Superior vena cava obstruction, also known as superior vena cava syndrome (SVCS), is a dangerous sign of an acute episode of obstruction or narrowing of the superior vena cava due to various causes, resulting in impaired blood return to the superior vena cava system. The main manifestations are obstruction of venous return, bruising, edema, and formation of collateral circulation in the head, face, neck, upper extremities, and chest, with the potential for further progression leading to hypoxia and increased intracranial pressure.
When this is encountered, the physician will treat it quickly to relieve the symptoms.
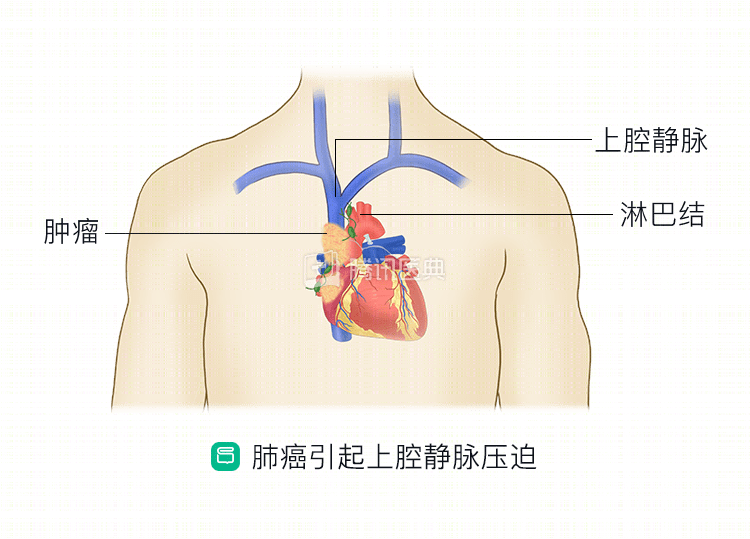
Why does lung cancer cause SCVS?
The superior vena cava is located in the right front of the upper mediastinum, between the ascending aorta and the right main bronchus, and receives blood primarily from the veins of the head and neck, upper extremities, and upper chest, returning to the right atrium.
The superior vena cava has a thin wall, low intraluminal pressure, is surrounded by groups of hilar and paratracheal lymph nodes, the aorta, pulmonary artery, trachea, and sternum, and is mostly encapsulated in the pericardial reflex with a small range of motion. Therefore, once there is a surrounding mass, such as lung cancer with enlarged mediastinal lymph nodes, it can easily invade or compress the superior vena cava and cause SVC.
How do doctors diagnose SVCS?
The severity and briskness of SVCS symptoms are related to the site and degree of venous return obstruction, with SVCS caused by malignant tumors such as lung cancer mostly being a chronic process.
For patients with lung cancer, the initial diagnosis can be made if symptoms such as dyspnea, cough, chest pain, facial and neck swelling or periorbital edema, conjunctival congestion, arm swelling, difficulty swallowing (caused by pharyngeal edema), headache and dizziness (caused by cerebral edema), blurred vision, and impaired consciousness are present, and the physician examines the patient and finds angry jugular veins, dilated chest wall veins, congested head and facial edema, and bilateral upper limb edema.
At this point, the physician may perform the necessary imaging tests to confirm the diagnosis, such as a chest radiograph, chest CT, or MRI. Chest radiographs are the preferred test because they are the most convenient, but the latter two are more accurate in diagnosis and can provide localization support for subsequent treatment, in addition to showing the relationship between the tumor and blood vessels.
Of course, lung cancer is not the only possible cause of SCVS; some benign lesions such as hilar lymphatic tuberculosis, benign mediastinal tumors, intrathoracic goiter, and chronic mediastinal inflammation are also possible.
What happens when SVCS occurs?
Once SVCS occurs, doctors will treat it as soon as possible, first symptomatically to relieve symptoms, and then later to treat the primary cause.
If you develop symptoms of SVCS, you will generally need bed rest, elevation of the head and neck, oxygen, and strict restriction of sodium intake. Your doctor may use diuretics and glucocorticoids to reduce water and sodium retention and relieve edema, and will take care to avoid causing blood clots. If you experience significant chest pain and irritability, inform your doctor promptly and he or she may give you some pain medication and sedatives.
In the acute phase, treatment for lung cancer may include radiation therapy, chemotherapy, or targeted therapy if there is a sensitive gene mutation.
Radiotherapy is one of the main therapies, which targets the enlarged mediastinal and paratracheal lymph nodes that cause venous compression. If the extent of the lesion can be completely wrapped into the irradiation field, the physician will consider using radical doses and target areas, including the mediastinum, hilum, and adjacent parenchymal lung lesions. If the lung cancer occurs in the upper lobes of both lungs, sometimes the supraclavicular lymph nodes are also covered. Radiation therapy is effective and quick, with varying degrees of remission usually occurring after 3 to 4 irradiations. If there is no improvement after a week of irradiation, the doctor may target venous thrombosis for exclusion and treatment.
Chemotherapy is also an optional strategy, or a combination of radiotherapy and chemotherapy. When using chemotherapy or other intravenous medications, physicians typically select lower extremity veins to avoid exacerbating symptoms.
If conservative medical treatment fails to achieve a satisfactory outcome, physicians will also consider surgical treatment, such as superior vena cava stenting.
Overall, SVCS starts rapidly and progresses rapidly, and doctors take effective measures to relieve symptoms while treating lung cancer aggressively.
Co-reviewed by: Dr. Zhou Qing, Chief Physician, Guangdong Provincial People’s Hospital, Guangdong Lung Cancer Institute Dr. Bai Xiaoyan Gao Xin