Today, when it comes to immunotherapy for lung cancer, we are most familiar with a large class of drugs called “immune checkpoint inhibitors. The most notable of these are PD-1/PD-L1 inhibitors, but there is also an important group of drugs called CTLA-4 inhibitors.
What is a CTLA-4 inhibitor?
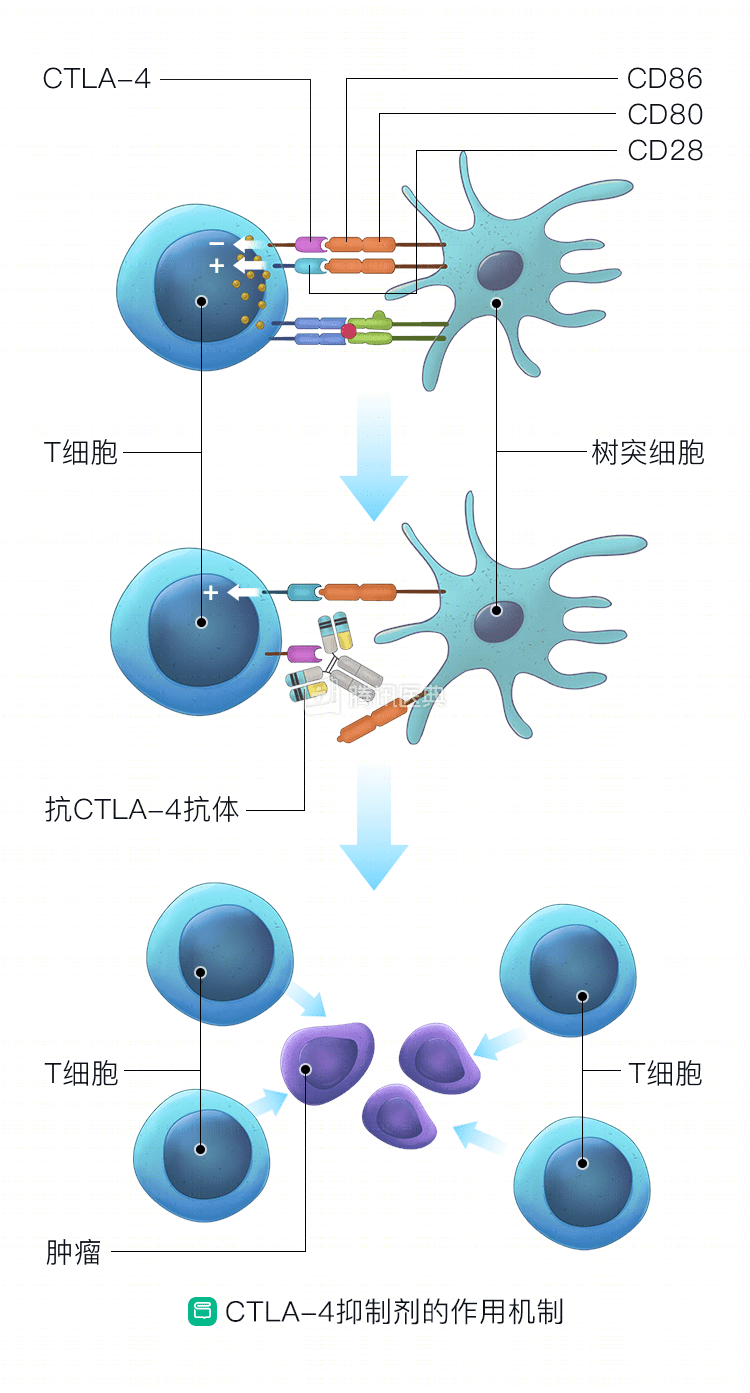
CTLA-4 (Cytotoxic T-Lymphocyte Associated Protein 4) is the Chinese name for “cytotoxic T-lymphocyte-associated protein 4,” and we certainly don’t need to remember this complicated name, just that it is distributed on the surface of our T When CTLA-4 is activated, instead of releasing “positive energy”, it inhibits the function of T cells and weakens their anti-tumor effect. To counteract this effect, we need to “fight” CTLA-4, so scientists have developed drugs such as “CTLA-4 inhibitors.
Currently, the main CTLA-4 inhibitor available in the US is Ipilimumab.
Can patients with lung cancer use CTLA-4 inhibitors?
Ipibizumab, which is available in the United States, is currently used primarily in melanoma and has not yet entered routine treatment for lung cancer, but scientists have begun clinical trials in lung cancer patients.
Non-small-cell lung cancer (NSCLC)
In a phase II study, 204 untreated patients with advanced NSCLC were divided into 3 groups, two of which had standard chemotherapy (paclitaxel + carboplatin) in combination with Ipilimumab.
The results showed that the sequential group had the best outcome, extending median overall survival by nearly 4 months compared with the chemotherapy-only group (table below).
| Control group | contemporaneous group | Sequence group | |
| Treatment protocol | Standard chemotherapy | Ipilimumab + chemotherapy for 4 cycles followed by placebo + chemotherapy for 2 cycles | Placebo + chemotherapy for 2 cycles, followed by Ipilimumab + chemotherapy for 4 cycles |
| Median Overall Survival (OS) | 8.3 months | 9.7 months | 12.2 months |
| Overall remission rate | 18% | 21% | 32% |
Another clinical trial, called CheckMate-012, also looked at the effects of Nivolumab (nabumab, a PD-1 inhibitor) in combination with Ipilimumab in patients with untreated advanced NSCLC. The results showed significant efficacy in patients with more than 50% of tumor cells expressing PD-L1, with up to 92% of patients having a tumor volume reduction of more than 30%.
| Nivolumab + Ipilimumab | Objective Remission Rate (ORR) | One-year OS rate |
| All Patients (Regardless of PD-L1 Expression) | 43% | 76% |
| PD-L1 expression is not less than 50% | 92% | 100% |
| PD-L1 expression is not less than 1% | 57% | 87% |
| PD-L1 expression >1% | 21% | 53% |
The internationally authoritative US NCCN guidelines do not currently recommend Ipilimumab for the treatment of NSCLC because the research evidence is not yet abundant.
Small cell lung cancer (SCLC)
SCLC is a major challenge in lung cancer treatment today, can these patients be treated with Ipilimumab? In recent years, a number of clinical trials have been conducted internationally.
In 2016, a study was published in a leading medical journal that showed that for SCLC patients who progressed after advanced chemotherapy, Nivolumab alone, or Nivolumab combined with Ipilimumab, significantly prolonged survival time.
| Single drug group | Dual-drug group | |
| Nivolumab | Nivolumab+Ipilimumab | |
| 14% | 26% | |
| ORR | 11% | 23% |
These numbers already exceed the efficacy of conventional chemotherapy. As a result, Nivolumab alone, or in combination with Ipilimumab, is the recommended regimen for second-line treatment of relapsed SCLC in the 2017 US NCCN guidelines. However, it is worth noting that the two-drug combination has greater side effects than single agents.
What are the side effects of CTLA-4 inhibitors?
There are toxic side effects with any therapy. Although CTLA-4 inhibitors have shown good efficacy in lung cancer studies, their serious toxic side effects cannot be ignored. Compared to PD-1 and PD-L1 inhibitors, CTLA-4 inhibitors may have more serious side effects, most commonly including pruritus, rash, enteritis, hepatitis, pneumonia, and endocrine disruption, especially the potential for severe colitis.
CTLA-4 inhibitors are currently less prominent than PD-L1 and PD-1 inhibitors in the treatment of lung cancer, and scientists are working to explore new combinations that they expect to get the most out of.
Related reading:
Co-Author: Dr. Xue-Tao Li, Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute