Review plan
The review plan is different for patients with different stages of lung cancer. Patients with stage I-III lung cancer are usually treated with radical aim such as surgery or simultaneous radiotherapy. The risk of recurrence is highest within 2 years after the end of treatment, and the risk of developing a second primary lung cancer is elevated 2 years after the end of treatment. Therefore, patients with stage I to III lung cancer should be followed up with surveillance by imaging every 6 months for 2 years after treatment to detect recurrence. After 2 years of treatment, patients should undergo annual imaging surveillance to detect new primary lung cancer.
Follow-up schedule for patients with stage I lung cancer
| 1 to 2 years post-op | 3rd, 4th, 5th year post-op | >5 years post-op | |
| Month 6, Month 12 | Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
|
|
Blood count, biochemistry |
Month 6, Month 12 | Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
| Month 6, Month 12 | Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
|
| Month 6, Month 12 | Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
Follow-up schedule for patients with stage II lung cancer
| 1 to 2 years post-op | 3rd, 4th, 5th year post-op | >5 years post-op |
| Month 6, Month 12 | Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
| Month 6, Month 12 | Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
| Month 6, Month 12 | Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
| Month 6, Month 12 | Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
Follow-up schedule for patients with stage III lung cancer
| 1 to 2 years post-op | 3rd, 4th, 5th year post-op | > >5 years post-op | |
| March, June, September, December | Month 6, Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
|
| Month 3, Month 6, Month 9, Month 12 | Month 6, Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
|
| Tumor markers | Month 3, Month 6, Month 9, Month 12 | Month 6, Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
| CT of chest, upper abdomen, bone ECT, brain MRI | (Month 3), Month 6, (Month 9), Month 12 | Month 6, Month 12 |
When there are clinical signs (e.g., cough, chest tightness, chest pain, hoarseness, etc.) |
Note: The brackets are optional depending on the patient’s condition, especially for stage IIIB lung cancer patients without surgical treatment, where the frequency of review can be increased as appropriate due to the elevated risk of recurrence.
Individualized postoperative follow-up strategies are lacking both domestically and internationally. The important prerequisite for achieving individualized follow-up is to clarify the individualized recurrence risk. Through a multicenter study with a large sample, Professor Chen Haiquan’s team at the Cancer Hospital of Fudan University created the first site-specific web-based prediction model for postoperative recurrence of stage I-III lung cancer in the world. The prediction model can calculate the risk of recurrence in each site of chest, abdomen, neck, brain and bone respectively, and guide the selection of different imaging means in the follow-up process; moreover, it can calculate the dynamic conditional probability of recurrence according to different postoperative follow-up times, which is closer to the clinical work practice. The research results were published in Chest, an authoritative journal in thoracic medicine. Further collaboration with the School of Pharmacy of Shanghai Jiao Tong University has developed intelligent prediction software based on the model for clinical work (URL: http://nsclc.cn/). By simply entering the clinicopathological information and follow-up time information of a particular patient on the webpage, it is possible to calculate an individualized and dynamic risk of recurrence and to develop an individualized postoperative follow-up strategy for the patient. The predictive model website has now been visited more than 200,000 times.
Stage IV lung cancer is incurable, and patients typically undergo chemotherapy, immunotherapy, or targeted therapy focused on prolonging survival and relieving symptoms. Because of the high risk of progression in advanced lung cancer, systemic exams and imaging assessments should be performed every 3 months after the end of treatment to detect tumor progression early.
| 1 to 2 years post-op | 3rd, 4th, 5th year post-op | >5 years post-op |
| March, June, September, December | Month 3, Month 6, Month 9, Month 12 | Month 12 |
| Month 3, Month 6, Month 9, Month 12 | Month 3, Month 6, Month 9, Month 12 | Month 12 |
|
Month 3, Month 6, Month 9, Month 12 |
Month 3, Month 6, Month 9, Month 12 | Month 12 |
| Month 3, Month 6, Month 9, Month 12 | Month 3, Month 6, Month 9, Month 12 | Month 12 |
Notes
1 . The review should be done as prescribed by the doctor, at the time and according to the items prescribed by the doctor.
2 . At each review, bring the initial imaging and pathology reports, along with imaging films of all initial and most recent lesions (chest CT films, brain MRI films, etc.), and medical records such as treatment course notes.
3 . Describe clearly recent symptoms, especially new discomfort, such as cough, chest pain, fatigue, weight loss, etc.
4 .
4 . If you have any psychological problems, you should also describe them to your doctor.
5 . If you have any psychological problems, you should also describe them to your doctor. If you need to take medication, keep detailed records of how it was taken, the duration of treatment, adverse effects, and monitoring indicators.
Indicators that need special attention
1. General: Patients with lung cancer need to have their weight measured regularly, and if they experience significant weight loss in a short period of time for no apparent reason, they need to promptly report this to their doctor.
2. Laboratory tests: Some lung cancer patients may have anemia, leukopenia, and impairment of liver and kidney function due to the disease and treatment, and should also have regular follow-up blood tests and liver and kidney function to understand the recovery of organ function after treatment is completed.
1) Routine blood tests, alert for bone marrow suppression
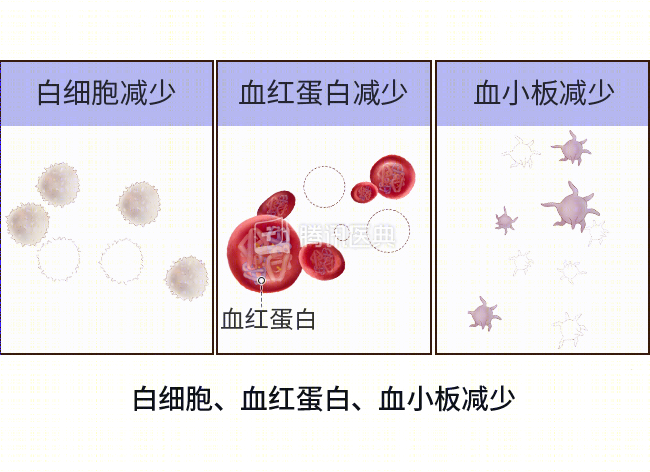
If the report shows white blood cells <3.0×109/L, hemoglobin <90 g/L, and platelets <75×109/L, there is a possibility of bone marrow suppression or other abnormalities.
Bone marrow suppression is a common adverse effect of radiotherapy or chemotherapy in lung cancer patients, and patients often have varying degrees of hemoglobin, white blood cell, or platelet reduction. Therefore, once the possibility of bone marrow suppression is detected, the doctor needs to be contacted for treatment at the first opportunity.
②Liver and kidney function tests to prevent liver and kidney function damage
Any abnormal elevation of alanine aminotransferase (ALT), aspartate aminotransferase (AST), and bilirubin, as well as a blood creatinine higher than the upper limit of normal, on the liver and kidney function test report should alert you to the presence of treatment-related liver and kidney impairment and require prompt consultation with your doctor for further testing.
②Tumor marker values to watch
Lung cancer patients need to be tested for lung cancer tumor markers, such as carcinoembryonic antigen, squamous carcinoma antigen, and neuroenolase, which are correlated with tumor disease and should be reported to the physician in a timely manner if there is a sudden and rapid increase in indicators, and imaging should be performed in a timely manner to exclude recurrence and metastasis.
3. Imaging: Lung cancer patients should have regular review of chest CT, upper abdominal CT, bone ECT and cranial MRI to detect tumor recurrence and metastasis in liver, adrenal gland, bone, brain, etc. If the report suggests abnormalities such as enlarged lesions or new lesions, you should promptly ask your doctor to read the films to clarify the nature of the lesions and whether the tumor has recurred and metastasized.
4. It is important to note that some new circulating markers, such as circulating tumor cells and free DNA, have not been recommended by guidelines for follow-up surveillance of lung cancer, so there is no need for private testing and you should follow your doctor’s instructions.