Small cell lung cancer (small cell lung cancer, SCLC) is one of the common pathological types of lung cancer, accounting for about 15% of lung cancers. It is characterized by short multiplication time (the time required for the tumor to double in size) and susceptibility to metastasis. Surgery, radiotherapy and chemotherapy each play an important role in the treatment of SCLC at different stages. They can both cooperate with each other and fight independently.
What is limited-stage SCLC?
Before doctors can make treatment decisions, it is important to first define the clinical stage of SCLC. Clinical staging helps physicians more accurately assess patient prognosis and guide treatment. According to the National Comprehensive Cancer Network (NCCN), SCLC can be classified as limited-stage or extensive-stage.
Limited stage means that the tumor is amenable to radical radiation therapy. This generally refers to relatively early stage patients, often stages I-III of TNM staging (any T, any N, M0, i.e., no distant metastases); however, patients in T3-4 who are unable to tolerate radical radiotherapy because of multiple nodules in the lung or tumor size need to be excluded.
Extensive stage refers to patients with tumors that are not amenable to radical radiotherapy, i.e., stage IV (any T, any N, M1a/b, i.e., distant metastases) in TNM staging, and patients with tumors that are too large to tolerate radical radiotherapy.
Treatment options for limited-stage SCLC: two cases
Here are two cases that show how doctors choose treatment options for limited-stage SCLC.
Case 1: Surgical treatment + postoperative concurrent chemoradiotherapy
Mr. Zhang had a cough and blood cough for almost 1 month, and a chest CT revealed a mass in the left upper lung. He was initially diagnosed with lung cancer cT2aN0M0 stage IB (limited stage) by PET-CT at a lung cancer specialist.
Our guidelines recommend that surgical resection be considered for SCLC staged T1-2N0M0 after complete workup.
Mr. Zhang underwent radical surgical resection as recommended by his doctor. Intraoperatively, tumor and lymph node specimens were taken for pathological analysis, indicating metastases in the hilar and mediastinal lymph nodes. The pathological diagnosis is the “gold standard” when the pathological stage is inconsistent with the clinical judgment before surgery, so the doctor revised the stage to SCLC, pT3N2M0 stage IIIB.
Our guidelines recommend that patients with pathologic staging suggestive of hilar (N1) and ipsilateral mediastinal lymph node (N2) metastases after SCLC surgery require postoperative radiotherapy + chemotherapy (sequential or synchronized radiotherapy) to reduce tumor recurrence.
So, Mr. Zhang received postoperative synchronized radiotherapy.
Radiotherapy was administered using intensity modulated radiation therapy (IMRT) at 50 Gy (Gy is the unit of radiation dose) / 25F (total dose of 50 Gy in 25 fractions) to the metastatic lymph node area.
Synchronous chemotherapy regimen: cisplatin 80 mg/md1 (80 mg per m2 of body surface area on day 1) + etoposide 100 mg / m d1,2,3 (100 mg per m2 of body surface area on days 1, 2, and 3).
Mr. Zhang’s course of radiotherapy went well with no significant side effects. After treatment, he is now being reviewed regularly on an outpatient basis, and no signs of tumor recurrence have been seen.
Case 2: Synchronized chemoradiotherapy
A 60-year-old grandfather came to the hospital with facial swelling. The doctor considered superior vena cava syndrome caused by tumor compression and recommended whole-body PET-CT.
PET-CT scan revealed a right upper lung mass with multiple mediastinal lymph node enlargement, which was considered a lymph node metastasis. The pathological diagnosis of SCLC was made by biopsy of the mass through fiberoptic bronchoscopy. cT4N2M0, stage IIIB, was the clinical stage.
The supervising physician convened a multidisciplinary team (MDT), which concluded that surgery was not recommended for SCLC with mediastinal lymph node metastases, and that the radiotherapist determined that the tumor could be treated with concurrent radiotherapy, and that the concurrent chemotherapy regimen was etoposide combined with platinum, as recommended by our guidelines.
Finally, the MDT recommended 4 weeks of etoposide + cisplatin chemotherapy with the addition of thoracic radiotherapy during chemotherapy, with the earlier the start of radiotherapy the better.
Lee followed his doctor’s advice and first received the first cycle of cisplatin 80 mg/m2 d1 + etoposide 100 mg/m2 d1,2,3 chemotherapy, along with radiotherapy preparation (CT simulation, target setting, planning, etc.); radiotherapy was started at the same time as the second cycle of chemotherapy (IMRT 60 Gy /30F, irradiated area including the primary lesion in the lung and metastatic lymph nodes); radiotherapy was started at the same time. The radiotherapy was started at the beginning of the second cycle of chemotherapy (IMRT 60 Gy / 30F, including the primary lung lesions and metastatic lymph nodes); chemotherapy continued after radiotherapy until the end of 4 cycles of chemotherapy.
The entire process went well, and after radiotherapy, he was reviewed regularly at the clinic, and the best outcome assessment was partial response (PR, 60% tumor shrinkage), and there are no signs of tumor recurrence.
Summary: Physicians’ thoughts on the management of limited-stage SCLC
.
After reading the above two case studies, do you have a general understanding of the treatment of limited-stage SCLC?
The treatment of limited-stage SCLC is a very important part of the treatment of SCLC, but it is important to note that in addition to guideline recommendations, physicians need to develop individualized treatment plans for each patient.
In addition to the indications for treatment, physicians need to be aware of the patient’s general condition, such as age, performance status (PS) scores, lung function, previous treatment, and any co-morbidities, which can affect the success of treatment. Only a detailed understanding of the disease and a combination of guideline recommendations and individual circumstances will allow the right treatment (concurrent radiotherapy, sequential radiotherapy, surgery, radiotherapy alone) to be used.
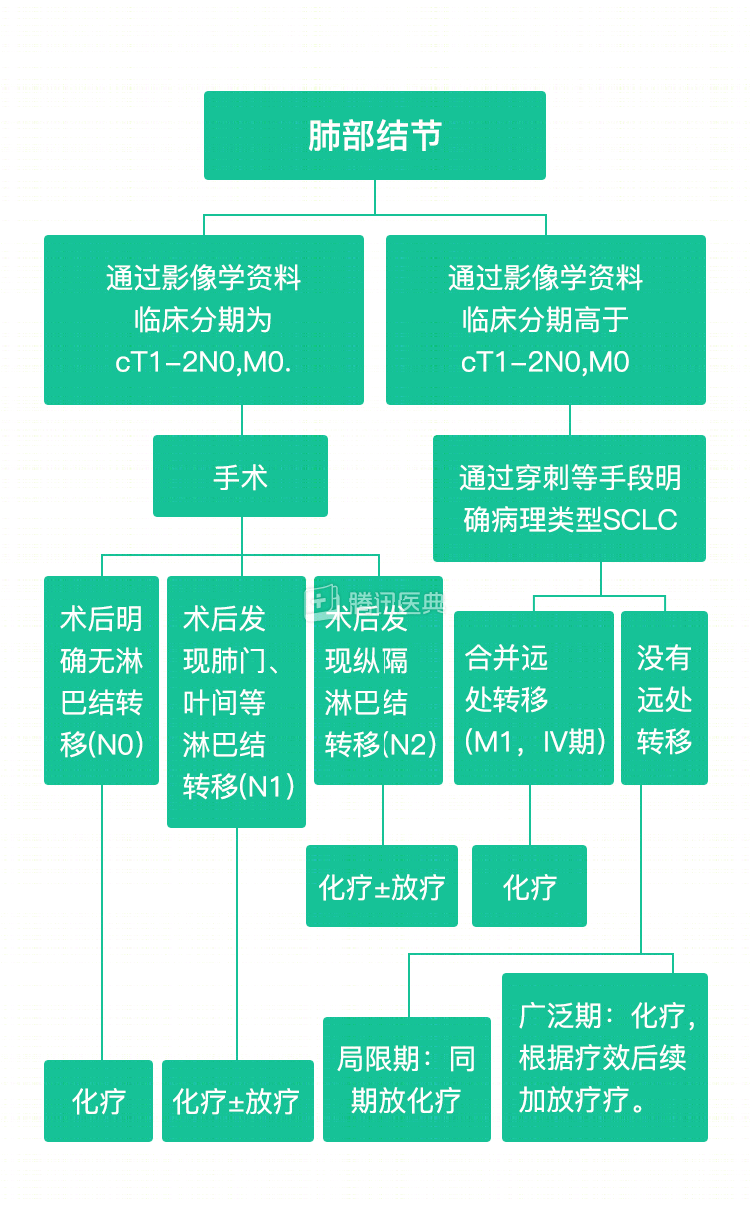
The chart below summarizes the treatment strategies for different stages of SCLC.
Disclaimer:
Tumor disease and treatment options are extremely complex, and treatment should be fully individualized, and this case does not represent a treatment decision for a “similar patient. Please seek professional advice from your supervising physician regarding your specific treatment plan.
Co-authors Dr. Peixin Tan Dr. Hao Sun, Guangdong Provincial People’s Hospital, Guangdong Lung Cancer Institute