCLC is effectively treated with crizotinib, and the 2018 edition of our lung cancer guidelines recommend first-line crizotinib or chemotherapy for these patients.
In addition to the three main loci mentioned above, patients with advanced NSCLC can also try immunotherapy, mainly PD-1 and PD-L1 inhibitor drugs. Currently approved for NSCLC treatment in the United States are Nivolumab (nabulizumab), Pembrolizumab (pablizumab), and Atezolizumab (atezolizumab). The first two are also available in China.
Co-reviewed by: Dr. Bai Xiaoyan, Guangdong Provincial People’s Hospital, Guangdong Lung Cancer Institute Dr. Gao Xin
Co-authors: Dr. Ma Yue, Department of Oncology, Renji Hospital, Shanghai Jiao Tong University