In our country, “lung cancer vaccine” may sound a little strange. But back in 2008, Cuba’s drug regulator approved a vaccine (CIMAvax-EGF) to treat adults with progressive non-small cell lung cancer (NSCLC). This was the first therapeutic vaccine for lung cancer to be marketed worldwide. A few years later, another lung cancer vaccine, Racotumomab, was also approved in Cuba and became the initial treatment for NSCLC in 2013.
So, what is a lung cancer vaccine? How is it different from the vaccines we usually get for infectious diseases? How effective is it in treating lung cancer? Here’s what you need to know.
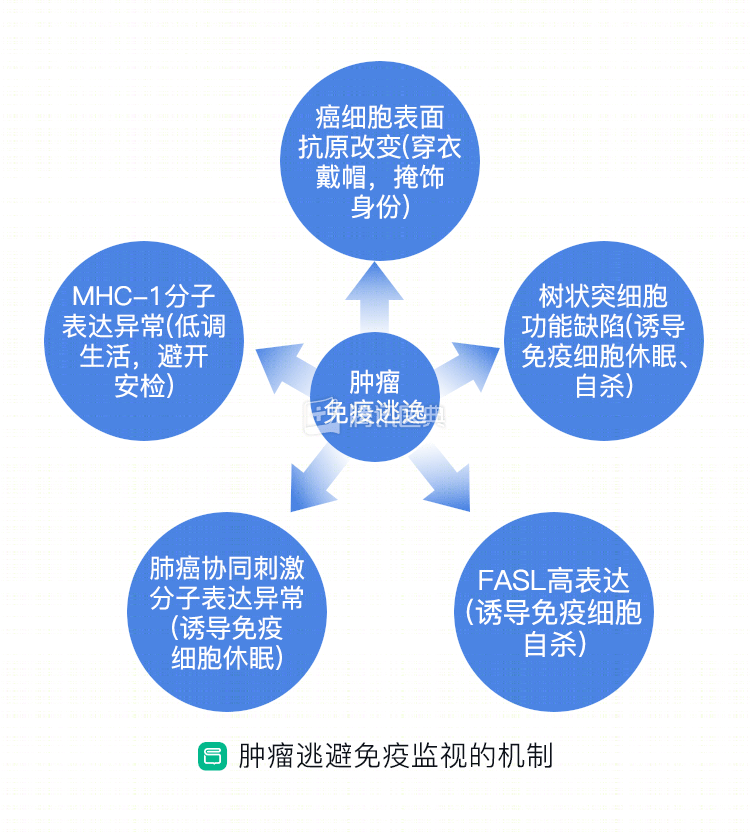
We know that cancer cells have the ability to grow indefinitely; not only does it grow fast, but it can also metastasize far away. Why does our body’s defense engineering, the immune system, turn a blind eye to cancer cells and let them grow? This is because cancer cells are particularly cunning and have many ways to evade the fight, including “camouflage”, “hypnosis”, “dodging”, inducing immune cells to “kill themselves”, etc. (Figure 1). This is known as “tumor immune escape” in professional circles.
Lung cancer vaccine helps immune system ‘shine the light’
The lung cancer vaccine builds on the concept of an infectious disease vaccine that “triggers” active immunity in the body, through a series of methods that allow our immune system to actively identify and kill tumors. In short, it “tells” the immune “police” about the characteristics of cancer cells: don’t be confused, that’s the bad guy, go get him.
What lung cancer vaccines are currently available and worth waiting for?
The lung cancer vaccines currently in development, or already in use, can be broadly divided into 3 categories: protein peptide vaccines, tumor vaccines, and antibody vaccines. We describe each.
Protein peptide vaccines
Protein peptide vaccines are vaccines that are prepared by chemical synthesis of an amino acid sequence in a tumor antigen (an antigen is a substance that triggers a response from the immune system). In short, the antigen carried by the tumor cells is prepared as a vaccine that stimulates the body to produce an immune response.
The MUCin-1 vaccine and the EGF vaccine are examples of these.
MUCin-1 (MUC-1) is a glycoprotein on the cell membrane surface that is abundantly distributed and appears structurally abnormal on the cell surface of many tumors, including NSCLC, making it a tumor marker. It can kill or disable immune cells.
Studies have shown that if a patient with advanced lung adenocarcinoma has high levels of MUC1 in his blood, it often suggests a suppressed state of immune function and a poorer outcome.
The MUC1 vaccine specifically targets MUC1, and two vaccines have been tested in clinical trials: TG4010 and L-BLP25. These trials have shown that in patients with intermediate-stage (stage IIIb or IV) NSCLC, the combination of the TG4010 or L-BLP25 vaccine increases the efficacy of chemotherapy after they have received standard first-line chemotherapy. The safety profile of both vaccines is also relatively good. Common adverse effects include fatigue, cough, nausea, and flu-like symptoms.
EGF (epidermal growth factor) stands for “epidermal growth factor,” which binds to its receptor (EGF receptor, EGFR, which is overexpressed or abnormal on the surface of many tumor cells) to promote tumor proliferation, angiogenesis, and metastasis. .
CIMAvax-EGF, the world’s first “Cuban vaccine” mentioned earlier, is one such protein vaccine that induces antibodies against EGF and prevents it from binding to EGFR, thereby inhibiting tumor growth.
A phase II clinical trial evaluated the effectiveness, safety, and efficacy of CIMAvax-EGF in patients with advanced NSCLC who had received first-line chemotherapy. The results showed that the vaccine was generally safe, with less than a quarter of patients experiencing adverse events and no serious adverse events. Patients in the vaccinated group had a 4-month longer survival compared to the unvaccinated group. The prolonged survival of the vaccine was more pronounced in patients younger than 60 years (18.53 months in those younger than 60 years and 7.55 months overall).
Tumor vaccine
Tumor vaccines work by introducing tumor-specific antigens into the patient’s body, reactivating the immune system’s ability to recognize and fight the tumor.
“Tumor-specific antigens” include tumor cells, tumor-associated proteins or peptides, genes that express tumor antigens, and so on. The antigens can be exposed by treating tumor cells with physical, chemical, or biological methods, or the immunogenicity (understood as the ability to stimulate an immune response) of a tumor vaccine can be enhanced by some specific methods to stimulate the immune system to generate an immune response to the tumor.
Belagenpumatucel-L falls into this category of vaccines.
Belagenpumatucel-L vaccine