It’s time for a thoracoscopy. What is the procedure for this exam? Is it painful? How do I need to cooperate? This article talks about these questions that you may have.
What do I need to do to prepare for the test?
The doctor will take a medical history to fully assess your health. Tests will include routine blood work, liver and kidney function, coagulation and other hematology tests, as well as an electrocardiogram and lung function.
The doctor will give you and your relatives a detailed description of the purpose, method, procedure, possible results and possible risks of the test, and ask you to sign an informed consent form.
Before the examination, you should regulate your physical and mental state, relax and not be too nervous, and receive psychological counseling from nurses and related professionals if necessary.
It is also important to get enough sleep and eat well. The night before the test, don’t eat or drink anything after ten o’clock. If you are also diabetic, it is important to keep your blood sugar stable before the exam to help the wound heal. You will need to abstain from food and water the morning of the exam.
The doctor will then select the appropriate puncture site on your body and mark the surface of your body, and you will cooperate with the doctor.
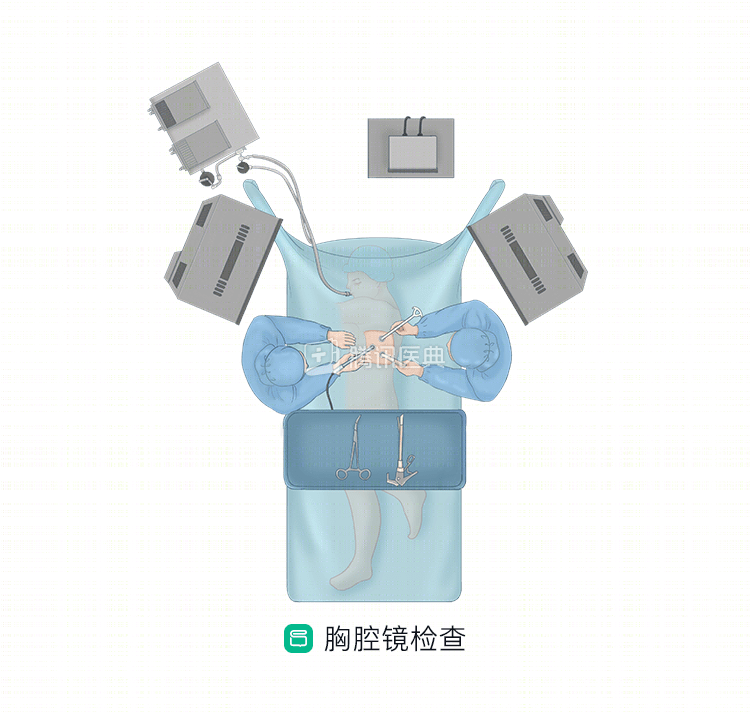
How is the test performed?
Once the preparation is complete, it’s time to go into the operating room for the specific procedure.
Thoracoscopy is performed under general anesthesia. The anesthesia is usually a general anesthesia with a double-lumen tube insertion, with one lung ventilated and the lung on the side of the procedure unventilated for observation and examination and treatment.
Internal thoracoscopy
In internal thoracoscopy, the physician makes a small incision of about 1 cm at a pre-marked puncture site, bluntly separates the subcutaneous layers to the pleura, places a puncture device, and delivers the thoracoscope through the trocar into the pleural cavity, at which point the treatment can be observed in detail.
During the examination, the surgeon will look at the entire pleural cavity in the order of internal, anterior, superior, posterior, lateral, and inferior, while taking a sample biopsy at the lesion. If there is a malignant pleural effusion, it will be aspirated first and then a pleural biopsy will be performed and fixed.
After completion, a drainage tube is placed. This is because the integrity of the pleura has been compromised, and a chest tube needs to be placed at the puncture site to assist with drainage, maintain negative pressure in the chest cavity, and allow the lung to expand. The doctor assesses what needs to be done by observing the amount and color of the drainage.
Surgical thoracoscopy
Surgical thoracoscopy is performed in much the same way as internal medicine. If the preoperative surgeon determines that management and treatment of pleural disease may be needed, such as an isolated small pleural tumor that can be removed at the same time as the examination, the surgeon will need to place several instruments through the puncture holes (which may be larger, or 1 to 2 more operative holes, than in medical thoracoscopy) to complete the various thoracoscopic maneuvers.
After the procedure is completed and the tube is drained, you will be resuscitated and extubated in the resuscitation room. You may wake up to find an additional tube (drainage tube) in your chest wall. There will be some discomfort after the operation, such as pain and chest tightness. Generally, after 1 to 2 days, the drainage tube can be removed when the doctor observes that no significant gas or fluid is being removed and a repeat chest X-ray confirms that the lung has expanded. After the tube is removed, the chest pain will be significantly relieved.
Co-reviewed by Dr. Dong Song Dr. Zhang Tao, Guangdong Provincial People’s Hospital, Guangdong Lung Cancer Institute, Deputy Chief Physician Liao Rijiang