Pathology is the irreplaceable “gold standard” for the diagnosis of lung cancer, and doctors usually do not base their treatment plans on a “clinical diagnosis” alone.
In conventional pathology, a pathologist takes a tissue specimen through a series of “processes” to make a glass slide, stains it, and then looks at the morphologic features of the tissue cells under a microscope to make a judgment. However, this qualitative morphological method can only make a rough judgment and in many cases cannot determine the origin of the cancer. Doctors sometimes need to adopt more and more in-depth tests, such as immunohistochemistry, image analysis techniques, and molecular pathology. We provide a brief overview.
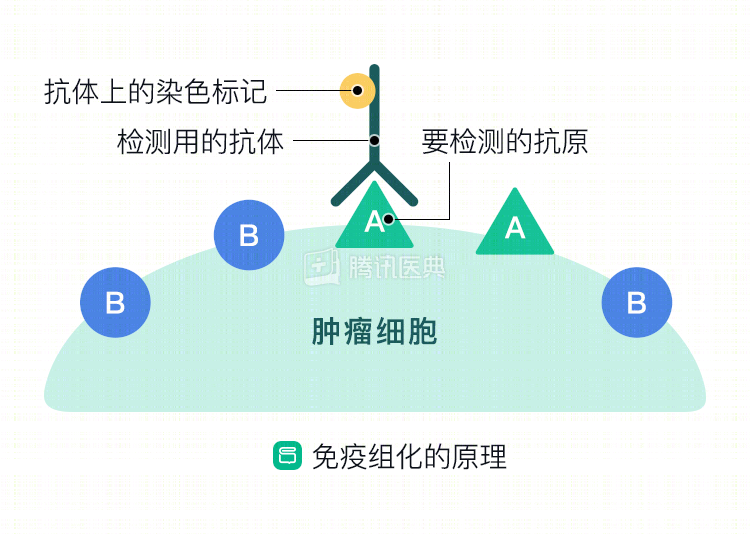
Immunohistochemistry (immunohistochemistry)
It uses the basic principle of immunology – antigen-antibody specific binding (like a key to a lock) – to detect a protein (“antigen”) expressed by a tumor cell using a specific antibody as a “bait”.
The basic principle of antigen-antibody specific binding (like a key with a lock) is to use a specific antibody as a “bait” to detect a protein (“antigen”) expressed by the tumor cells, and then use that protein as a clue to determine the tissue origin of the cells.
The process is to extract a chemical from the tissue or cell as an “antigen” or “semi-antigen” and immunize the animal (e.g., rabbit, sheep, etc.) to obtain specific “antibodies “The antibodies are then used to detect similar antigenic substances in tumor tissues or cells. The antigen-antibody complex is colorless and must be displayed with the help of a special “dye”.
In the case of lung cancer, cancer cells of different origins secrete different specific proteins. For example, TTF-1, Napsin A, and CK7 are common immunomarkers for lung adenocarcinoma, while p63 and ΔN p63 (p40), CK5/6, and CK34βE12 are common immunomarkers for squamous lung cancer.
Clinically, a combination of different immunomarkers is generally required to identify lung adenocarcinoma and lung squamous carcinoma. According to the 2018 CSCO lung cancer guidelines, in advanced biopsy cases, two immunohistochemical markers, TTF-1 and P40, are used to identify adenocarcinoma or squamous carcinoma when possible. For example, the TTF-1/p40 combination is usually “one negative, one positive” in both adenocarcinoma and squamous carcinoma. TTF-1 positivity has a strong predictive value for lung adenocarcinoma; diffuse, strong positive p40 expression tends to diagnose squamous lung carcinoma.
Molecular pathology
This is an emerging subdiscipline of pathology, which studies disease at the genetic level, using molecular biology techniques. Specialists extract and amplify genetic information in samples such as tumor tissue, pleural fluid, or blood, and use molecular biology techniques to detect the genetic information of DNA molecules in cells and analyze their status at the level of biomolecules such as proteins and nucleic acids to help in the diagnosis and treatment of tumors.
Targeted therapies, which are now widely used in lung cancer, are based on the detection of the “driver genes” of lung cancer.
Targeted therapies in lung cancer are based on testing for the presence of a driver gene, and the choice of small molecule drugs or monoclonal antibodies is based on the presence of the driver gene.
Related reading
Co-reviewed by: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Tu Haiyan, Associate Chief Physician Dr. Sun Yueli Dr. Li Xiangmeng