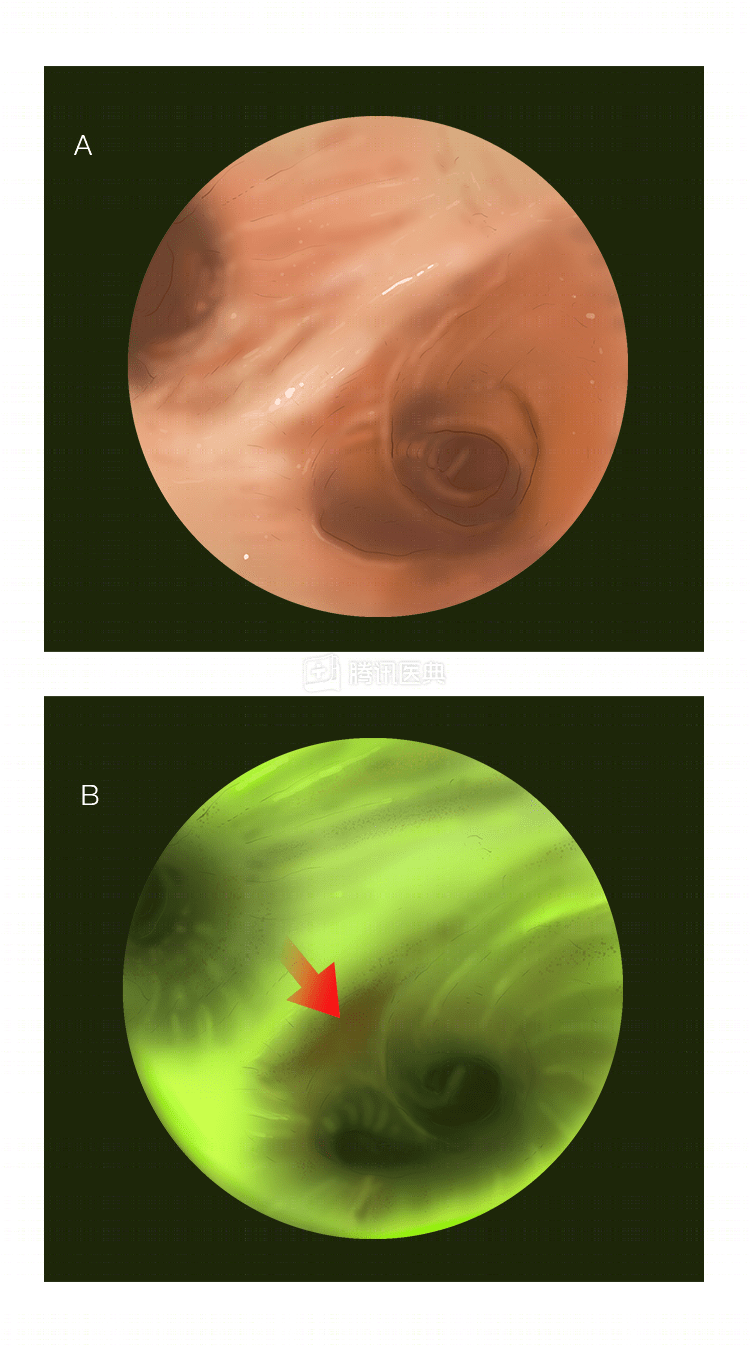
“Demonoscopy”: autofluorescence bronchoscopy (AFB)
This new technique acts as a “demon mirror” to distinguish precancerous or tumor tissue from normal bronchial mucosa, and is uniquely suited to detect early lung cancer.
It works on the principle that abnormal and normal tissues fluoresce differently in response to certain light. Under blue laser light at a wavelength of 442 nm, the diseased area appears reddish-brown while the normal area appears green, and with the help of computer image processing, the site and extent of the lesion can be determined.
The advantage is that the fine, clear, high-contrast images highlight inflammatory and tumor tissue, helping physicians easily distinguish normal from abnormal tissue and “detect” lesions early.
But it also has the disadvantage of lower diagnostic specificity and a higher rate of false positives (showing a lesion when there is none). Doctors will combine this with a low-dose spiral CT scan to improve the accuracy of early screening for lung cancer.
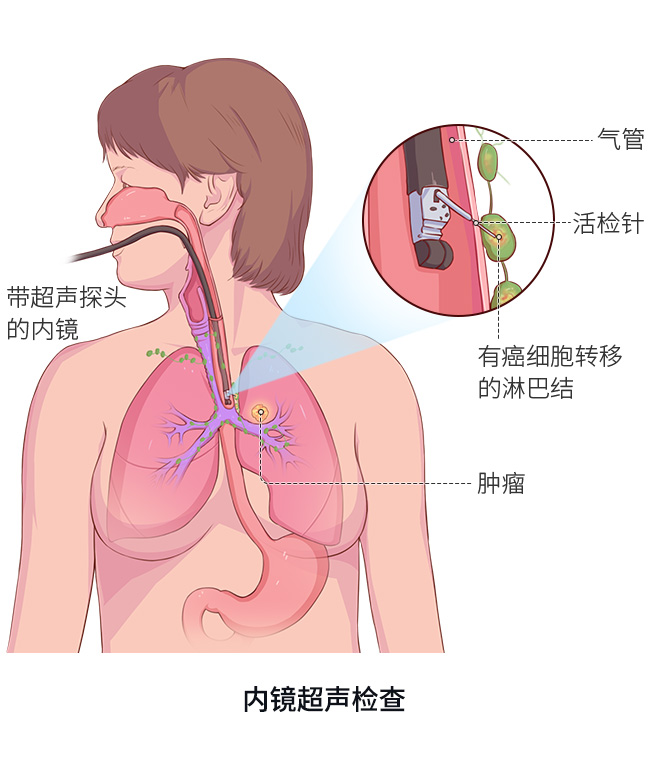
“Microprobe”: ultrasound bronchoscopy (EBUS)
This technique involves the introduction of a miniature ultrasound probe through the bronchoscopic operating orifice, which allows the physician to accurately visualize lesions in the bronchial wall, peribronchi and mediastinum, and to accurately stage lung cancer with less trauma and risk.
With EBUS-guided needle aspiration biopsy technology (TBNA), target lymph nodes and masses can be visualized in real time and the puncture path can be confirmed for biopsy under ultrasound guidance.EBUS is equipped with ultrasound Doppler to measure blood flow rates at specified locations while displaying cross-sectional images to avoid blood vessels during puncture, enabling accurate manipulation and reducing the risk of puncture.
“Faux magnetic field”: electromagnetic navigational bronchoscopy (ENB)
This new technology combines the advantages of conventional bronchoscopy and spiral CT simulation bronchoscopy.
During the operation, the patient lies on an electromagnetic positioning plate and the physician places the sensor probe in the bronchus. The sensor, combined with the magnetic field, is able to create a 3D simulated bronchoscopic image, while the spiral CT provides a realistic bronchoscopic image, and the two images are superimposed, which can be used to observe and guide the course of the probe and control its arrival at the target location.
In 1998, Solomon et al. in the United States first reported the application of ENB for animal testing, establishing the feasibility of the technique. In 2006, Gildea et al. initially demonstrated through their study that ENB has higher accuracy and safety than conventional bronchoscopy . In recent years, several national and international studies have confirmed the high diagnostic accuracy of the ENB technique for biopsy of peripheral lung lesions.
“Real-time navigation”: virtual navigation bronchoscopy technology – Lung point system
This system includes: a path planning system, a virtual bronchoscopy navigation system, and a disposable biopsy core needle (Flexneedle). The biopsy of the distal lung nodule is accomplished through three steps: localization, measurement, and navigation.
Clinical studies have shown that this technology improves diagnostic accuracy compared to conventional bronchoscopy. Compared with electromagnetic navigation bronchoscopy, virtual technology is not real-time navigation, requires less consumables and cost, requires a higher degree of CT precision, requires no special training for the operator, and is easy to master.
Co-reviewed by: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Zhou Qing, Chief Physician Dr. Bai Xiaoyan