Lung cancer surgery needs to be performed inside the chest cavity. In addition to the lung lobes, there are other important nerves, blood vessels, and organs in the thoracic cavity that could be damaged during surgery.
Who can be injured during surgery?
Who can be injured during surgery?
Vessels
The important vessels in the thoracic cavity are the aorta, pulmonary artery, pulmonary veins, subclavian arteries, superior and inferior vena cava, odd veins, and intercostal vessels, all of which are relatively large central vessels that can lead to hemorrhage if injured.
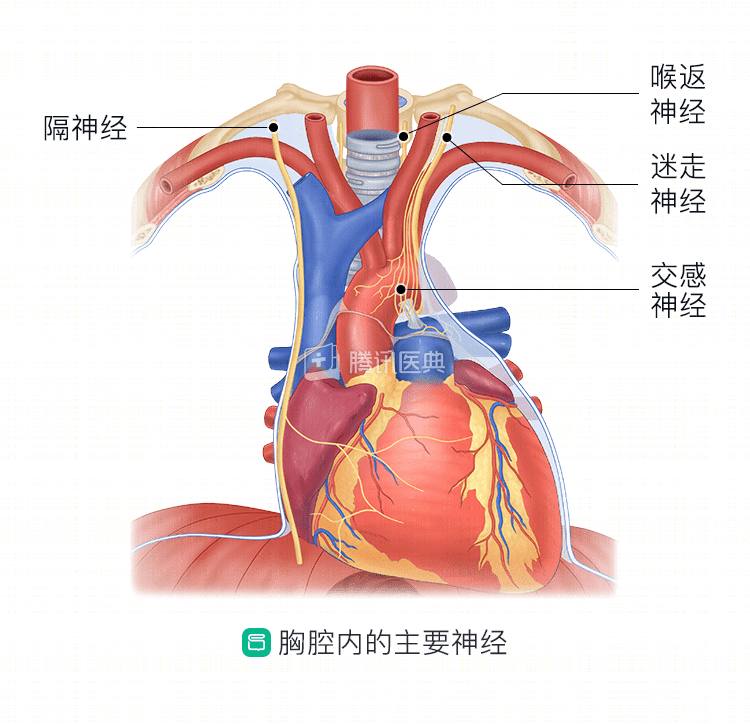
Nerves
The main nerves that travel through the chest cavity are the vagus nerve, phrenic nerve, recurrent laryngeal nerve, and sympathetic nerves in the chest wall.
The vagus nerve controls our heart rate, respiration, and digestive system function, and when damaged, it can lead to abnormal heart rate, poor gastrointestinal motility, and more.
The phrenic nerve controls the movement of the diaphragm. The diaphragm is the “bottom” of the chest and the “top” of the abdomen, and plays an important role in our breathing: when it contracts, the chest expands to help us breathe in, and when it relaxes, the chest shrinks to help us breathe out. Once damaged, respiratory function decreases.
The recurrent laryngeal nerve controls our vocal cords and some of our respiratory swallowing muscles. If it is damaged unilaterally, you may have hoarseness and choking after surgery; if it is damaged bilaterally, you may have difficulty breathing and even choking after surgery.
Sympathetic nerve damage can result in localized skin numbness, pain, loss of sensation, or absence of sweating on one limb or head and face. If the sympathetic nerves in the neck are damaged, there may be a narrowing of the pupils and a sunken eye, known medically as Horner syndrom.
Organs
The main organs that are susceptible to injury are the thoracic duct and esophagus.
The thoracic duct is the largest lymphatic vessel in the body, collecting lymphatic fluid and draining it into the lymphatic circulation. Once damaged, it can cause lymphatic fluid to “leak” into the pleural cavity, which is known professionally as “celiac disease” and requires long-term chest tube drainage or reoperation.
The esophagus is the pathway through which we eat and drink every day. If it is damaged, it can lead to a tracheal connection with the esophagus, which is called a “tracheoesophageal fistula”. The esophageal contents can flow into the trachea, causing choking, lung infection, and respiratory failure. If poorly controlled, further damage to other organs in the mediastinum may occur.
Pericardium, diaphragm
The pericardium is a membrane that wraps around the outside of the heart. If the tumor invades the pericardium or diaphragm, the doctor will need to cut open the pericardium and damage the diaphragm. After the pericardium is cut, the heart may protrude outside the pericardium, forming a “heart hernia”. When the diaphragm is partially thinned, the abdominal pressure may perforate the thinned area, and the abdominal organs may “pass” into the thoracic cavity, forming a “diaphragmatic hernia”.
Ribs
The gap between the human rib cage is narrow, and open-heart surgery requires instruments to hold the rib cage open and expose the surgical site to the surgeon’s view. This can lead to rib fractures and increased postoperative pain. The elderly and postmenopausal women are prone to osteoporosis, and they are more likely to have fractures.
How to respond?
Unilateral nerve injury is usually not life-threatening. There is no good management for nerve injury, and you may recover gradually over 1 to 2 years after surgery.
If celiac disease develops, you may observe a milky white drainage or a large amount of fluid that does not go away for a long time. After surgery, you will need to “avoid” eating fatty foods and strictly control your fat intake; you may even need to fast and switch to intravenous fluid for nutritional support. If conservative treatment does not work, surgical ligation of the chest tube may be required.
If an esophagotracheal fistula develops, there will be a violent cough with drinking or eating, which may be accompanied by sputum or fever. Early postoperative fasting is required, with nasal feeding to feed or rehydrate, along with anti-infective therapy. If the fistula is large, surgical treatment is required.
Related reading:
Co-authors: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Zheng Shaopeng Dr. Xia Jin