- Immune checkpoint inhibitors: This is the most prominent class of immunotherapy drugs available. If you compare our immune system to a car, using an immune checkpoint inhibitor is like releasing the brakes and letting the car go full speed.
- Monoclonal antibodies: Once the antigen is found, it acts as a tugboat to “tow” the cancer cells to the immune cells to destroy them, and it also blocks the signaling of the cancer cells to inhibit their growth and reduce the size of the tumor.
.
.
Cancer vaccines and secondary cellular immunotherapy
Doctors take a portion of the tumor tissue from the patient, isolate the tumor antigens, “modify” it, and then infuse it back into the patient to help the patient’s immune system recognize the tumor cells and attack them.
- Continuous cellular immunotherapy: Still in clinical trials, they are effective against leukemia and some types of melanoma.
- Immunotherapy: The newest therapy for metastatic non-small cell lung cancer (NSCLC), it uses the body’s immune system to kill cancer cells and inhibit their growth.
Immune drugs
Our immune system, which recognizes “unfamiliar” substances like viruses and bacteria, protects the body from attack, and cancer cells often “escape” this defense because they look so much like normal cells.
Some cancer cells can even “shut down” parts of the immune system so that they can reproduce unrestricted, and immune drugs can help “shine the light” on the immune system, allowing it to “see” and “see”. The immune drugs can help “shine” the “eyes” of the immune system so that it can “see” and kill the cancer cells.
There are several immune drugs that have been approved for clinical use in the United States, and the rest are still in clinical trials, and scientists are continuing to research and develop these new drugs.
What kinds of immunotherapy are included?
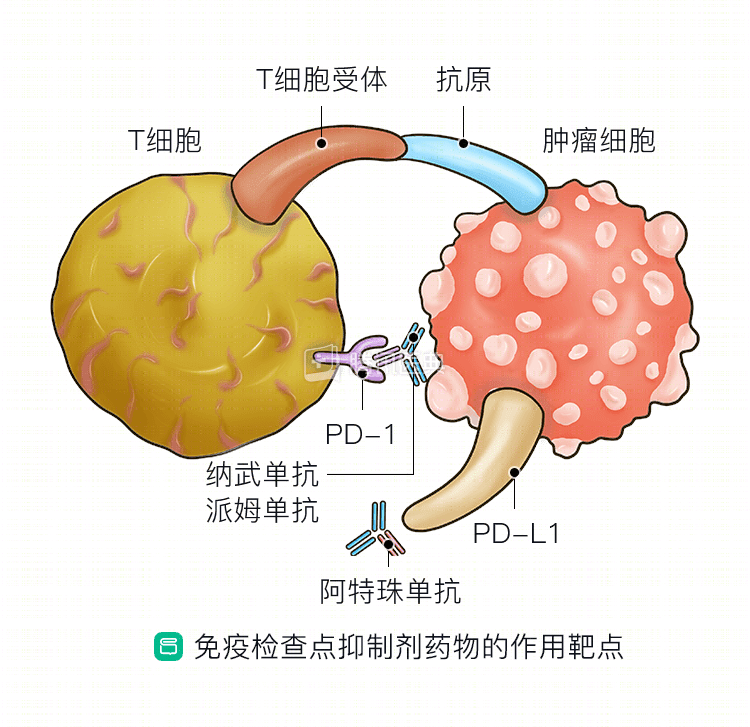
Immune checkpoint inhibitors
“Immune checkpoints” are molecules that attach to the outside of immune cells and regulate the strength of the immune response. The cancer cells use this to “activate” immune checkpoint molecules to protect themselves from being cleared by the immune system.
If you compare the immune system to a car, using an immunotherapy drug is like releasing the brakes and letting the car go at full speed, the immunotherapy drug stops the immune checkpoint molecules from working and lets the immune system work.
They “tell” the immune system to go all out against the cancer cells, and they also stop the cancer cells from shutting down the immune system.
4 immune checkpoint inhibitor drugs
Currently, the FDA approves 4 immune checkpoint inhibitor drugs for the treatment of non-small cell lung cancer, administered intravenously every 2 to 3 weeks: atezolizumab, nabolutumab, pablizumab, and devaluzumab.
Among them, nabumab was approved by the FDA in September 2018 for the treatment of patients with metastatic small cell lung cancer (SCLC) who are not responding to platinum-based chemotherapy and at least one other treatment.
However, serious side effects can occur when the immune system is working at full capacity with the drug, and the immune system may attack the lungs, intestines, liver, secretory glands, kidneys, or other organs.
If this happens, the doctor will take the patient off the immune checkpoint inhibitor and switch to a corticosteroid to give the immune system a proper “rest.
Monoclonal antibodies
The FDA has also approved several immune checkpoint inhibitor drugs that can be used to treat other cancers, and scientists are now conducting clinical trials to see if they can also treat non-small cell lung cancer.
There are also studies that are looking at the efficacy of the combination, including avelumab, eprilimumab (also called epirimab).
Monoclonal antibodies
Scientists have grown this molecule in the lab and can look for specific markers (antigens) outside of cancer cells to trace the cancer cells.
Once the antigen is found, the monoclonal antibody acts as a tugboat to “drag” the cancer cells to the immune cells to destroy them, and the monoclonal antibody can also block cancer cell signaling and inhibit their growth, thereby reducing the size of the tumor.
Bevacizumab and ramolutumab
The following 2 monoclonal antibodies have been approved by the FDA: bevacizumab and ramolutumab.
Cancer vaccines
Preventive vaccines, which give the body early immunity, are now being used by doctors to treat cancer cells that are already in the body; these are called therapeutic vaccines.
This is how doctors might use a therapeutic vaccine: They take a portion of the tumor tissue from the patient, isolate the tumor antigen, “modify” it, and then infuse it back into the patient to help the patient’s immune system recognize the tumor cells and attack them.
The FDA has not approved any cancer vaccines for non-small cell lung cancer, and those in the research phase include DRibbles, GV1001, Tergenpumatucel-L, TG4010, and others.
Persistent cellular immunotherapy
These types of cancer immunotherapies are still in clinical trials, and they are effective against leukemia and some types of melanoma.
Doctors take immune T cells from patients, proliferate them in the lab, and then infuse the cultured T cells back into the patient to boost the body’s defenses against cancer.
In other types of pericyte immunotherapy, doctors take normal T cells, add a mixture of antibodies and T-cell receptors, and then infuse them back into the patient, which can precisely target and kill cancer cells.
Is immunotherapy right for me?
If you have advanced NSCLC with high PD-L1 expression or high TMB, your doctor may recommend immunotherapy, possibly right off the bat.
Related reading:
Co-reviewed by Dr. Yue-Li Sun, Guangdong Provincial People’s Hospital Dr. Lun-Xi Peng, Guangdong Lung Cancer Institute.