Brain metastases are a common hurdle for almost all patients with advanced lung cancer. Studies have shown that 3 to 5 out of 10 patients with non-small cell lung cancer will develop brain metastases, and the proportion is higher in adenocarcinoma patients; about 15% of small cell lung cancer patients have brain metastases at the time of diagnosis, and cumulatively more than half will develop them within 2 years of diagnosis.
What is the current clinical treatment for this “hurdle”?
What is the current clinical treatment for this “hurdle”?
Recommendations according to current authoritative guidelines:
- For ≤3 brain metastases, “stereotactic radiotherapy” with fewer side effects is preferred;
- For >3 brain metastases, “stereotactic radiotherapy” with fewer side effects is preferred.
- With >3 brain metastases, the only option is usually whole brain radiotherapy. However, the side effects are significant, damaging normal brain tissue, affecting brain function, and with very limited life extension.
You may be wondering, with so many side effects from radiation therapy, can it be treated with medications?
It is important to understand that there is a “barrier” between our blood and our brain, called the “blood-brain barrier,” which normally prevents some harmful substances in the blood from entering the brain, but also blocks most anti-cancer drugs, making the brain a “safe place” for cancer cells. The brain is a “sanctuary” for cancer cells.
So, is there really no cure for brain metastases?
There are new targeted drugs and immunotherapies that have the “superpower” to cross the blood-brain barrier, giving cancer cells nowhere to hide.
There are different options for new drugs for different patients.
Mutation “targets”: new targeted drugs
EGFR and ALK, known medically as “epidermal growth factor receptor” and “mesenchymal lymphoma kinase,” are the two “targets” in lung cancer that we know best. “These are the two best understood targets in lung cancer. The most important thing is that the patient can choose the right target drug under the guidance of the doctor.
There are now three generations of both types of targeted drugs, each with a different ability to deal with brain metastases.
EGFR-targeted drugs
First- and second-generation EGFR-targeted drugs, which do not effectively penetrate the blood-brain barrier, have limited ability to fight intracranial cancer. However, third-generation oxitinib and AZD3759, which is currently in clinical trials, can penetrate the blood-brain barrier more efficiently and have good efficacy against brain metastases.
For patients with brain metastases, ositinib was significantly more effective than chemotherapy (below), with a median progression-free survival of 15.2 months for patients; AZD3759 resulted in shrinkage of brain metastases in 52% of patients, with 28% shrinking by more than 30%.
Treatment efficiency:
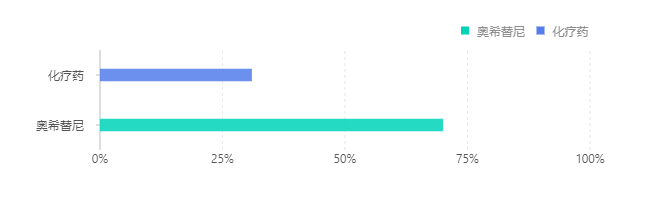
Time to intracranial remission (months)

ALK-targeted drugs
The first-generation crizotinib has limitations in the treatment of advanced lung cancer, and the second and third-generation drugs are more effective in intracranial lesions, as shown in the following table:
| Level | Drug name | Efficacy |
| Second generation | Aletinib | Reduces the risk of brain metastases by 84% and the risk of disease progression or death by more than 50%, resulting in a progression-free survival of 27.7 months for patients with brain metastases |
| Ceretinib | Produces 45% overall intracranial remission rate and prolongs median progression-free survival to 9.2 months in patients with brain metastases | |
| Bugatinib | Prolongs median progression-free survival to 12.9 months | |
| Third generation | Lauratinib | Able to inhibit a broader range of ALK targets, it can save many patients who have failed other treatment regimens: for patients who have failed crizotinib, crizotinib + chemotherapy, two or three ALK-targeted agents, the intracranial efficiency of loratinib is as high as 100%, 55.6%, 41.2% and 57.1% |
Overall, aletinib has better efficacy than brugitinib and ceritinib, and lauratinib is mainly indicated for patients after drug resistance.
No mutation “target”: choose anti-angiogenic drugs or immunotherapy
Anti-angiogenic agents
“Anti-angiogenic therapy” degrades tumor blood vessels and inhibits neovascularization, depriving cancer cells of blood nutrients and “starving the tumor”.
The combination of chemotherapy with anti-angiogenic drugs such as bevacizumab resulted in a twofold increase in median progression-free survival (from 4.5 months to 9 months) and similar intracranial remission rates to extracranial ones, which seems to break the “spell” of the brain as a tumor sanctuary. However, this needs to be supported by more research evidence.
Immunotherapy drugs
New immunotherapeutic agents such as nabolutumab (commonly known as “O”), pablizumab (commonly known as “K”), and Atezolizumab also offer treatment options for patients with brain metastases, with efficacy shown below:
| Drug name |
Efficacy |
| Navulizumab | Patients with less progression of brain metastases with nabumetumab treatment compared to chemotherapy |
| Pabrolizumab | 40% remission rate in patients with PD-L1 expression>1% brain metastases |
| Atezolizumab | Reduces the risk of disease progression by 39% and the risk of death by 45% in patients with brain metastases |
It can be argued that for patients with brain metastases, all 3 of these drugs are applicable. However, the problem facing this class of drugs is that it is difficult for physicians to identify patients suitable for treatment. And in patients who are not screened, these drugs are less than 30% effective, and even less effective in patients with brain metastases.
In conclusion, for patients with brain metastases that have a mutated “target,” targeted therapy is effective, extending survival by 11 to 24 months, and for patients without a mutated “target,” anti-angiogenic drugs and immunotherapy offer some new options. The new options are