41. How often should I be retested after medication? What needs to be reviewed?
.
According to the drug insert, physicians should perform regular imaging exams in patients using PD-1/PD-L1 inhibitors until disease progression or treatment is discontinued. The frequency of review for the 4 PD-1/PD-L1 inhibitors approved by the FDA for NSCLC treatment is shown in the table below.
|
Drugs |
Review frequency |
|
Nivolumab |
Imaging was performed at 9 weeks after initial dosing; then every 6 weeks for 12 months; and after 12 months, it was repeated every 12 weeks. |
|
Pembrolizumab |
Re-check imaging every 9 or 12 weeks. |
|
Atezolizumab |
Imaging was repeated every 6 weeks for 36 weeks after initial dosing; and every 9 weeks thereafter. |
|
Durvalumab |
Reviewed every 8 weeks. |
.
42. Do I need to monitor PD-L1 expression/TMB during dosing?
.
PD-L1 expression is a common clinical predictor of efficacy, but studies have found that PD-L1 expression is spatiotemporally heterogeneous. In other words, PD-L1 expression may differ between surgical and biopsy specimens from NSCLC patients, PD-L1 expression differs between primary and metastatic tumor sites, and PD-L1 expression may change after other treatments (such as chemotherapy or radiation therapy), so dynamic monitoring of PD-L1 expression can help physicians understand the immediate disease status of patients and give more effective treatment.
TMB (tumor mutational load) is another marker used to predict the efficacy of PD-1/PD-L1 inhibitors. Studies have found no significant difference between TMB of blood (bTMB) and TMB of tissue. There is no clinical evidence at this time, and no relevant guidelines or recommendations, that dynamic monitoring of TMB can increase patient benefit.
43. After taking the drug, if the tumor is found to be enlarged, does it mean that the treatment is not effective and should be discontinued?
.
Chemotherapy and targeted therapies work directly on tumor cells, and if the tumor continues to grow after treatment, doctors will consider stopping the drug and choosing other treatments. But PD-1/PD-L1 inhibitors are unique in that they do not act directly on tumor cells, but rather attack them by “recruiting” (collecting tumor-specific lymphocytes) in the body. “In patients with solid tumors, PD-1/PD-L1 inhibitors usually work within 2 to 4 months, but they can also take up to 6 months or even a year to work (delayed remission). During the time before it takes effect, the tumor may grow, but after the PD-1/PD-L1 inhibitor takes effect, the tumor shrinks, a phenomenon also known as pseudoprogression.
In these cases, it is not appropriate to stop the drug hastily. So what are the circumstances of tumor enlargement that warrant discontinuation? The current recommendation for patients on PD-1/PD-L1 inhibitors is to have imaging every 6 to 12 weeks, and if the tumor enlargement is present at the first exam, it does not require discontinuation. However, if two consecutive exams are suggestive of tumor enlargement, the physician needs to evaluate this together with the total tumor load, and if the evaluation concludes that the treatment is not working, the drug should be discontinued.
44. How long do I have to take PD-1/PD-L1 inhibitors? Do they need to be taken for life?
.
The results of the Checkmate153 study suggest that patients who are effectively treated with PD-1/PD-L1 inhibitors are better off continuing the drug after 1 year than stopping it. But how long do you have to continue it after 1 year? The longest time used in foreign clinical trials so far has been the full 2 years. On the other hand, several studies suggest that even in patients who discontinue the drug, the disease continues to remit after discontinuation. Therefore, there is no definitive answer as to how long is appropriate, and it remains for scientists to answer through research.
45. Can PD-1/PD-L1 inhibitors be resistant? Why does resistance occur?
.
Resistance to PD-1/PD-L1 inhibitors has been observed previously in both melanoma and advanced kidney cancer patients treated with PD-1/PD-L1 inhibitors, as evidenced by tumor re-expansion after a period of stable disease control, and resistance as assessed by irRC (Immune-Related Response Evaluation Criteria) or iRECIST (Immunotherapy Efficacy Evaluation Criteria in Solid Tumors). Some patients develop resistance right after starting the drug, which we call primary drug resistance. There are also patients who have effective tumor control with the drug for a period of time and then develop resistance, which we call secondary resistance.
Resistance occurs because of the emergence of a new immune escape pathway, TIM-3, mutations in important genes (JAK2 and β2MG, etc.), defects in the tumor antigen delivery pathway, and dysregulation of immune metabolism. For example, the presence of TIM-3 is like a roadblock for PD-1/PD-L1 inhibitors to bind PD-1 or PD-L1, while mutations in JAK2 can turn the immune system “blind”. The JAK2 mutation makes the immune system “blind”, and even though the PD-1/PD-L1 inhibitor activates the lymphocytes, they can’t find the tumor cells to attack.
46. What happens when a PD-1/PD-L1 inhibitor fails (is resistant)?
.
Even if a PD-1/PD-L1 inhibitor is resistant, doctors are not helpless. Combining the NCCN Non-Small Cell Lung Cancer (NSCLC) Guidelines 7th Edition 2017 and the CSCO Primary Lung Cancer Guidelines 2018 Edition, the current treatment of NSCLC in China can be summarized in the table below. When PD-1/PD-L1 inhibitors fail, chemotherapy can still be used.
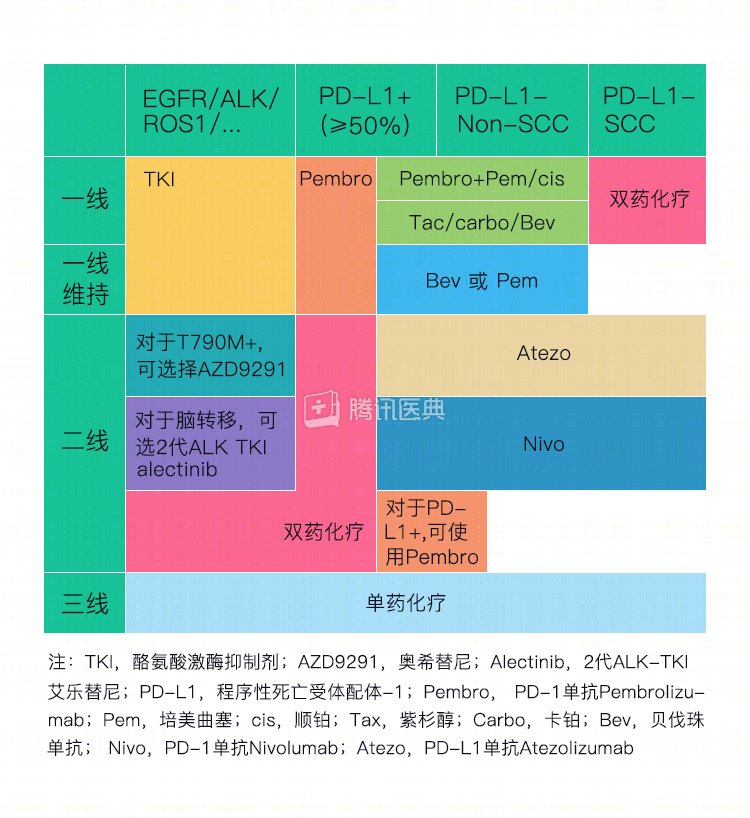
In addition to guideline-recommended chemotherapy regimens, switching to another immune checkpoint inhibitor is an option, and there are also exploratory studies that have found that PD-1/PD-L1 inhibitors combined with other immunotherapies (including CTLA-4 antibodies, LAG-3 antibodies, etc.), chemotherapy, and radiation therapy may resist resistance.
47. Is it true that I have heard that some patients remain effective when PD-1/PD-L1 inhibitors are continued after resistance or ineffectiveness?
.
In the OAK study, 56% (168/332) of patients with drug resistance had no disease progression and even some tumor shrinkage after continuing Atezolizumab. In addition, in the trials of PD-1/PD-L1 inhibitors for melanoma and kidney cancer (Keynote-006, Checkmate-067, Checkmate-025), the efficiency rate was 13% to 19% in patients who continued the drug after resistance.
The data from these studies seem to suggest that PD-1/PD-L1 inhibitors can be continued even after resistance has occurred. However, in fact, several of these studies do not distinguish between pseudoprogression and true disease progression in a clinical sense, and therefore have little reference value. Once resistance has occurred, it is still important to test promptly and follow the guideline recommendations to change the treatment regimen.
48. Are there any additional laboratory tests that need to be done before receiving immunotherapy?
.
According to the drug insert, routine blood, urine, stool, biochemistry, thyroid function, pituitary function, adrenocortical function, electrocardiogram, and chest X-ray should be checked before PD-1/PD-L1 inhibitor therapy to help the doctor understand the baseline situation without the drug. These indicators also need to be reviewed during treatment to monitor for adverse effects.
49. Can it be used in combination with surgery?
.
Neoadjuvant therapy refers to treatment with chemotherapy, radiation therapy, targeted therapy, and PD-1/PD-L1 inhibitors before surgery to reduce the size of the tumor to facilitate surgery afterwards.
For resectable NSCLC (stages I, II, and IIIA), recent studies have shown that Nivolumab is far more effective as neoadjuvant therapy than neoadjuvant chemotherapy and has less adverse effects. Currently, the Checkmate 816 study of Nivolumab in combination with Ipilimumab (another class of immune checkpoint inhibitor) as neoadjuvant therapy and the study of Atezolizumab as neoadjuvant therapy (NCT 02927301) are both ongoing. Once results are confirmed, the combination of PD-1/PD-L1 inhibitors and surgery is likely to be recommended by guidelines and enter clinical use.
50.
50. Can it be used in combination with chemotherapy?
.
For NSCLC without EGFR, ALK mutations, a recent study (Keynote-189) showed that Pembrolizumab in combination with chemotherapy (pemetrexed + platinum) in first-line therapy was almost 3 times more effective than standard chemotherapy in both PD-L1-negative and positive patients.
In another study (the IMpower-150 study), Atezolizumab combined with chemotherapy (paclitaxel + carboplatin) and bevacizumab (which is an angiogenesis inhibitor) as second-line treatment significantly prolonged progression-free survival in patients.
While not currently in clinical guidelines, the combination of PD-1/PD-L1 inhibitors with chemotherapy is likely to be recommended by guidelines and enter clinical use based on these results.
51. Can it be used in combination with targeted drugs?
.
Previous studies have shown that PD-1/PD-L1 inhibitors are only 3% to 7% effective in patients with NSCLC harboring EGFR or ALK mutations, far less effective than targeted therapy, and that there is a high incidence of immune-associated pneumonia when combining targeted therapy with PD-1/PD-L1 inhibitors (both the TATTON and CAURAL studies were terminated early for this reason). Therefore, the current evidence does not support the combination of PD-1/PD-L1 inhibitors with targeted therapy.
52. Can it be used in combination with other immunotherapy drugs?
.
Ipilimumab is a CTLA-4 (cytotoxic T-lymphocyte-associated antigen-4) inhibitor, which is part of the same family of immune checkpoint inhibitors as PD-1/PD-L1 inhibitors.
In 2015, the US FDA approved Nivolumab in combination with Ipilimumab for the treatment of patients with unresectable or metastatic melanoma with BRAF V600E wild type. Moreover, the combination therapy was much more effective than the two drugs alone. Recently, this combination therapy was also approved for the treatment of intermediate to high-risk advanced kidney cancer.
In the treatment of small cell lung cancer, Nivolumab in combination with Ipilimumab was recommended by the National Comprehensive Cancer Network (NCCN) guidelines for second-line treatment of recurrent small cell lung cancer.
In the treatment of NSCLC, the Checkmate 012 and Checkmate 227 studies confirmed that Nivolumab combined with Ipilimumab in first-line treatment of patients with high TMB (tumor mutational load) achieved excellent efficacy and significantly prolonged progression-free survival.
Taken together, these studies show that PD-1/PD-L1 inhibitors in combination with other immunotherapies can achieve excellent efficacy, but it is important to note that combination therapy also has more and heavier adverse effects than single agents. Practical application requires careful consideration by physicians.
.
53. Is it oral or intravenous? How exactly does it work?
.
According to the drug insert, the four PD-1/PD-L1 inhibitors currently approved by the FDA for NSCLC treatment (Nivolumab, Pembrolizumab, Atezolizumab, and Durvalumab) are all intravenous agents. Specific dosing, as well as regimen adjustments, will need to be based on physician opinion.
.
54. Are the doses for Chinese people the same as for foreigners? Is the efficacy the same?
.
Among the four PD-1/PD-L1 inhibitors that have been approved by the US FDA for NSCLC treatment, Nivolumab has been the first to obtain efficacy data in Chinese patients through the CHECKMATE078 study. The study confirmed that dosing and efficacy in Chinese were not significantly different from those in foreigners.
Studies recruiting Chinese lung cancer patients with Pembrolizumab, Atezolizumab, and Durvalumab are ongoing, and there is no evidence to confirm that these 3 drugs are still available in the same doses in Chinese patients.
55. Can it be used in older adults?
.
The drug insert does not state that it should not be used in older patients, although some studies have found that people over 65 years of age are more likely to have accelerated tumor progression. Therefore, for this group of patients, the drug should be used with caution.
56. What drugs should not be used during treatment with this class of drugs?
.
There are no formal interaction studies of the four approved PD-1/PD-L1 inhibitors with other drugs, and given that all four lack circulatory action factors, the academic community presumes that they have minimal pharmacokinetic effects on other drugs.
According to the drug insert, glucocorticoids and other immunosuppressants should be avoided before starting PD-1/PD-L1 inhibitors to prevent interference with the drug activity of PD-1/PD-L1 inhibitors.
In addition, antibiotics may have an impact on the efficacy of PD-1/PD-L1 inhibitors and should be used with caution in patients receiving PD-1/PD-L1 inhibitor therapy. If you are taking, or planning to take, antibiotics, be sure to inform your doctor first and use them under his or her supervision. (See question #57 for more details.)
57. Do antibiotics affect drug efficacy and safety?
In patients with lung, kidney, and bladder cancers, it was observed that the efficacy of PD-1/PD-L1 inhibitors decreased by nearly 1.5 if antibiotics (amides, quinolones, and macrolides) were administered 2 months before or during the use of PD-1/PD-L1 inhibitors. However, in animal studies of pancreatic and intestinal cancers, antibiotics were observed to make PD-1/PD-L1 inhibitors more effective.
The main reason for either reduced or improved efficacy is presumably that antibiotics affect intestinal flora, which in turn affects the immune system. Therefore, antibiotics should be used with caution in patients treated with PD-1/PD-L1 inhibitors. If you are taking, or are planning to take, antibiotics, be sure to inform your doctor first and use them under his or her supervision.
58. Can I take Chinese medicine at the same time during treatment?
.
The efficacy of PD-1/PD-L1 inhibitors relies on the body’s normal immune system. Chinese medicine is a mixture of substances that are likely to affect the body’s immune system and influence the efficacy of PD-1/PD-L1 inhibitors. Therefore, Chinese medicine is not recommended during treatment.
.
59. Do I need to pay attention to anything in my daily life during treatment with these drugs?
.
Considering that common adverse effects of PD-1/PD-L1 inhibitor therapy include malaise, rash, diarrhea, or constipation, patients should take rest during treatment. It is also important to avoid infections as much as possible to prevent the use of antibiotics and other drugs from affecting the efficacy of PD-1/PD-L1 inhibitors.
Serious adverse reactions to this class of drugs can be fatal, despite their low incidence. Therefore, patients should inform their doctors of any discomfort during treatment.
Related reading:
Co-reviewed by: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Xue-Tao Li, Associate Chief Physician Dr. Si-Yang Liu