What is an “isolated pulmonary nodule”?
The term “solitary pulmonary nodule” refers to a single pulmonary nodule less than 3 cm in diameter.
A solitary pulmonary nodule (SPN) is a solitary lung lesion less than 3 cm in diameter that is surrounded by lung tissue and is not associated with other abnormalities of the lung or nearby lymph nodes.
Isolated pulmonary nodule, how can you tell if it is benign or malignant?
It is possible for an isolated lung nodule to be lung cancer, and it is important to distinguish between benign and malignant as quickly and accurately as possible for subsequent treatment decisions.
Providing helpful information to your doctor
To help the doctor determine how benign or malignant a nodule is, the patient should tell the doctor the following information:
- Age: The risk of malignancy increases with age, with a 3% risk of cancer at ages 35-39; a 15% risk at ages 40-49; a 43% risk at ages 50-59; and a risk of more than 50% at ages 60 and older.
- History of smoking: increased likelihood of malignancy.
- History of cancer: Higher chance of malignancy with previous cancer in other parts of the body.
- History of occupations and travel at high risk for lung cancer
- Have occupational risk factors for lung cancer: exposure to asbestos, radon, nickel, chromium, vinyl chloride, and polycyclic hydrocarbons increases the likelihood of malignancy.
- Travel history: higher chance of benignity having traveled in areas with endemic fungal disease (such as histoplasmosis, coccidioidomycosis, or budding mycosis), or areas with high prevalence of tuberculosis.
- History of tuberculosis or pulmonary fungal disease has a higher chance of benignity.
Imaging
Thoracic CT scan is important for the diagnosis of benign and malignant isolated pulmonary nodules.
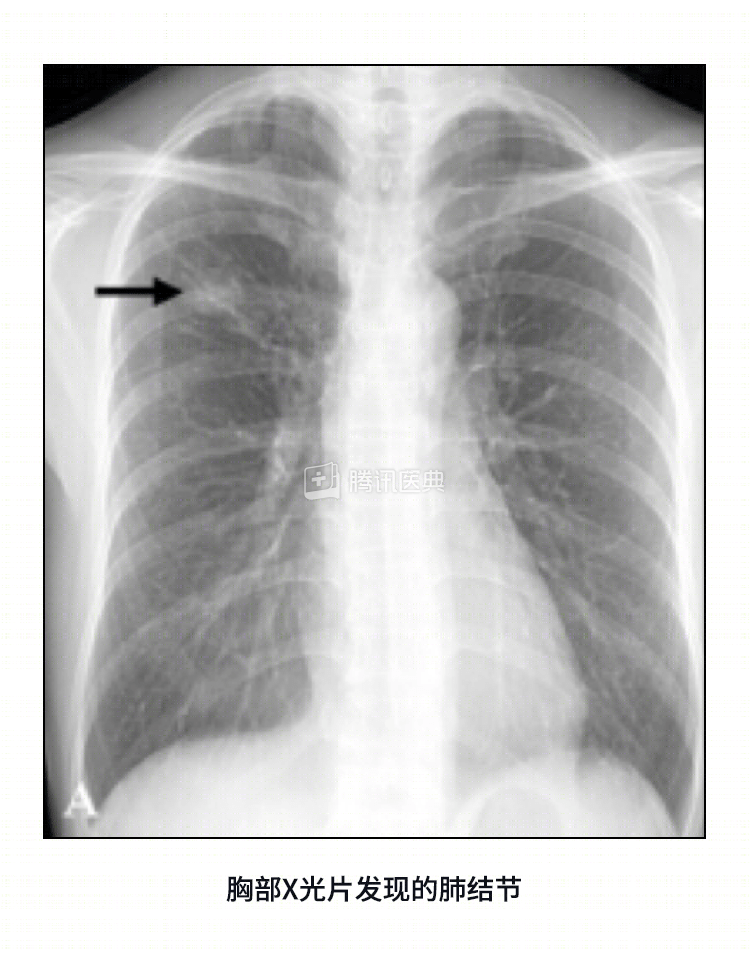
Chest x-ray
Chest X-rays are often difficult to detect for small pulmonary nodules, especially those with a ground-glass component, and are not generally recommended for screening of small pulmonary nodules in the early stages.
CT scan
It is very helpful in identifying the features of the nodule and in confirming the diagnosis of cancer, helping to distinguish a tumor from an infected lesion, and if the CT scan shows fat within the nodule, the nodule is usually benign, which is a specific feature of a benign nodule.
CT scans have the following advantages over chest X-rays:
- Higher resolution: Nodules as small as 3-4 mm can be detected, allowing the physician to see the nodule’s features.
- Better localization: the location of the nodule can be determined more accurately.
- Better visualization of areas that are difficult to evaluate with X-rays.
- Can provide more detail of internal structures and more easily show calcifications.
Positron emission tomography (PET)
- Malignant cells require more energy and consume more sugar than normal cells and benign lesions, and PET measures sugar consumption by tracking radioactive markers that are identified on three-dimensional color images.
- PET scanning is a more accurate test, but it is expensive.
Single-photon emissioncomputed tomography (SPECT)
- SPECT scans are imaged using the radiolabeled substance technetium Tc P829.
- SPECT scans are less expensive than PET scans but have essentially similar sensitivity and specificity, except that the test has not been evaluated on a large scale and is not widely available, and in addition, SPECT is less sensitive to nodules smaller than 20 mm in diameter.
Biopsy
Doctors use different methods to remove nodule cell samples for examination under the microscope.
- Bronchoscopy: This test is used to diagnose nodules that grow close to the wall of the bronchi. The bronchoscope is a soft, thin tube with a tiny camera at one end that enters the trachea through the mouth or nasal cavity and then into the bronchi.
- The doctor takes a biopsy sample from the nodule, and if the lesion is not easily accessible in the bronchial wall or is less than 2 cm in diameter, a puncture biopsy, known medically as transbronchial needle aspiration (TBNA), may be performed.
- Transthoracic needle aspiration (TTNA)
- If the nodule is located at the edge of the lung, a biopsy sample must be obtained with the help of a puncture needle that passes through the chest wall and into the nodule, which is usually guided by CT.
- The accuracy of TTNA is as high as 90-95% for nodules larger than 2 cm in diameter and decreases to approximately 60%-80% for nodules smaller than 2 cm in diameter.
- Video-assisted thoracoscopy (VATS)
- The surgeon inserts the thoracoscope through a small incision in the chest wall to perform the examination, and a miniature camera takes pictures of the lungs, which are displayed on a TV screen outside the body, and the surgeon performs the procedure with the aid of the display.
- This approach not only helps to confirm the diagnosis of a nodule, but can also be used to remove it.
Blood tests
For isolated pulmonary nodules (SPN), blood tests are not diagnostic, but the following tests may be informative for diagnosis, especially in ruling out benign tumors such as tuberculosis:
- Anemia (low hemoglobin levels) or an elevated erythrocyte sedimentation rate (the rate at which red blood cells settle in anticoagulated blood) may indicate cancer or an infectious disease.
- Elevated liver enzymes, alkaline phosphatase, or serum calcium levels may indicate cancer and metastasis in isolated lung nodules, or cancer that has metastasized to the lungs from another part of the body.
- Histoplasmosis and tuberculin skin test
- Patients with histoplasmosis (an infection due to inhalation of spores of Histoplasma capsulatum) or coccidioidomycosis (a common disease in the southwestern United States in which a person exhales fungal spores dispersed in the soil and causes a lung infection) may have high levels of fungal-specific immunoglobulin G and immunoglobulin M antibodies.
- Tuberculin skin test: The physician injects tuberculin antigen into the skin and observes the body’s response; if the injection site is red and swollen, it may be caused by tuberculosis.
.
Related reading:
Co-reviewed by: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Dong Song Dr. Zhang Chao.