- Oxitinib, a third-generation EGFR TKI that has been approved for marketing in China in March 2017, can better overcome the resistance of the first/second-generation EGFR TKI represented by EGFR T790M mutation. Clinical studies have also confirmed definitive efficacy in patients with brain metastases.
- On April 18, 2018, the FDA officially approved axitinib for the first-line treatment of patients with metastatic NSCLC with EGFR-sensitive mutations (exon 19 deletion or exon 21L858R mutation). Our 2018 Chinese Society of Clinical Oncology guidelines for lung cancer include oxitinib as one of the optional strategies for the first-line treatment of advanced EGFR mutation-positive NSCLC.
- Oxitinib is more expensive, and despite the China Charity Federation’s charity assistance program launched less than a month after approval, the financial burden of using the drug is still not light. If you pay 50,000 RMB per month out-of-pocket, you get 8 months after 4 months of use, which translates to 200,000 RMB per year.
.
Why was axitinib created?
Gefitinib, erlotinib, and other first-generation EGFR-TKI (epidermal growth factor receptor-tyrosine kinase inhibitors) drugs have brought significant benefit to patients with advanced non-small cell lung cancer (NSCLC) with sensitive mutations, but drug resistance is an inevitable problem. In addition to the original mutation, 50%-60% of drug resistance is caused by tumor cells newly developed mutations in the EGFR T790M locus, which in turn escape drug attack.
Osimertinib is a third-generation EGFR TKI that was approved for marketing in China in March 2017.
Osimertinib (AZD9291, trade name Theresa) inhibits both EGFR-sensitive mutations and T790M, so it can better overcome the resistance of the first/second generation EGFR TKI represented by EGFR T790M mutation. Clinical studies have also demonstrated definitive efficacy in patients with brain metastases.
What kind of patients are suitable for oseltinib?
The best drug is not a panacea.
A good drug is not a panacea, so don’t take it “blindly”.
To understand when to use axitinib, look at these two important studies – the AURA series and the FLAURA study.
(1) The AURA Series – First-Generation Targeted Drug Resistance Options
The AURA series of studies includes AURA, AURA2, and AURA3. Based on the results of AURA and AURA2, the FDA gave early approval to axitinib for second-line treatment of NSCLC patients carrying EGFR T790M mutations.
Based on this, the AURA3 conducted included a total of 419 patients with advanced NSCLC in 18 countries who had EGFR T790M mutation confirmed by tissue biopsy after failure of first-line EGFR-TKI therapy, and the results showed that ositinib was significantly superior to platinum/pemetrexed chemotherapy.
The median progression-free survival (mPFS) of 10.1 months for patients in the axitinib group was 5.7 months longer than in the two-drug chemotherapy group, reducing the risk of disease progression by 70%.
Once the use of oseltinib took effect, 49% of patients could be maintained for at least six months and 11% for at least one year. However, only 27% of patients in the chemotherapy group were maintained for up to six months and only 2% of patients were maintained for up to one year.
Of the 279 patients in the oseltinib group, 260 had controlled disease (93% disease control rate), 197 had significant tumor shrinkage (71% objective remission rate), and only 18 had no beneficial response to the drug, while of the 140 patients in the chemotherapy group, 104 had stable disease or remission (74% disease control rate), only 44 had significant shrinkage (31% objective remission rate), and 26 had There was no effect.
In summary, the clinical efficacy of oseltinib was significantly better than the current standard second-line treatment, platinum + pemetrexed chemotherapy. Therefore, the FDA approved axitinib for the second-line treatment of patients with EGFR T790M mutation-positive NSCLC.
In ARUA 3, 182 Asian patients (48 Chinese patients) have been enrolled, and two studies, AURA 17 and AURA 18, specifically validated the efficacy of oseltinib in the Asian population, with results similar to those of the global study, confirming the efficacy and safety of oseltinib in the Asian population.
Oxitinib was also successfully approved for marketing in China by the CDFA in March 2017, with a recommended daily oral dose of 80 mg.
(2) The FLAURA study – the future looks promising
Another important study of oxitinib was conducted to assess its efficacy in first-line treatment of patients with prime-stage advanced EGFR-sensitive mutation-positive disease.
The phase III clinical study FLAURA enrolled 556 EGFR mutation-positive, previously untreated patients with locally advanced or metastatic NSCLC in 30 countries and compared the efficacy and safety of first-line oseltinib with gefitinib/erlotinib. The results showed that oseltinib also beat its “predecessor” as a first-line regimen: oseltinib increased the time to tumor stabilization by up to 8.7 months and reduced the risk of disease progression by 54% over the first-generation TKI.
At 1 year post-treatment, up to 64% of patients in the axitinib group were still responding to treatment, and 49% at 1.5 years, compared to 19% of patients in the gefitinib/erlotinib group who were maintained to 1.5 years.
The disease control rate in the oseltinib group was 97% and the objective remission rate was 80%, while the disease control rate in the gefitinib/erlotinib group was 92% and the objective remission rate was 76%. They were similar in terms of efficiency, with oseltinib having a slight advantage.
Prolonged overall survival was the ultimate goal of treatment, with a survival rate of 83% in the oseltinib group and 71% in the control group at 18 months of treatment. According to the current incomplete clinical data, patients in the ositinib group had prolonged overall survival, but did not reach a statistical difference for the time being, so further follow-up is needed to observe patients in both groups.
Based on these results, in September 2017, the US NCCN guidelines have recommended oseltinib for first-line treatment, and on April 18, 2018, the FDA also officially approved oseltinib for first-line treatment of patients with EGFR-sensitive mutations (exon 19 deletion or exon 21 L858R mutation) in metastatic NSCLC. .
In China, the 2018 Chinese Society of Clinical Oncology CSCO lung cancer guidelines, include ositinib as one of the optional strategies for first-line treatment of advanced EGFR mutation-positive NSCLC.
In fact, there is a lot of controversy in academia about whether or not ositinib should be used for first-line treatment: for patients who develop T790M mutation resistance after first-line use of a first-generation TKI, it may be better to use a first-generation TKI followed by ositinib, but if the T790M mutation does not appear, first-line use of ositinib may be better.
The problem is that the probability of developing T790M is about 50%, and it is not yet known who will go down the path of T790M resistance.
It is important to note that using this arithmetic addition is not yet rigorous, but only provides an idea. Pending the publication of the overall survival results of the FLAURA study and further exploration of the mechanisms of resistance to oxitinib, there is still much room for development of how the trio of EGFR TKI will line up.
It is encouraging to see that as more and more drugs are developed, patients will have more choices and a future of “individualized” precision medicine with your physician to look forward to.
(3) Effectively crosses the blood-brain barrier, also for central lesions
Brain metastasis from lung cancer is a headache for doctors and patients alike, with 20% to 65% of lung cancer patients developing brain metastases during the course of their disease, resulting in a poor prognosis.
EGFR TKI, a class of small molecule drugs, can cross the blood-brain barrier better, but most of the cerebrospinal fluid concentrations are not as good as the drug concentrations in peripheral blood. Ocitinib has again proven itself with data.
Previous pooled analyses of AURA and AURA2 have shown that oseltinib can effectively cross the blood-brain barrier and better treat intracranial lesions. In the AURA3 study, the median PFS for those with CNS metastases was 8.5 months in the axitinib group compared to 4.2 months in the chemotherapy group (HR 0.32), meaning that patients in the axitinib group had double the PFS and 68% lower risk of disease progression than those in the chemotherapy group.
In the FLAURA study, the results of the subgroup analysis of brain metastases were equally promising, with a PFS of 15.2 months in the oseltinib group compared to 9.6 months in the gefitinib/erlotinib group. This suggests that oseltinib may be a better choice for the initial treatment of patients with EGFR mutations in the presence of brain metastases.
At this point, oseltinib may be a better choice than first-generation targeted agents for patients with brain metastases, regardless of whether they have T790M mutations.
How safe is oseltinib?
.
First, the AURA3 study: Ocitinib is better than chemotherapy drugs
The results of the AURA3 study showed that the most common adverse events were diarrhea (29%) and rash (28%) in the axitinib arm, compared with nausea (47%) and loss of appetite (32%) in the platinum-pemetrexed chemotherapy arm. Serious adverse events were significantly less in the oxitinib group than in the chemotherapy group (6% vs. 34%). However, it is important to note that there were 4 fatal events (2 respiratory failures, pneumonia, ischemic stroke) in the oxitinib group compared to 1 (hypovolemic shock) in the chemotherapy group.
Look again at the FLAURA study: Oxitinib is superior to the generation of targeted agents
The range of toxicities was similar between the two generations, with common side effects in the axitinib group including diarrhea (58%) and dry skin (32%), and common side effects in the control group were diarrhea (57%) and dermatitis acnes (48%). However, the frequency of serious adverse events was significantly lower in the oseltinib group (34% versus 45%).
How was the target identified – the T790M gene mutation?
.
(1) Tissue biopsy is most reliable
For patients with EGFR mutations, if resistance develops during treatment with a generation of targeted agents, be sure to re-puncture the tumor tissue if possible and obtain 15-20 white slices of pathologic tissue for gene sequencing. This is because the genes of tumor cells can change as the stress of therapy strikes, so be sure to re-biopsy to clarify the presence of emerging T790M mutations.
(2) Liquid biopsy is also feasible
In the AURA3 study, which compared the results of tissue and plasma EGFR mutations in 486 patients, the blood test was found to be highly specific and consistent with the tissue test, meaning that if a T790M mutation was detected in the blood, there was more than 90% certainty that it was also present in the tumor tissue. T790M is also present in the tumor tissue, at which point oxitinib can be administered directly.
However, the sensitivity of the blood test is poor, and only 51% of patients with positive tissue biopsies for T790M mutations have positive blood tests. Therefore, if a blood draw suggests no T790M mutation, it is still important to obtain a tumor tissue specimen by puncture if possible to confirm that ositinib is really not appropriate.
How should axitinib be administered?
.
(1) Timing and dosing
The recommended dose of axitinib is 80 mg daily and should be taken at the same time each day, whole and with water, either on an empty stomach or with a meal. If you are unable to swallow the drug, take the tablet dissolved in 50 mL of carbonate-free water.
(2) Can I take Ocitinib with other medicines?
.
Check with your primary care doctor before combining other medicines (including over-the-counter medicines, etc.). In particular, taking drugs such as carbamazepine, phenytoin, rifampin, and resulvastatin can affect the concentration of oxytetracycline in the blood, and you will need to discuss with your medical professional to decide on the dose of the drug.
(3) Don’t panic if you develop a rash, treat the symptoms
Adverse skin reactions are often a problem that affects the quality of life of many patients and can even lead to discontinuation of the drug in some patients, which is a pity. The appearance of a rash may be an indirect sign that the drug is working, and in previous studies of other EGFR-targeted drugs, the severity of the rash was found to correlate positively with efficacy. Rest assured, however, that the absence of a rash does not mean that the drug is ineffective.
- Prevention: Avoid sun exposure, keep your body clean, and apply a mild moisturizer, silicone cream, or vitamin E ointment after bathing to prevent dry skin.
- Mild rash.
- Mild rash: topical ointments such as dermaplanin and hydrocortisone can be used; for dry skin, thin phenol glycerin lotion can be given twice daily or benadryl ointment can be applied to the itchy area.
- Moderate rash: add oral loratadine to the above; for dry skin, apply benadryl ointment or compound benzoic acid ointment to the itchy area. In symptomatic patients, oral memantine 100 mg twice daily should also be given as soon as possible.
- Severe rash: Apply methylprednisolone and antibiotics if necessary, and reduce the dose. If adverse reactions do not resolve sufficiently after 2 to 4 weeks, consider suspending or discontinuing treatment.
.
(4) Seek medical attention when these conditions occur
- Fever (>38°C), chills;
- Diarrhea (4 to 6 times in 24 hours);
- nausea (interfering with eating and not relieved by symptomatic medication);
- Vomiting (more than 4-5 vomits in 24 hours);
- Sudden onset of shortness of breath with cough and/or fever; persistent cough or wheezing; shortness of breath;
- Yellowish staining of the skin or whites of the eyes; deepening or turning brown in the urine; loss of appetite; abdominal pain; easy bleeding or petechiae;
- Red or black asphaltic stools; hematuria.
Follow-up after axitinib dosing is as important as treatment
(1) Regular review to assess efficacy
When you take oseltinib for the indication, it’s not all good. Regular follow-up is as important as treatment, so don’t wait for something serious to happen before you see a doctor.
Always remember to keep a copy of the baseline imaging before starting treatment for subsequent comparative evaluation of efficacy. Patients taking the medication for the first time are generally recommended to be reviewed after the first month and then usually once every 2-3 months, but should be followed up promptly if there is worsening of symptoms or new onset of symptoms. At the time of follow-up, remember to inform the doctor of any recent discomfort or adverse reactions, and generally review 1 CT of the chest and abdomen every 3 months (CT scan and enhancement can be done alternately when the disease is stable to reduce radiation damage), 1 MRI of the brain every 6 months, and 1 bone scan every 1 year to assess the efficacy of treatment based on the results.
(2) Good documentation and a healthy mindset
To establish good communication with your doctor, try to keep him/her informed of all the medications and nutritional supplements you are taking, create a medication log, record changes in your body, and take good notes during your visits.
There is also no need to be overly stressed during treatment. Try to be positive. Although you need to make necessary adjustments to your life and work after the disease, you should not be too far away from your regular life, and you can continue to participate in community life; family members should also try to help reduce stress and make patients feel supported; trust your doctor and always ask for help from your treatment team.
Oxitinib is not perfect
(1) Expensive
Although the China Charity Federation launched a charity assistance program less than a month after the approval of axitinib, the financial burden of using the drug is still not light. The monthly out-of-pocket cost is 50,000 RMB, and after 4 months of use, 8 months are granted, which translates into an annual drug cost of 200,000 RMB.
(2) Loss of control
Although the efficacy of oseltinib is clear, we still saw 6% of patients in AURA3 who initially progressed and 29% who did not have significant tumor shrinkage. Even in first-line therapy in FLAURA, 1% of patients had uncontrolled disease at the outset, and 20% had no objective remission. The reason for this is unclear and needs to be further investigated.
(3) Drug resistance
Drug resistance is an inescapable topic for targeted therapy, and oxitinib has not been spared. It is important to biopsy again after drug resistance and perform genetic testing to clarify the cause of drug resistance.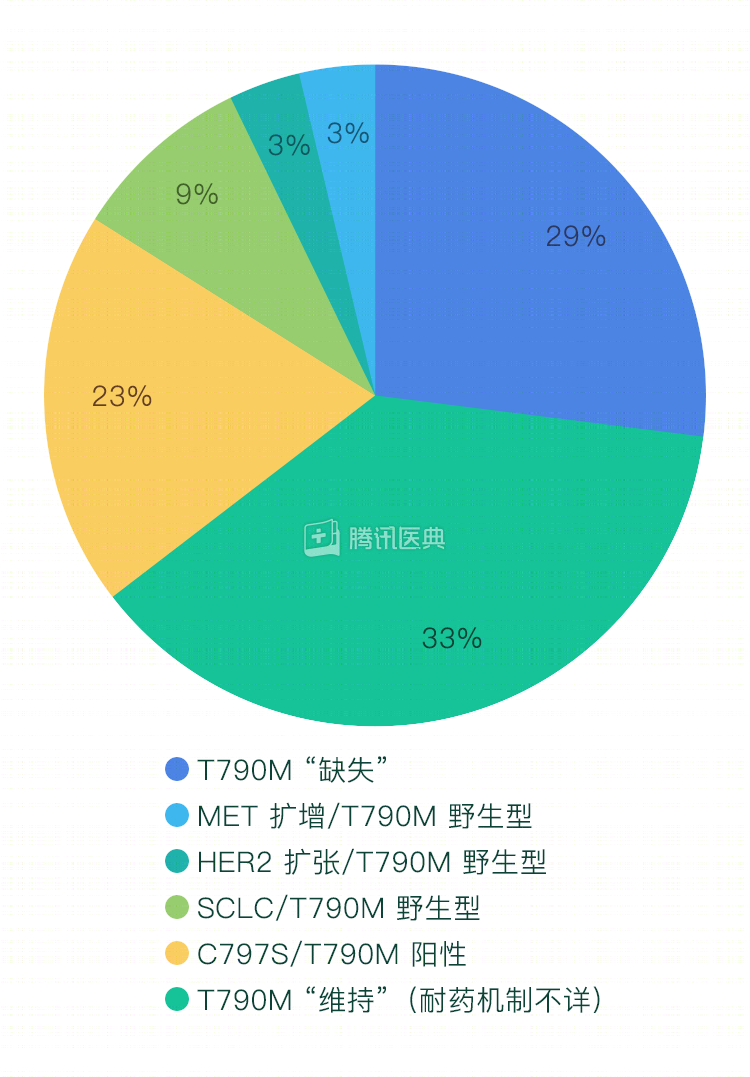
1) New mutations in EGFR
We are in the third round of the battle with EGFR mutant lung cancer: in the first round, the enemy released 19DEL/L858R and we took out gefitinib; in the second round, the enemy made T790M and we sent out oseltinib; in the third round, the enemy created C797S and wise scientists chose to combine gefitinib with oseltinib in some cases (trans mutations), but in cis In the case of cis mutations, fourth-generation drugs are needed, and drugs such as Brigatinib are in development, the efficacy of which remains to be seen.
(2) In addition, the EGFR pathway is blocked, the tumor cells may also activate other cellular pathways, or even transform into small cell lung cancer, which requires doctors and scientists to find new ways to target.
In summary, it is currently seen that oseltinib has good efficacy and safety for suitable patients, but the drug indications should be strictly grasped, and adverse reactions should be dealt with in a timely manner to ensure the safety of the drug.
Co-reviewed by: Dr. Qing Zhou, Chief Physician, Guangdong Provincial People’s Hospital, Guangdong Lung Cancer Research Institute Dr. Xiaoyan Bai, Dr. Yichen Zhang