For patients with lung cancer, there is nothing more to look forward to than a cancer cure. In fact, even when treatment is effective, most lung cancers recur within 5 years of diagnosis. A survey by the National Cancer Institute (NCI) showed that stage IA and IB lung cancer recurs in about one-third of patients, and in about two-thirds of patients with stage IIA, IIB, or IIIA.
So, why is lung cancer prone to recurrence and how do you recognize recurrence?
What is a recurrence of lung cancer?
Cancer is treated and the lump subsides and the cancer cells are undetectable. But then the cancer is found again in the body, and the pathology is the same as before.
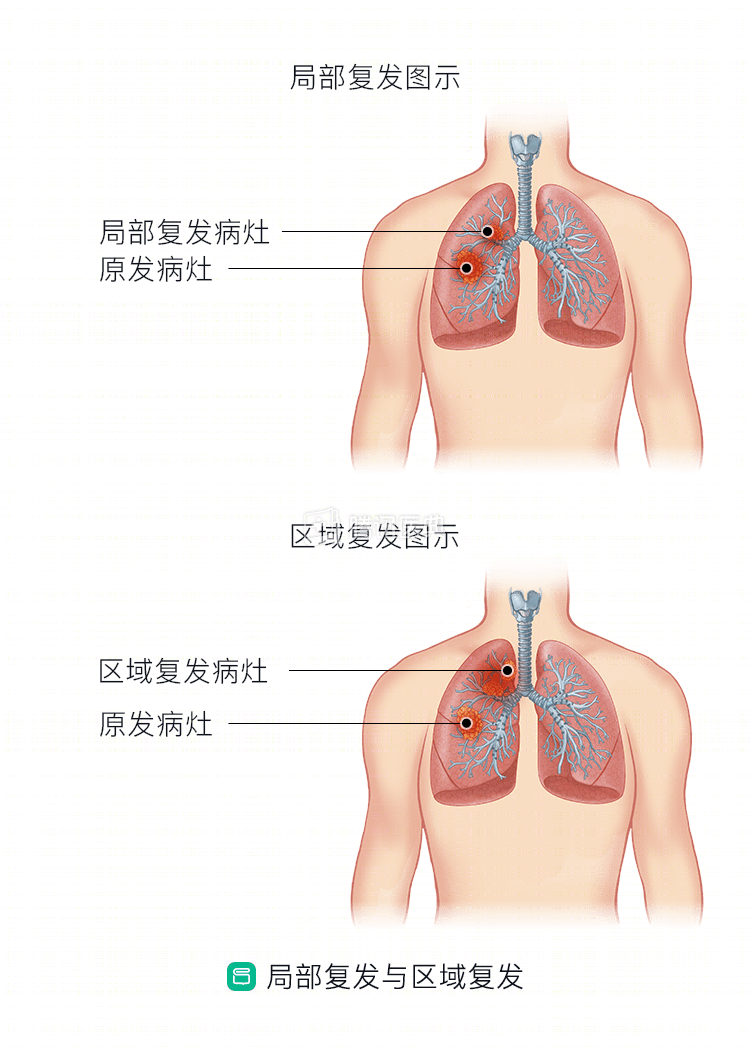
Recurrence of lung cancer can be classified as local recurrence, regional recurrence, or distant recurrence (local recurrence and regional recurrence are shown below).
- Local recurrence, where the recurrent lesion is in the vicinity of the original lesion;
- Regional relapse, where the relapsed lesion is in the lymph nodes near the original lesion;
- Distant relapse, which refers to relapse outside the lungs in the bones, brain, adrenal glands, liver, etc.
Doctors need to distinguish between a “recurrence” (“comeback”) of lung cancer and “progression” (spread or worsening) of the disease. Usually, a cancer that remains cancer-free for more than a year and is then rediscovered is considered a recurrence, and below that time frame, progression is considered more likely.
Why does lung cancer come back?
The root cause of cancer recurrence is that the cancer cells have not been completely eliminated, but this does not mean that the previous treatment was wrong or ineffective. Usually, this is due to a very small number of cancer cells that are still alive after treatment but cannot be detected by conventional tests.
Local treatment of lung cancer (surgery or stereotactic radiotherapy) primarily targets the local primary lesion. In most cases, however, lung cancer has developed “micrometastases” that are difficult to detect with conventional testing, and local therapy is usually “helpless” against micrometastases. As the micrometastases progress, the tumor will recur.
On the other hand, although systemic treatments such as chemotherapy are effective for micrometastases, they sometimes fail. Lung cancer with specific genetic mutations can be treated with targeted drugs, but some patients will have relapses due to drug resistance, such as the emergence of new mutations.
Is recurrent lung cancer the same as when it first started?
Symptoms may not be the same
Symptoms of lung cancer are directly related to the location of the lesion. For example, tumor compression of the recurrent laryngeal nerve in the airway causes hoarseness; compression of the esophagus causes dysphagia; compression of the superior vena cava causes swelling of the face, neck, and upper extremities. Therefore, similar symptoms may occur in local recurrence of lung cancer if the location is similar to that of the initial recurrence; in regional recurrence, swelling of lymph nodes; and in distant recurrence, the symptoms are site-related (brain, bone, liver, adrenal gland, etc.). Overall, the symptoms of lung cancer recurrence may not be the same as when it first occurred.
The same type of pathology
A major basis for determining that lung cancer is a recurrence rather than a second primary tumor is that the pathological type of recurrence is the same as the initial one; if it was squamous at the beginning, it is also squamous at the recurrence; if it was adenocarcinoma at the beginning, it is also adenocarcinoma at the recurrence.
Gene mutations may not be the same
Some lung cancers are driver gene-positive, and common causative mutations include EGFR, ALK, KRAS, HER2, RET, and ROS1 mutations. Take EGFR mutations, the most common gene mutation in the national population, as an example, this type of lung cancer can be treated with drugs such as EGFR- tyrosine kinase inhibitors (TKI), which are usually very effective. However, sooner or later, drug resistance will occur in almost all patients. The emergence of drug resistance is usually accompanied by relapse and progression of the disease. Nearly half of the causes of EGFR-TKI resistance are due to T790M mutations. This is another indication that the type of mutation in recurrent lung cancer may not be identical to that in the initial presentation.
How do you distinguish between a recurrence of lung cancer, or a new recurrence of lung cancer again?
According to statistics, 1% to 2% of lung cancer patients develop a second primary lung cancer each year. The criteria for determining “second primary lung cancer” are based on those established by the American College of Chest Physicians (ACCP) in 2003:
- Two foci with different histologic types, or with different molecular genetic characteristics, or with separate origins in different primary carcinomas;
- Two carcinomas of the same histologic type, but found more than 4 years apart and without systemic metastasis.
How do you distinguish between a recurrence of lung cancer or metastasis from another cancer to the lung?
Malignant tumors from other sites can also metastasize to the lung, and these tumors are different from lung cancer in terms of onset, progression, symptoms, and imaging findings.
The essential point to distinguish whether it is recurrent lung cancer or metastatic lung cancer is that the pathologic features of recurrent lung cancer are consistent with the initial lung cancer, whereas metastatic lung cancer is consistent with the pathologic features of the source tumor (e.g., liver cancer, breast cancer).
What signs indicate recurrent lung cancer? How is it detected?
When lung cancer recurs, the symptoms vary depending on the location of the recurrence.
When a local or regional recurrence occurs, what may occur are the common symptoms of lung cancer – chronic cough (mostly manifested as irritating dry cough), shortness of breath, blood in sputum or bloody sputum, chest pain, fever, etc.
When distant recurrence occurs, it is related to the site of the disease, for example, lesions in the brain can lead to dizziness, headache, loss of vision, and sometimes unilateral physical weakness or ataxia; liver lesions can lead to abdominal pain, jaundice, itchy skin, or confusion; bone lesions can lead to bone pain. When lung cancer recurs with lymph node enlargement, it can sometimes be palpable. In addition, unexplained weight loss, fatigue, and weakness are sometimes suggestive of lung cancer recurrence.
To clarify whether lung cancer has recurred, your doctor may recommend a pathology test. For lung cancers with genetic mutations, repeat tests are needed because the mutation may not be the same at recurrence as at initial presentation. Sometimes multiple biopsies are not possible, and our clinical guidelines suggest that EGFR mutations can be detected by specific liquid biopsy techniques if tissue specimens are difficult to obtain.
How is lung cancer recurrence treated? What are the results?
Once a cancer recurs, the chances of a cure are slim, and this is true for lung cancer. However, it has also been found that for patients with local recurrence and regional recurrence with aggressive remedial therapy (surgery, radiation, chemotherapy, etc.), there is no significant difference in patients’ 5-year survival compared with those without recurrence.
Treatment options for lung cancer correlate with the grade, stage, and molecular genetic type of lung cancer. Treatment options for recurrent lung cancer are also determined on a case-by-case basis, with surgery, radiation therapy, chemotherapy, targeted therapy, and immunotherapy being considered. In addition to efficacy and safety, physicians will weigh the side effects of treatment and the impact on quality of life.
Co-reviewed by: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Liao Rijiang, Associate Chief Physician Dr. Dong Song Dr. Chen Jinghua