Doctors sometimes mention that “according to current international (national) guidelines, we should ……..”. . What are “guidelines”? Why should doctors “follow” the guidelines?
Guidelines are usually written by experts from professional medical groups and are updated regularly as new research evidence becomes available. The guidelines are a summary of the “best current research evidence and expert experience”. The current mainstream guidelines are the NCCN guidelines in the United States and the CSCO guidelines in China.
So what do the guidelines say about the treatment of stage III non-small cell lung cancer?
NCCN guidelines
Note: Supraglottic sulcus, a lung cancer that is located at the lung apex and invades the chest wall.
The “jargon” in the professional guidelines above is a bit difficult to understand, so I’ll “translate” it for you. The most complex stage III lung cancer is still curable in some patients, but most patients are not so lucky.
Stage N1
Stage III patients, some of whom have only ipsilateral bronchial or hilar lymph node metastases, are called “stage N1,” and usually have surgery to remove the entire lobe of the lung where the lesion is located, sometimes even one lung. After surgery, chemotherapy, radiation therapy or a combination of the two is required. If surgery is not possible because of poor lung function or other diseases, the doctor may recommend “concurrent radiotherapy”, which means that chemotherapy and radiotherapy are administered simultaneously. It gives full play to the advantages of both therapies to achieve a “1+1>2” effect. After treatment, Durvalumab, a new immunotherapy drug, is recommended for further consolidation.
It is important to note that there is a specific type of lung cancer that is located at the apex of the lung and invades the chest wall, called a “supraglottic sulcus”. This is a special type of lung cancer that is located at the apex of the lung and invades the chest wall. Therefore, simultaneous radiotherapy before surgery and adjuvant therapy after surgery are needed to completely destroy the cancer cells.
Stage N2, N3
If the tumor expands further from N1 and invades the mediastinal lymph nodes, you are in the “N2” or “N3” stage. Some of these N2 patients still have hope for surgery, but adjuvant therapy is required both preoperatively and postoperatively.
If surgery is not appropriate, concurrent radiotherapy is usually effective. Durvalumab is also recommended at the end of treatment to consolidate the war effort.
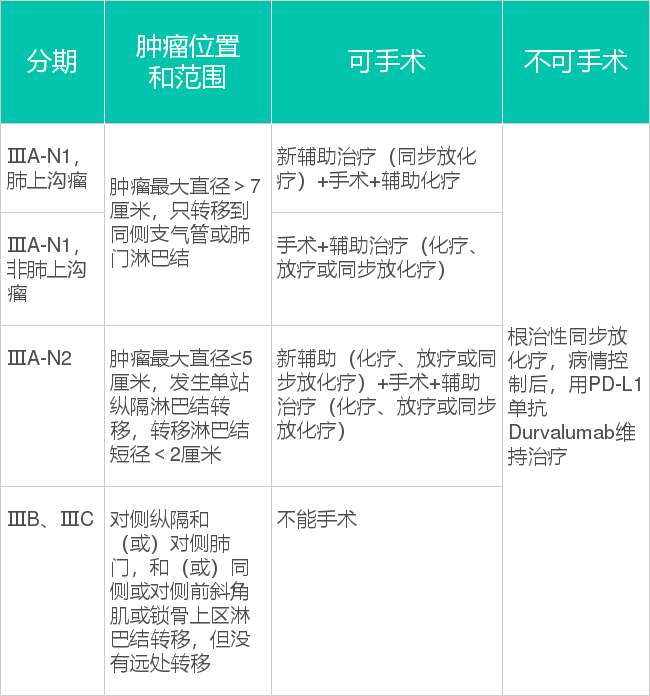
CSCO guidelines
As you can see, our guidelines are roughly the same as the US.
Stage N1
If a patient is in stage IIIA-N1, the surgeon usually chooses surgery with adjuvant chemotherapy after surgery. In patients with supraglottic sulcus tumors, neoadjuvant therapy is added preoperatively.
Stage N2
For patients with stage IIIA-N2 who are operable, surgery + adjuvant therapy is recommended.
There are several options for adjuvant therapy:
- If genetic testing is done and EGFR or ALK mutations are found, oral targeted agents are an option;
- If you don’t have these mutations, you can use “classic” chemotherapy, radiation, or a combination of both.
Neoadjuvant therapy can also be added before surgery if the doctor determines that the patient is at high risk for recurrence.
If surgery is not possible, you can do concurrent radiotherapy. But this can be more adverse, and if the patient can’t tolerate it, the doctor may also use chemotherapy or radiotherapy alone.