Approval Date:
Revision Date:
Risulvastatin Calcium Tablets Instructions
Please read the instructions carefully and use under the guidance of your physician
[Drug Name]
Generic Name: Rosuvastatin Calcium Tablets
English name:Rosuvastatin Calcium Tablets
Hanyu Pinyin:Ruishufatatinggai Pian
[Ingredients]
The active ingredient of this product is Rosuvastatin calcium.
Chemical name: bis-[(E )-7-[4-(4-fluorophenyl)-6- >isopropyl-2-[methyl< span style="font-family:Times New Roman">(Methanesulfonyl)amino]-pyrimidine< span style="font-family:Times New Roman">-5-base](3R,5S )-3,5-dihydroxyheptan-6- enolate]calcium salt (2:1)
Chemical structure formula:
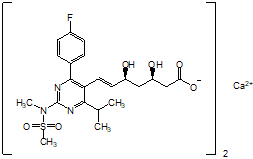
Molecular Formula:(C22H27FN3< /sub>O6S)2Ca
Molecular weight:1001.13
[Properties]
This product is a film-coated tablet, which appears white or off-white after removing the coating.
[Indications]
This product is indicated for primary hypercholesterolemia that is not adequately controlled by dietary control and other non-pharmacological treatments (e.g., exercise therapy, weight loss) for dyslipidemia (). family:Times New Roman”>Type IIa, including heterozygous familial hypercholesterolemia) or mixed dyslipidemia (IIbtype).
This product is also indicated in patients with pure-onset familial hypercholesterolemia as a component of dietary control and other lipid-lowering measures (e.g., LDLremoval therapy) or as an adjunct to these methods when they are not indicated.
[Specification]By Rosuvastatin (C22) H28FN3O6S) count:
(1)5mg
(2)10mg
[dosage]
Patients should be given standard cholesterol-lowering dietary control prior to the start of therapy and maintain dietary control during therapy. The use of this product should be individualized, taking into account the individual patient’s cholesterol level, expected cardiovascular risk, and potential risk of adverse events.
Oral. The usual starting dose of this product is 5 mg once a day. The choice of starting dose should take into account the individual patient’s cholesterol level, the expected cardiovascular risk, and the potential risk of adverse events. For those patients who require a more potent reduction in LDL cholesterol (LDL-C) may be considered10 mgonce a day as a starting dose, which controls lipid levels in most patients. If necessary, the dose may be adjusted to a higher dose level after 4weeks of treatment. The maximum daily dose of this product is20 mg.
This product can be administered at any time of the day and can be taken with food or on an empty stomach.
Medication for patients with renal insufficiency
No dose adjustment is required in patients with mild and moderate renal impairment. All doses of this product are contraindicated in patients with severe renal impairment.
Dosing in patients with hepatic impairment
InChild-Pughscores no higher than7 in subjects with no elevated systemic exposure to Rosuvastatin. In Child-Pughscores. New Roman”>8and9of subjects, elevated systemic exposure was observed. In these patients, assessment of renal function should be considered. Subjects without a Child-Pughscore above9 in patients with experience with this product. This product is contraindicated in patients with active liver disease.
People
Increased whole-body exposure has been observed in Asian subjects. This factor should be considered when determining dosing in patients of Asian ancestry.
Dosing in patients with predisposition factors for myopathy
Recommended starting dose for patients with predisposition to myopathy (see [precautions]) is5 mg. .
[Adverse Reactions]
Adverse reactions seen with this product are usually mild and transient. In controlled clinical trials, fewer than4% of patients withdrew from the trial due to adverse events.
List of adverse events
Based on clinical study data and extensive post-marketing experience, the following table lists the adverse event characteristics of resulvastatin. The following adverse events are classified according to frequency and systemic organ class.
The frequency of adverse events is listed in the following order: common(≥1/100, << span style="font-family:Times New Roman">1/10); see occasionally(≥1/1,000, < >1/100); rare (≥1/10,000, <1/1,000); very rare( <1/10,000); unknown (cannot be estimated from available data).
|
System organ classification |
Common |
Eventually |
Rare |
Very rare |
unknown |
|
|
Abnormalities of the blood and lymphatic system |
Thrombocytopenia |
|||||
|
Immune system abnormalities |
Allergic reactions (including angioedema) |
|||||
|
Endocrine Disorders |
Diabetes1 |
|||||
|
Mental abnormalities |
depression |
|||||
|
Neurological abnormalities |
Headache Dizziness |
Polyneuropathy Memory loss |
Peripheral neuropathy Sleep disorders (including insomnia and nightmares) |
|||
|
Respiratory, thoracic, and mediastinal abnormalities |
cough Hard to breathe |
|||||
|
Gastrointestinal abnormalities |
Constipation Nausea Abdominal pain |
Pancreatitis |
Diarrhea |
|||
|
Hepatobiliary abnormalities |
Elevated transaminases < /td> |
Jaundice Hepatitis |
||||
|
Dermal and subcutaneous tissue abnormalities |
itching Rash Hives |
|||||
|
Skeletal muscle and connective tissue abnormalities |
myalgia > |
Myopathy (including myositis) Rhabdomyolysis |
Joint pain |
Joint pain | < p>Tendon damage and sometimes rupture complications Immune-mediated necrotizing myopathy |
|
|
< em>Kidney and urinary tract abnormalities |
Hematuria | |||||
|
Reproductive and breast abnormalities |
Gynecomastia |
|||||
|
Systemic abnormalities and medication site discomfort |
Powerless |
Oedema |
||||
|
1 |
||||||
Same as otherHMG–CoA As with reductase inhibitors, the incidence of adverse reactions with this product tends to increase with increasing dose.
Effects on the kidney: Proteinuria (as detected by the test paper method) was observed in patients receiving this product, with the majority of the protein originating from the renal tubules. Less than1% of patients on10 mg and 20 mgProteinuria elevated from none or trace to ++ or more at certain times during treatment, after receiving 40 mg, this percentage is about 3% in patients treated with /span>. In 20 mgdose therapy, an increase in proteinuria was observed from none or trace to family:Times New Roman”>+ mildly elevated. In most cases, proteinuria decreases or disappears spontaneously with continued treatment. A causal relationship between proteinuria and acute or progressive kidney disease cannot be established based on clinical trials and post-marketing data to date.
Hematuria has been observed in patients using this product, and data from clinical trials suggest that its incidence is low.
Effects on skeletal muscle: Effects on skeletal muscle, such as myalgia, myopathy (including myositis), and, rarely, rhabdomyolysis, have been reported in patients treated with various doses of this product, particularly at doses greater than 20 mg in patients.
Creatine kinase (CK) levels are dose-related; most cases are mild, asymptomatic, and transient. If creatine kinase levels are elevated (>5×ULN), treatment should be discontinued (see [Precautions]).
Effects on the liver: Same as otherHMG–CoAreductase inhibitors, in Dose-related transaminase elevations have been observed in a small number of patients taking this product; most cases are mild, asymptomatic, and transient.
The following adverse events have been reported with certain statin therapy:
Sexual dysfunction
Special cases of interstitial lung disease, especially in those receiving long-term treatment.
Pediatric Patient Population: Pediatric and adolescent patients treated with resulvastatin over a period of52week clinical trial found creatine kinase elevations greater than10×ULN, as well as concomitant muscle symptoms observed after exercise or enhanced physical activity, compared to those observed in adults frequency observed in clinical trials conducted in adults. Otherwise, the safety profile of resulvastatin in pediatric and adolescent patients is similar to that in adults.
Statin drugs:
1.Post-marketing surveillance of statin drugs with hyperglycemic reactions, abnormal glucose tolerance, glycated hemoglobin The study also reported reports of hypoglycemic reactions, abnormal glucose tolerance, elevated glycated hemoglobin levels, new-onset diabetes, and worsening glycemic control for some statins.
2.Post-marketing experience: Rare reports of cognitive impairment have been reported in foreign post-marketing surveillance of statins, manifesting as memory loss
[Contraindicated]
This product is contraindicated in:
- style=”margin-left: 39pt”>
-
Hypersensitivity to Rosuvastatin or any of the ingredients in this product.
-
Patients with active liver disease, including persistent elevation of serum aminotransferases of unknown cause and any elevation of serum aminotransferases above3 times the upper limit of normal (ULN) for patients.
-
Patients with severe renal impairment (creatinine clearance<30ml/min).
-
Patients with myopathy.
-
Patients with concomitant cyclosporine use.
-
Women during pregnancy, while breastfeeding, and at risk of pregnancy without adequate contraception.
[Precautions]
On the kidneys
At high doses especially 40 mgtreated patients, proteinuria (detected by the test paper method) was observed, most of the protein originated from the renal tubules, and in most cases, proteinuria was transient or intermittent. Proteinuria was not considered a precursor to acute or progressive kidney disease (see “Adverse Reactions”).
Action on skeletal muscle
Effects on skeletal muscle, such as myalgia, myopathy, and, rarely, rhabdomyolysis, have been reported in patients treated with various doses of this product, particularly at doses greater than20 mg in patients. Ezetimibe has been reported in combination with HMG-CoAreductase inhibitors with very rare reports of rhabdomyolysis. Interaction of drug effects cannot be ruled out, and caution should be exercised when these drugs are combined.
Creatine kinase assay
Creatine kinase should not be tested after strenuous exercise or in the presence of plausible factors that cause creatine kinase elevation (CK), which can confuse the interpretation of the results. If the creatine kinase basal value is significantly elevated (>5×ULN), which should be used in5 to 7 days for retesting confirmation. If repeat testing confirms that the patient has a creatine kinase basal value >5×ULN, then treatment cannot be started.
Before treatment
and otherHMG–CoA As with reductase inhibitors, caution should be exercised when using this product in patients with factors predisposing them to myopathy/rhabdomyolysis. These factors include:
- style=”margin-left: 54pt”>
-
Renal impairment
-
Hypothyroidism
-
Hereditary muscle disease in one’s own or family history
-
Past history of otherHMG-CoAreductase inhibitors or betablockers with a history of muscle toxicity
-
Alcohol abuse
-
Age& gt;70years
-
May occur with elevated blood levels
-
Concurrent use of fibrates
In these patients, the possible benefit of therapy should be considered in relation to the potential risk, and clinical monitoring is recommended. If the patient has a significantly elevated creatine kinase basal value (>5×ULN), then treatment should not be started.
In treatment
Patients should be asked to immediately report unexplained muscle pain, weakness, or spasticity, especially when accompanied by discomfort and fever. Creatine kinase levels should be tested in these patients. If creatine kinase values are significantly elevated (>5×ULN) or muscle symptoms that are severe and cause discomfort throughout the day (even if creatine kinase≤5 >×ULN), treatment should be discontinued. If symptoms resolve and creatine kinase levels return to normal, consider re-giving this product or switching to another HMG–Minimal dose of CoAreductase inhibitor with close observation.
Regular testing of creatine kinase levels is not required in asymptomatic patients.
Rarely, there is immune-mediated necrotizing myopathy associated with statin use (IMNM) (an autoimmune myopathy) has been reported. IMNM was characterized by proximal muscle weakness and elevated serum creatine kinase, which persisted with or without discontinuation of statin therapy. Muscle biopsy showed necrotizing myopathy without significant inflammation; it improved with the application of immunosuppression.
In clinical studies, there was no evidence of increased drug effects on skeletal muscle in the small number of patients treated with concomitant use of this product and other treatments. However, it has been found that in otherHMG–CoAreductase inhibitors in combination with febric acid derivatives (including gemfibezil), cyclosporine, nicotinic acid, pyrrole antifungals, protease inhibitors, or macrolide antibiotics, the myositis and myopathy incidence was increased. Gemfibezil is associated with some HMG–CoAreductase inhibitors can increase the risk of myopathy when used concomitantly. Therefore, the combination of this product with gemfibezil is not recommended. The benefits of combining this product with fibrates or niacin to further improve lipid levels should be carefully weighed against the potential risks of such combinations.
Risulvastatin in combination with fusidic acid is not recommended. Rhabdomyolysis, including death, has been reported in patients receiving this combination. (See“Drug Interactions“)
For any patient with acute severe illness suggestive of myopathy or prone to renal failure secondary to rhabdomyolysis (e.g., sepsis, hypotension, major surgery, trauma, severe metabolic, endocrine, and electrolyte abnormalities, or uncontrolled epilepsy) should not be used.
Effects on the liver
Same as otherHMG–CoA As with reductase inhibitors, excessive alcohol consumption and/ or a history of liver disease should be used with caution. Liver function tests are recommended before starting treatment and for the first 3months after initiation. If serum transaminases are elevated above the upper limit of normal3fold, the product should be discontinued or the dose reduced.
For hypercholesterolemia secondary to hypothyroidism or nephrotic syndrome, the primary disease should be treated prior to initiating treatment with this product.
People
Pharmacokinetic studies have shown higher drug exposure in Asian subjects than in Caucasian subjects.
Protease inhibitors
Increased systemic exposure to resulvastatin has been observed in subjects receiving the combination of resulvastatin and a different protease inhibitor (in combination with ritonavir). Full consideration should be given to the lipid-lowering benefit of this product in HIV patients treated with protease inhibitors and to the possibility that in combination with protease inhibitor therapy, resulvastatin The potential for elevated plasma concentrations of resulvastatin Combination with protease inhibitors is not recommended unless the dose of this product is adjusted.
Lactose intolerance
With rare genetic galactose intolerance, lactase deficiency, or glucose–galactose malabsorption should not be taken by patients with rare hereditary galactose intolerance, lactase deficiency, or glucosegalactose malabsorption. –
Interstitial lung disease
Rare cases of interstitial lung disease have been reported in some statin therapy, especially in those on long-term treatment. Presenting features include dyspnea, a dry cough without sputum, and a decline in general health status (malaise, weight loss, and fever). Patients should discontinue statin therapy when interstitial lung disease is suspected.
Diabetes mellitus
Reports have shown thatdiabetes family:Times New Roman”>3-hydroxy-3-methylglutaryl coenzymeA(3-hydroxy-3-methyl glutaryl coenzyme A, HMG-CoA) reductase inhibitors (including this product) are used with glycated hemoglobin ( >Glycated haemoglobin A1C, HbA1c) and elevated fasting serum glucose levels.
Risk patients (fasting glucose:5.6) should be treated according to the relevant guidelines. -family:equivocal”>to6.9 mmol/L,,BMI >30 kg/m2, elevated triglycerides, hypertension) for clinical and biochemical monitoring.
Pediatric patient population
For patients aged 10-17years old,Tennerstage in Pediatric patients with maturation of secondary sexual characteristics according to linear growth (height), weight,BMI (Body Mass Index) was assessed for a limited period of one year on Rosuvastatin. After 52 weeks of study treatment, the effects on growth, weight, BMI or sexual maturation. Experience with clinical trials in pediatric and pediatric patients is limited, and the long-term (>1year) treatment effects of resulvastatin in adolescent patients are not known.
Children and adolescent patients treated with resulvastatin over a period of52week clinical trial found creatine kinase elevations greater than10×ULN, and the muscle symptoms observed after concomitant exercise or enhanced physical activity, than those performed in adults The frequency observed in clinical trials was higher. (See “Adverse Reactions”).
Effects on driving vehicles and operating machines
Studies to determine the effect of this product on driving vehicles and maneuvering machines have not been performed. However, based on the pharmacodynamic properties, it is unlikely that this product will affect these abilities. When driving vehicles and maneuvering machines, consideration should be given to the possibility that dizziness may occur during treatment.
[For pregnant and lactating women]
This product is contraindicated in pregnant and lactating women.
Women at risk of pregnancy should use appropriate contraception.
Because cholesterol and other cholesterol biosynthesis products are important for embryonic development, the cholesterol from HMG-CoA reductase inhibition outweighs the benefits of treatment for pregnant women. Animal studies have provided limited evidence of reproductive toxicity. If a patient becomes pregnant while using this product, treatment should be discontinued immediately. Rosuvastatin is secreted into rat milk. There is no information on the secretion of Rosuvastatin into human milk.
[Pediatric Use]
The safety and efficacy of this product in children have not been established. Experience with pediatric use is limited to a small number (age ≥8years) of children with pure-sibling familial hypercholesterolemia. Therefore, pediatric use of this product is not currently recommended.
[Geriatric Use]
No need to adjust the dose according to age. In clinical studies10,275 patients taking this product,3159 patients (31%)≥65 years old,698 (6.8% )≥75 years of age. The overall safety and efficacy of these two populations did not differ from those of younger subjects. Other reports of clinical use experience also show no differences between the older and younger populations. However, it cannot be excluded that some older patients are more sensitive to the drug and that advanced age is a predisposing factor for myopathy, so caution should be exercised when applied to the older population.
[Drug Interactions]
Combination of drugs on Rosuvastatin
Transporter protein inhibitors: Rosuvastatin is a substrate for certain transporter proteins, including hepatic uptake of transporter proteinsOATP1B1and efflux transporter proteinBCRP< span style="font-family:equinox">. This product may cause increased plasma concentrations of resulvastatin and increased risk of myopathy (including rhabdomyolysis) when used in combination with the above mentioned transfer protein inhibitor medicinal products. Consider alternative medications when possible and, if needed, temporarily discontinue treatment with this product. When the combination of these drugs with this product is unavoidable, the benefits and risks of coadministration and dose adjustment of this product should be carefully considered.
Cyclosporine: When this product is combined with cyclosporine, theAUC of resulvastatin span style=”font-family:equivocal”>was on average7fold higher than that observed in healthy volunteers (compared with those taking the same dose of this product). The combination does not affect the plasma concentration of cyclosporine. This product is contraindicated in patients receiving concomitant cyclosporine therapy.
Protease inhibitors: Although the mechanism of drug interaction is unclear, concomitant administration of protease inhibitors may substantially increase exposure to resuprastatin. In pharmacokinetic studies, concomitant administration of this product10 mgwith a combination containing two protease inhibitors in healthy volunteers ( 300 mgazanavir/ 100 mgritonavir), the results showed that theAUC of resulvastatinandCmaxvalues were elevated by approximately3fold and7< span style="font-family:equinox">fold. Caution should be exercised with the combination of protease inhibitors after adjustment of this product dose based on the expected increased exposure to resulvastatin (see [Precautions]).
Gefeberzil and other lipid-lowering products: Concomitant use of this product with gemfibrozil may result in an C dose of resupivastatin Roman”>CmaxandAUCincreased2fold.
No pharmacokinetic interactions with fenofibrate are expected based on information from dedicated interaction studies, but pharmacodynamic interactions may occur.
Giffibezil, fenofibrate, other fibrates, and lipid-lowering doses (≥1g/day) of niacin in combination with HMG-CoAreductase inhibitors increased the risk of myopathy This may be due to their ability to cause myopathy when administered alone.
Ezetimibe: In hypercholesterolemic subjects, this product10 mgand ezetimibe10 mgof combined dosing resulted in an increase in the AUCof resuprastatin1.2fold. Adverse reactions due to pharmacodynamic interactions between this product and ezetimibe cannot be excluded.
Antacids: Simultaneous administration of this product and an antacid suspension containing magnesium aluminum hydroxide reduced the plasma concentration of resuprastatin by approximately50% if the plasma concentration of resulvastatin is reduced after administration of this product2hours after administration of antacids, this effect may be reduced. The clinical significance of this drug interaction has not been studied.
Erythromycin: The combination of this product with erythromycin resulted in an AUC for resulvastatindecrease20%, < span style="font-family:Times New Roman">Cmaxdeclinedecline30%. This interaction may be due to the increased gastrointestinal motility caused by erythromycin.
CytochromeP450 P450 P450 =”font-family:equinox”>Enzyme: Data from both in vitro and in vivo studies show that resuprastatin is neither a cytochromeP450P450 “font-family:equinox”>isoenzyme inhibitor, nor is it an enzyme inducer. In addition, Rosuvastatin is a weak substrate for these enzymes. Rosuvastatin is compatible with fluconazole (CYP 2C9 and CYP 3A4 or ketoconazole (CYP 2A6< span style="font-family:equivocal">andan inhibitor of CYP 3A4) did not have a clinically relevant interactions.
Colchicine: There have been reports of interactions between, including resulvastatin family:Times New Roman”>HMG-CoAreductase inhibitors in combination with colchicine have been reported to occur myopathies including rhabdomyolysis; therefore, caution should be exercised when combining this product with colchicine.
Interactions requiring dosage adjustment of Rosuvastatin:
Dose adjustment should be made when combined with drugs known to increase exposure to this product. Expected exposure (AUC) increases by approximately2fold or higher, the starting dose of this product is5 mgonce daily.
The maximum daily dose of this product should be adjusted so that the expected exposure to resulvastatin does not exceed the exposure level at the maximum recommended dose.
|
Published clinical trials on the effect of combination dosing on exposure to resulvastatin (AUC< span style="font-family:equine">; in descending order) |
||||
|
Dosing regimens for interacting drugs > |
Risulvastatin dosing regimen |
Risulvastatin< span style="font-family:Times New Roman">Variation in AUC * |
||
|
Cyclosporine75 mg BID~ 200 mg BID,,6months |
10 mg OD,,10 days |
7.1times |
||
|
Atazanavir300 mg/ritonavir100 mg OD,,8days |
10 mg, single dose |
3.1times |
||
|
Simeprevir 150mg OD,7days |
10mg, single dose |
, single dose | , single dose |
2.8< span style="font-family:equals">times |
|
Lopinavir400 mg/ Ritonavir100 mg BID,< 17days |
20 mg OD,< span style="font-family:Times New Roman">7days |
2.1timestimes /span> |
||
|
Clopidogrel300mgload,24hours after maintenance dose75mg |
20mg, single dose |
2times |
||
|
< span style="font-family:equivocal">Giffibenzi600 mg BID,< span style="font-family:Times New Roman">7days |
80 mg, single dose |
1.9times |
||
|
Eltrombopta75 mg OD, 5days |
10 mg , single dose |
1.6times |
||
|
Darunavir600 mg/ritonavir100 mg BID,,7days |
10 mg OD,,7 days |
1.5times |
||
|
Tilanavir500 mg/ritonavir200 mg BID,,11days |
10 mg, single dose |
1.41.4 =”font-family:equals”> times |
||
|
Decidual Nedarone400 mg BID |
Not applicable |
1.41.4 =”font-family:equals”> times |
||
|
Itraconazole200 mg OD, 5days |
10 mg, single dose |
1.4times** |
||
|
Ezetimibe10 mg OD,< span style="font-family:Times New Roman">14 days |
10 mg,,OD,14day |
1.2times** |
||
|
Fosamprenavir700 mg/ritonavir100 mg BID,,8days |
10 mg, single dose |
“ |
||
|
Agreza< span style="font-family:Times New Roman">Aleglitazar 0.3 mg,, 7days |
40 mg,7< span style="font-family:equinox">day |
“ |
||
|
Silybin140 mg TID,5days |
10 mg, single dose |
10 mg, single dose |
“ | |
|
Fenofibrate67 mg TID, 7 days |
10 mg,7days |
“ |
||
|
Rifampin450 mg OD,77 “font-family:equinox”>day |
20 mg, single dose |
“ |
||
|
Ketoconazole 200 mg BID, 7 days |
80 mg< span style="font-family:equinox">, single dose |
“ |
||
|
Fluconazole200 mg OD,11days |
80 mg, single dose |
80 mg, single dose |
“ | |
|
Erythromycin500 mg QID, 7 days |
80 mg, single dose |
20%¯ |
||
|
Scutellarin50 mg TID,14day |
20 mg, single dose |
47%¯< /p> |
||
|
*shown in the textxfold change data represent simple ratios for combined dosing and resulvastatin alone, as shown in the text%< /span>variation represents the difference relative to the use of Rosuvastatin alone%. respectively with ““, “““and“¯“indicates increase, no change, and decrease. **Several interaction studies have been performed with different doses of this product and the data shown in this table are the most The data shown in this table are the most significant ratios. OD = once daily;BID = twice-daily;TID = three times a day;QID = four times a day | ||||
Risulvastatin on Combined Medications< span style="font-family:Times New Roman">
VitaminKAntagonists: same as otherHMG–CoAreductase inhibitors, for concomitant use of vitamin Kantagonists (e.g., warfarin or other coumarin-based anticoagulants), initiation of this product or gradual increase in the dose of this product may result in an international normalized Ratio (INR) to increase. Discontinuation of this product or gradual reduction in the dose of this product may result in a decrease in INR. In this case, proper detection of INR is required.
Oral contraceptives/hormone replacement therapy (HRT).
Concurrent use of this product and oral contraceptives resulted in AUC of ethinylestradiol and norethindrone -family:equivocal”>increased by 26%and, respectively, and 34%. These elevated blood levels should be considered when selecting the dose of oral contraceptives. No pharmacokinetic data are available for subjects using both this product and HRT; therefore, a similar interaction cannot be excluded. However, in clinical trials, this combination was widely available and well tolerated by patients.
Other drugs:
No clinically relevant interactions with digoxin have been estimated based on data from dedicated drug interaction studies.
Fusidic acid: No studies have been conducted on the drug interaction between resuprastatin and fusidic acid. As with other statins, muscle-related events (including rhabdomyolysis) have been reported in post-marketing experience with the combination of resulvastatin and fusidic acid.
Therefore, combining resulvastatin with fusidic acid is not recommended. If possible, temporary discontinuation of resulvastatin therapy is recommended. If combination cannot be avoided, the patient should be monitored closely.
Other drugs that may interact with statins include telithromycin, nefazodone, and amiodarone.
Pediatric patient population: Interaction studies have only been performed in adults, and information on interactions in the pediatric population is not yet available.
[Drug overdose]
There is no specific treatment for overdose of this product. Once an overdose occurs, symptomatic treatment should be given, with supportive measures if needed. Liver function and creatine kinase levels should be monitored. Hemodialysis may not be significantly effective.
[Pharmacology and Toxicology]
Pharmacological effects
Risulvastatin is a selective, competitiveHMG-CoA span style=”font-family:equinox”>reductase inhibitor. HMG-CoA< span style="font-family:isoline">reductase is3-hydroxy-3-Methylglutaryl coenzymeA is the rate-limiting enzyme in the conversion to mevalonate, a precursor of cholesterol. The results of animal tests and cell culture assays showed that risuvastatin is highly and selectively taken up by the liver, which is the target organ for cholesterol-lowering effects. Results from in vivo and in vitro tests showed that resrivastatin increased the number of hepaticLDLreceptors on the cell surface, thereby enhancing the effect on< span style="font-family:Times New Roman">LDL uptake and catabolism, and inhibit hepaticVLDLVLDL synthesis, thereby reducingVLDLandLDLparticles in total.
For patients with pure and heterozygous familial hypercholesterolemia, patients with nonfamilial hypercholesterolemia,
mixed dyslipidemia, and resulvastatin reduces total cholesterol,LDL-C,ApoB, non, non family:Times New Roman”>HDL-Clevels. Rosuvastatin also lowersTG, elevatesHDL-C levels. In patients with simple hypertriglyceridemia, resulvastatin reduces total cholesterol,LDL-C,VLDL-C,ApoBApoBApoB span>, nonHDL-C, < span style="font-family:Times New Roman">TGlevels and elevatedHDL -Clevels. The effect of resulvastatin on cardiovascular morbidity and mortality has not been determined.
Toxicological studies
Central nervous system toxicity
Found in several dog trials of similar drugsCNS =”font-family:equine”>vascular injury, as seen by perivascular hemorrhage, edema, and perivascular mononuclear cell infiltration. A drug structurally similar to this class of drugs at plasma drug concentrations in dogs higher than the mean concentration at the maximum recommended human dose30 times the dose, showed dose- dependent optic nerve degeneration (retinal-knee fiberWalleriandegeneration).
1female dog given transoral resulvastatin90 mg/kg/day (at AUCprojected whole-body exposure equivalent to a human40 mg/day exposure100 times), the first24day euthanasia due to near death was seen with interstitial edema, hemorrhage and partial necrosis of the choroid plexus. Dogs were given transoral resulvastatin6 mg/kg/day (at AUC extrapolated to a whole body exposure equivalent to human40mg/ day exposure20times), continuous< span style="font-family:Times New Roman">52weeks, and corneal clouding was seen. Dogs were given transoral resulvastatin30 mg/kg/day (at AUC extrapolated, the whole body exposure is equivalent to human40mg/ 60fold of the daily exposure), continuous< span style="font-family:Times New Roman">12weeks, and cataractogenesis was seen. Dogs were administered resulvastatin90 mg/kg/day orally (at AUC extrapolated, systemic exposure is equivalent to human40mg/ day exposure100times), continuous< span style="font-family:Times New Roman">4weeks, retinal dysplasia and retinal detachment were seen. Dogs at doses ≤30 mg/kg/day (at AUC extrapolated to a whole body exposure equivalent to human40mg/60fold of the daily exposurewhen administered continuously< span style="font-family:Times New Roman">1year, no effect on the retina was seen.
Genotoxicity
Risulvastatin inAmestest, mouse lymphoma test,CHLcell chromosome aberration test, and mouse micronucleus test were negative.
Reproductive toxicity
In the rat fertility test, male rats were found to be 9fertilized since before matingweek to mating, and female rats from 2week before mating to the firstweek of gestation. span>7days to be given orally5,15,< span style="font-family:Times New Roman">50mg/kg/day at the highest dose (at AUC extrapolated to a systemic exposure equivalent to human40 mg/day exposure10fold), with no adverse effects on fertility seen. Dogs given transoral resulvastatin30 mg/kg/day continuously1month, giant spermatocytes were seen in the testes (Spermatidic giant cell). Monkeys were given transoral resulvastatin30 mg/kg/day continuously6months, and vacuolization of giant spermatocytes and vas deferens epithelium was seen. The above doses in dogs and monkeys are equivalent to human40 mg/day, respectively, extrapolated from body surface area. font-family:Times New Roman”>20fold and10fold. A similar phenomenon was seen with similar drugs.
Female rats before to after mating77day given via mouth5,15, 50mg/kg/day, and the high-dose group (at AUCextrapolated, systemic exposure equivalent to human40mg/day of exposure10. span>fold) was seen in fetal litter weight loss and delayed ossification.
Rats from gestation day 7 to lactation day . day to breastfeeding day 21(lactation) given transorally2,10, 50mg/kg/day, high dose group (extrapolated by body surface area, greater than or equal to human40mg/day of12 >times) was seen to decrease the survival rate of the pups. The survival rate of the rabbits was reduced from day 6of gestation to day 18of lactation. New Roman”>18days (lactation) given orally0.3day0.3 family:isoline”>,1,3mg/kg/day (extrapolated from body surface area, compared to human40mg/< span style="font-family:equinox">days), a decrease in fetal litter survival and maternal animal mortality was seen. Rosuvastatin doses in rats≤25mg/kg/day, rabbitsday, and rabbits≤3mg/kg/day did not show teratogenicity (respectively by AUC >and body surface area extrapolated to human40 mg/day of exposure (equivalent).
Carcinogenicity
in rats104week carcinogenicity assay in rats at oral administration doses of2, 20,60 = “font-family:equinox”>, 80mg/kg/day. 80mg/kg/day (based on AUC extrapolated to a whole body exposure equivalent to a human40 mg/20fold of the humanday exposure, while no increase was observed at the lower dose. No increase in incidence was seen at lower doses.
In mice107 weeks In the carcinogenicity test, the doses administered orally were10, 60,200mg/kg/day. 200mg/kg/day (based on AUC extrapolated to a whole body exposure equivalent to a human40 mg/20day exposure dose group, with no increased incidence seen at the lower dose. No increased incidence was seen at lower doses.
[Pharmacokinetics]
Results of pharmacokinetic studies completed abroad:
Absorption: This product was administered orally5< span style="font-family:equinox">hours after peak blood concentration. Absolute bioavailability is 20%.
Distribution: Rosuvastatin is heavily taken up by the liver, which is responsible for cholesterol synthesis and LDL-Cclearance is the major site of LDL-Cclearance. The volume of distribution of resulvastatin is approximately 134L. The plasma protein binding rate (mainly albumin) of Rosuvastatin is about 90%.
Metabolism: Limited metabolism of Rosuvastatin occurs (approximately10%). In vitro metabolism studies using human hepatocytes have shown that resuprastatin is a weak substrate for cytochromeP450 metabolism. The major isoenzyme involved in metabolism is CYP 2C9,2C19,3A4, and 2D6 are involved in metabolism to a lesser extent. The known metabolites are Nposition demethylation and lactone metabolites. Nsite demethylated metabolites were less active than resulvastatin50%, while the lactone metabolite is considered to be clinically inactive.
on circulating HMG-CoAreductase inhibitory activity,90% or more from resulvastatin.
Excretion: approximately90% of the dose of Rosuvastatin is excreted in its original form in the feces (both absorbed and unabsorbed active substances), with the remainder excreted in the urine. Approximately5% of the urine is in its original form. The plasma clearance half-life is approximately 19hours. The clearance half-life does not increase with dose, and the geometric mean of plasma clearance is approximately 50L/hour (coefficient of variation of < span style="font-family:Times New Roman">21.7%). As with other HMG-CoAreductase inhibitors, hepatic uptake of resuprastatin involves membrane transporters style=”font-family:Times New Roman”>OATP-C. This transporter is important in the hepatic clearance of resupristatin.
Linear: The systemic exposure to Rosuvastatin increases proportionally with dose. Pharmacokinetic parameters are unchanged after multiple dosing.
Only about 10% of rasuvastatin undergoes metabolism, primarilyNsite demethylation.
Special Populations:
Age and Gender: Age or gender does not have a clinically meaningful effect on the pharmacokinetics of Rosuvastatin.
Renal insufficiency: In a study of patients with varying degrees of renal impairment, mild and moderate renal disease had no clinically meaningful effect on the pharmacokinetics of resulvastatin orN-demethyl metabolite had no effect on plasma concentrations. However, compared with healthy volunteers, patients with severe renal impairment (creatinine clearance<30mL/min) had increased blood concentrations3fold,N- demetabolite blood levels increased9 times. Steady-state blood concentrations of reseruvastatin were approximately50% higher in hemodialysis patients than in healthy volunteers.
Hepatic insufficiency: In a study of patients with varying degrees of hepatic impairment, there was no evidence of Child-Pugh scores did not exceed7 subjects had elevated exposure. However, 2examples of Child-Pugh scores of 8 and9 patients who had greater exposure to resuprastatin than thoseChild-Pughscore values were increased by at least2fold. There are no Child-Pugh scores over 9 of the subjects’ experience with the use.
Genetic polymorphisms:HMG-CoACatabolism of reductase inhibitors (including resulvastatin) involvesOATP1B1andBCRP transporter proteins. SLCO1B1(OATP1B1) and/orABCG2(BCRP) genetic polymorphism in patients at risk for increased exposure to resulvastatin. WithSLCO1B1 c.521TT orABCG2 c.421CC genotype patients compared toSLCO1B1 c.521CC andABCG2 c.421AA Patients with genetic polymorphisms are more likely to have elevated exposure to resulvastatin (AUC). Although this particular genotypic profile has not been established in clinical practice, a lower daily dose of this product is recommended for patients with the known genetic polymorphisms described above.
Ethnicity: Foreign pharmacokinetic studies have shown that the area under the blood concentration-time curve in Asian (including Chinese) subjects (AUC) median and peak concentration (C) sub>max) is about 2fold. Population pharmacokinetic analysis showed no clinically relevant differences in pharmacokinetics in Caucasian and black groups.
Results from a pharmacokinetic study in healthy Chinese volunteers in China:
This study was conducted on5,10,20 mg of Rosuvastatin calcium tablets after single and multiple doses were measured for pharmacokinetic parameters in healthy Chinese volunteers. After a single dose,tmax the median values ranged from2.5–5. span>hours, followed by an exponential decrease. The half-life (t1/2) is . family:Times New Roman”>11to12hours or so. Steady-state blood levels were reached on day 3 of multiple dosing. Drug accumulation after multiple doses was minimal and dose-independent.
This study, along with previous pharmacokinetic studies completed in Singapore and the United States in healthy Chinese volunteers, determined the pharmacokinetic properties of resupivastatin calcium in healthy Chinese volunteers. In these three studies, the pharmacokinetic parameters of resulvastatin calcium were similar.
[Storage]Seal and store in a dry place.
[Package]Packaged in aluminum and plastic, per plate7tablets,10tablets per box< span style="font-family:Times New Roman">1plate,2 board.
[Expiration date]24 “font-family:equals”>months
[Executive Standard]
[Approval number](1< span style="font-family:equinox">)5mg:国药准字H20143337 (2)10mg:国药准字 >H20143338
[Marketing Licensee]
Company name: Hazen Pfizer Inc
HISUN PFIZER PHARMACEUTICAL CO.
Land
Address: Haizheng Road, Xukou Town, Fuyang City, Zhejiang Province2No.
Postal Code:311404
Phone Number:4006236717
[Manufacturer]
Zhejiang Haisheng Pharmaceutical Co.
ZHEJIANG HISUN PHARMACEUTICAL CO.
Manufacturing Address: Waisha Road, Jiaojiang District, Taizhou City, Zhejiang Province46No.
Postal Code:318000
Phone Number:4001180618
Fax Number:0576-88827887