- Traditional radiotherapy techniques are flawed in that they can only roughly determine the general extent of the tumor and require multiple irradiations, which can cause irreversible damage to normal tumor surrounding tissues, especially radiation-sensitive vitals;
- The newer radiotherapy techniques include five types: “tailored” conformal radiotherapy (3D conformal radiotherapy, intensity modulated conformal radiotherapy), “surgery-like” high-dose stereotactic ablative radiotherapy, “multi-pronged “The company’s main products are the spiral tomotherapy system, intraoperative radiotherapy, and particle beam radiotherapy, which is a “targeted blast”.
“Radiotherapy” (radiation therapy), one of the “triad” of comprehensive lung cancer treatment, uses high-energy radiation to destroy the DNA, the genetic material of tumor cells, so that they lose their ability to regenerate.
However, conventional radiotherapy techniques use an “analog localizer” (note: a special x-ray machine that identifies and marks the site of irradiation for the patient) to determine the extent of irradiation, which is somewhat flawed and can only roughly determine the general extent of the tumor. In addition, conventional radiotherapy has a large irradiation area and requires multiple irradiations, which can cause irreversible damage to the normal tissues surrounding the tumor. If the tumor is surrounded by radiation-sensitive tissues and vital organs (e.g., heart, esophagus, etc.), the risk of conventional radiotherapy is even greater.
In recent years, radiation therapy for lung cancer has evolved dramatically, allowing it to be more “stable, accurate, and precise. Here is a brief overview of these new “highly sophisticated” radiotherapy weapons.
I. Conformal radiotherapy: precisely tailored to the tumor
.
Conformal radiotherapy, as the name implies, is a form of radiotherapy that fits the shape of the tumor and includes mainly three-dimensional conformal radiotherapy (3D-CRT) and intensity-modulated conformal radiotherapy (IMRT)[1]:
Three-dimensional conformal radiotherapy (3D-CRT), uses CT scans to obtain a three-dimensional structure of the tumor, from which the physician outlines the area to be focused on (radiotherapy target area) and the organs to be protected. The radiologist then designs the shape of the actual radiation area (radiation field) with the goal of ensuring that the high-dose radiation area wraps tightly around the target area from all sides, with less harm to surrounding normal tissue.
Intensity-modulated conformal radiotherapy ( IMRT), which evolved from 3D-CRT, meets both of the following conditions:
(1) the irradiation field is consistent with the shape of the lesion (target area) in the direction of irradiation;
(2) The dose is equal everywhere within the target area and on the surface, and the dose can be adjusted as needed at each radiation point (points within the radiation field).
What does this mean? To use an analogy, we know that most malignant tumors grow very irregularly, like a bumpy, oddly shaped rock. Conventional chemotherapy is like a flashlight shining a beam of light on this stone, with the part close to the light source being brighter and the distant part being darker. If you want the whole stone to receive the same intensity of light, then you need to finely adjust the intensity of light according to the surface of the stone and the distance. This is the basic concept of “intensity adjustment”.

In summary, 3D-CRT allows for more precise radiotherapy target areas and less damage to surrounding normal tissue. On this basis, IMRT can precisely adjust the radiation dose so that the tumor surface receives the same radiation intensity, the radiation distribution is more uniform and reasonable, and the treatment effect and the ability to protect the surrounding tissues are slightly better.
Which lung cancer patients are suitable for conformal radiotherapy? Although the overall use of 3D-CRT is gradually decreasing, it is still used more often in palliative radiotherapy (radiotherapy aimed not at curing the tumor, but at controlling pain and relieving symptoms) such as whole brain radiotherapy, or bone metastases. In contrast, IMRT is less damaging to normal tissues surrounding the tumor and is increasingly used in lung cancer, especially when there are many vital organs surrounding the tumor or when localized dose irradiation of specific areas is required, IMRT is preferred.
The Cancer Hospital of the Chinese Academy of Medical Sciences analyzed data from 652 Chinese lung cancer patients and showed that IMRT had higher local tumor control rates and longer patient survival compared to 3D-CRT, extending life expectancy by an average of nearly 4 months.
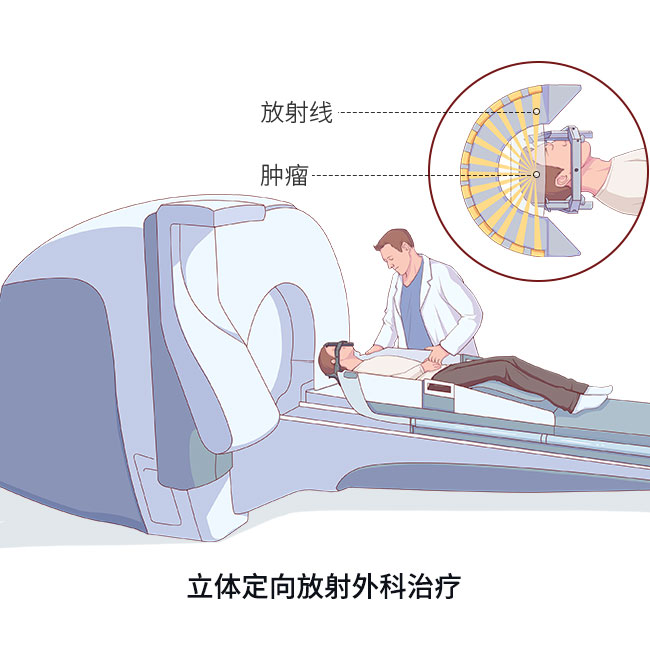
II. High-dose stereoscopic ablative radiotherapy: a sharp “light knife” comparable to surgery
High-dose stereotactic radiotherapy (SBRT) uses stereotactic technology to spatially localize the tumor to the millimeter with the help of fixation devices and computer calculations. Then, a single high-dose irradiation is used to precisely focus on the lesion (target area) and kill the tumor, potentially achieving a treatment effect similar to surgery, which can be understood as a sharp “light knife”.
Expert studies at MD Anderson Cancer Center have shown that high-dose SBRT can provide local control of early-stage lung cancer at rates comparable to surgery. Therefore, this single-dose, high-fraction radiotherapy regimen is also known as stereotactic ablative radiotherapy (SABR).
The advantages of high-dose SABR are:
(1) more precise localization, less radiation damage to normal tissue, and consequent reduction in side effects;
(2) high dose irradiation, which produces a stronger killing effect on tumors, even comparable to surgery;
(3) fewer irradiation sessions, resulting in shorter total radiotherapy time and less inconvenience and pain for patients.
SABR works so well and avoids the pain of surgery, is it appropriate for all lung cancer patients? Not really. The current professional opinion is that SABR should be considered only in the following situations:
(1) Most appropriate for SABR: Early-stage lung cancer that is isolated, has no metastases, and is less than 5 cm in diameter (less than 3 cm is better). Patients who meet these criteria and are inoperable, or unwilling to have surgery, are recommended for SABR;
(2) Conditions in which SABR can be considered: lung cancer with certain metastatic lesions, such as brain metastases, with less than 3 metastases and less than 3 cm in diameter, may be considered for SABR of the metastases to provide pain relief, kill the cancer cells, and control the development of the lesions.
Related reading:
III. Spiral tomotherapy system: multiple lesions, one solution
The spiral tomotherapy system (TOMO radiation therapy), commonly known as the “Tomo knife,” is brilliant in that it combines multiple technologies to irradiate multiple lesions simultaneously, greatly improving treatment efficiency.
1.
1. Radiation therapy while scanning:
TOMO radiotherapy combines spiral CT scanning with imaging accuracy of ±0.1 mm, allowing for scanning and radiotherapy at the same time, and 360° focused tomography to irradiate tumors.

2. Intelligent intensity modulation and conformability:
TOMO radiotherapy also features conventional linear gas pedal IMRT, image-guided radiotherapy (IGRT), and dose guided radiotherapy (DGRT).
It is very advantageous for lung cancers that require extra-long irradiation, or have a wide distribution of lesions. Specifically, for tumors with a longer irradiation range, such as whole brain and whole spinal cord irradiation, you can irradiate from head to toe without seams; and with a wider distribution of lesions such as multiple lesions throughout the body, you can irradiate all the lesions found at the same time, and you can ensure that different doses are given to different sites, with better treatment outcomes and shorter times.
To summarize, TOMO as a modality of intensity-modulated radiotherapy can be widely used in the treatment of all types of lung cancer and is more important for multiple lesions, but physicians should also be aware that simultaneous treatment of multiple lesions takes care to monitor the range of low-dose irradiation to the lung and the patient’s physical condition.
4. Intraoperative radiotherapy: consolidating the effect and “cleaning up the remaining damage”
Intraoperative radiotherapy (IORT), as the name implies, is a one-time high-dose irradiation of the original tumor growth (tumor bed), tumor tissues that may have been invaded by the tumor, or tumor tissues that could not be removed surgically, after surgical removal of the malignant tumor, in order to “clean up the loose ends.
The advantages are:
(1) In general, in external irradiation, the radiation must first pass through the normal tissues of the body before it can reach the lesion. The doctor can see the lesion “straight on”, pinpoint it, and narrow the scope of irradiation.
(2) Outside the treatment area, the radiation dose decays rapidly, thus maximizing the protection of surrounding normal tissue.
(3) One-stop operation for surgery and radiotherapy, saving the time between surgery and radiotherapy, as well as the time to re-plan and implement radiotherapy.
At present, IORT has been used extensively in breast cancer, but is still in its infancy in lung cancer. The professional community has reported in the literature that it is primarily used in acinar lung cancer, with better operational safety and efficacy, but more research is needed.
V. Particle beam radiotherapy: targeted blasts with minimal injury
To understand the “power” of different types of radiation, one needs to understand the concept of linear energy transfer (LET), which refers to the efficiency of energy transfer along the path of ionizing radiation. For the same absorbed dose, the higher the LET, the more concentrated the energy produced and the stronger the biological effects.
The particles currently used in oncology radiation therapy are: neutrons, protons, alpha particles, and charged heavy ions such as carbon and neon ions [“heavy ion” in the professional world means a nucleus with a mass number greater than 4 (helium)].
Protons and alpha particles are charged particles with low LET; neutrons are not charged particles but have high LET biology; and charged heavy ions such as carbon ions and neon ions have high LET biology, and carbon ions are now commonly used in clinical practice.
Related reading:
What is so “great” about “charged heavy ions”? We know that the X-rays, electron beams, gamma rays, etc. most commonly used in radiotherapy have a disadvantage: they decay after they enter the body. Before reaching the tumor, they kill normal tissue along the way. If the lesion is deep, the normal tissues will be exposed to higher doses along the way when the energy reaches the tumor. When the “heavy ion” beam passes through human tissue, it gradually releases energy, and the effect increases rather than decreases, reaching a certain depth when the energy is released and rapidly peaks, then decreases rapidly (below). The Bragg peak is one of the advantages of high LET rays. The proton beam is unique in that it is not a high LET ray, but it does have a distinct “Bragg peak”.
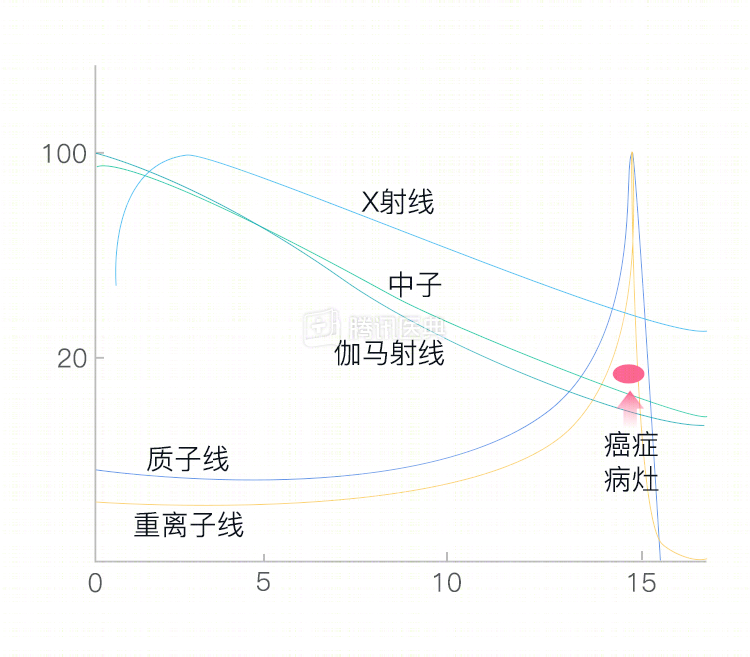
By adjusting the depth to the Bragg peak effect unique to protons and heavy ions, clinical scientists have been able to release the highest dose (Bragg peak) exactly in the tumor lesion with little additional irradiation to the normal tissue surrounding the tumor, similar to a “targeted blast”, which rarely hurts as long as it is well positioned. The tumor is not a tumor.
Currently, medical centers with proton and heavy ion radiotherapy facilities are still primarily located in North America and Europe. Because the gas pedals are bulky, expensive, and time-consuming to treat, their clinical use is still immature, and only a few institutions are currently using them.
As you can see above, chemotherapy for lung cancer may not seem like a dramatic breakthrough, but there are many “new weapons” that are making our fight against tumors more precise and efficient.
Co-authors: Dr. Zhiyong Chen, Guangdong Provincial People’s Hospital, Guangdong Lung Cancer Institute Dr. Jiatao Zhang