How lung cancer is treated depends on its type and stage. If it is early and has not metastasized, then the doctor may remove the tumor surgically and may also use radiation or chemotherapy, or if it is advanced and has metastasized to distant sites, radiation and chemotherapy may be used to shrink the tumor and help control symptoms.
In addition, the doctor will choose a treatment plan based on the side effects of the treatment, the patient’s age and overall health, and the patient’s preferences and needs. Quality of life is critical, so when the oncologist recommends a treatment, the doctor should be fully informed of his or her needs and preferences.
After the treatment plan is formed, the doctor will describe its effectiveness as well as side effects, what will be encountered and how you will feel during and after treatment, and some treatments will have side effects for which home care will be helpful.
The following are common treatments for lung cancer.
Surgery
Surgery may be considered in early stages of lung cancer without distant metastases, and is the best treatment for non-small cell lung cancer (NSCLC).
Doctors will remove part of the tumor and surrounding tissues, and if necessary, the whole lung. Some patients will also need radiotherapy and chemotherapy after surgery, and a normal open-heart surgery will require about one week of hospitalization to wait for the wound to heal.
However, nowadays, minimally invasive surgery is becoming more and more common, as doctors can probe and remove the tumor by probing a hose (i.e., thoracoscope) into the patient’s lung, leaving only a small incision in the patient’s chest and shortening the recovery time.
Small cell lung cancer (SCLC) usually cannot be removed surgically.
Radiofrequency ablation
Some patients with non-small cell lung cancer do not meet the indications for surgery, then radiofrequency ablation may be considered.
This is done by introducing a very thin electrode needle into the patient’s body until it enters the lung tumor, and then a high-frequency current passes through, creating heat that kills the cancer cells.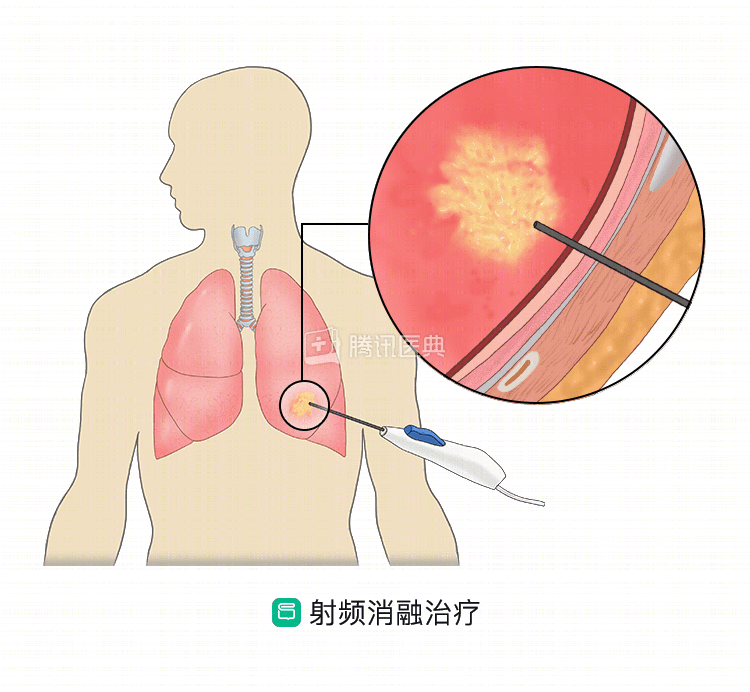
Radiotherapy
Radiotherapy, in which high-energy X-rays are targeted to the tumor site to kill tumor cells through the biological effects of ionizing radiation, is used for non-small cell lung cancer and also for small cell lung cancer (SCLC).
Radiotherapy is often given in combination with surgery, chemotherapy, or sometimes all 3 modalities together. Radiotherapy is given as a course of treatment, which may last for several weeks, several days a week.
Preoperative radiation therapy shrinks the tumor, making surgery easier and improving resection rates. Postoperative radiation therapy destroys cancer cells left over from surgery, and radiation therapy also helps relieve some of the symptoms of lung cancer, such as pain and bleeding.
Chemotherapy
Chemotherapy uses chemicals to kill cancer cells and can be used for both non-small cell lung cancer and small cell lung cancer.
Chemotherapy can be used before and after surgery, and can also be used in combination with radiation therapy, which may be the main treatment option if surgery is not possible.
When chemotherapy is given, the doctor may use a single drug or may combine different chemotherapy drugs (i.e., combination chemotherapy). Chemotherapy may be done by sedation (drip or push) and may need to last for several weeks.
Other therapies for non-small cell lung cancer
The following approaches may also be used to treat non-small cell lung cancer, for example
- Photodynamic therapy. Uses drugs and special rays to treat the cancer.
- Cryosurgery. Can be used to freeze and destroy tumors in the lungs.
- Electrocautery. Uses a low voltage load to destroy the tumor.
- Close observation. This means that the tumor is not treated until symptoms or some kind of change occurs and the doctor observes it closely; this method is only used in a few cases.
Other treatments for small cell lung cancer
Patients with tumor compression of the airway can also be treated with endoscopic stent placement to relieve the symptoms of patients whose breathing is being compressed by the tumor.
With the help of an adjustable, lighted endoscope, doctors place a small hollow wire mesh tube (stent) into the trachea, which holds the airway open and allows the patient to breathe freely.
A new approach to treatment
To help lung cancer patients live better and longer, researchers have been working to find better treatments, and scientists are investigating new combination chemotherapy regimens, new forms of radiation therapy, and drugs that make cancer cells more sensitive to radiation therapy. These approaches include.
Targeted therapy
Targeted drugs can work precisely on cancer cells or specific parts of the tumor, using drugs such as monoclonal antibodies or tyrosine kinase inhibitors (TKI) to stop the growth of cancer cells, and some targeted drugs can even control lung cancer that has metastasized.
Doctors will test patients for several tumor markers (also called biomarkers), such as EGFR, ALK, KRAS, etc. They are just a few targets where gene mutations in non-small cell lung cancer cells often occur, and by figuring these out, doctors can choose the best treatment plan for their patients.
Commonly used targeted drugs.
- Afatinib (Afatinib).
- Elotinib (Alectinib).
- Bevacizumab (Bevacizumab).
- Bugatinib (Brigatinib).
- Ceritinib (Ceritinib).
- Crizotinib (Crizotinib).
- Erlotinib (Erlotinib).
- Gefitinib (Gefitinib).
- Nexitumumab (Necitumumab).
- Osimertinib (Osimertinib).
- Remolimumab (Ramucirumab).
Immunotherapy
There are also drugs, such as nabumab (Nivolumab) and pembrolizumab (Pembrolizumab), that will use the body’s own immunity to attack cancer cells, an approach called immunotherapy.
Follow-up treatment
Follow-up after the initial treatment is also important. The frequency of follow-up is related to the treatment plan and patient history, usually once every 3 to 4 months, and decreases after 2 to 3 years of treatment, but needs to be done at least once a year.
Follow-up examinations include physical examinations, blood tests, chest X-rays, CT scans, or other tests recommended by the oncologist.
Clinical trials
Patients may be interested in clinical trials that contain up-to-date information about treatment and are being conducted to find better treatments.
Patients who do not want to receive standard treatment, or for whom standard treatment has not worked, may prefer to participate in a clinical trial, and patients can ask their doctor for information about which studies they are suitable for and how to participate.
Supportive treatment
Supportive therapy differs from curative therapy in that it focuses on symptom relief. Its goal is to improve the patient’s quality of life, both physically and mentally, and it can be used in combination with curative therapy.
The doctor will help the patient manage pain or side effects, will help the patient decide whether to take the treatment he wants or doesn’t want, and will help relatives understand how to support the patient.
A study of patients with non-small cell lung cancer (NSCLC) showed that receiving this therapy not only allowed patients to feel the effects of treatment, but also actually prolonged their lives compared to not receiving supportive treatment at the time of the initial lung cancer diagnosis.
Treatment at the end of life
For some patients with advanced cancer, treatment is no longer the best option, because the side effects of treatment, the pain from the disease itself, and the time and money it takes to treat are far greater than the hope of a cure or remission.
However, patients can still receive some treatment before they die to make themselves feel as comfortable as possible. Patients and their families can communicate with their doctors to decide the timing of receiving hospice care (hospice care).
Co-reviewed by: Guangdong Provincial People’s Hospital, Guangdong Provincial Lung Cancer Institute Dr. Dong Song and Dr. Zeng Fanjun.