I. PD-1/PD-L1 inhibitors
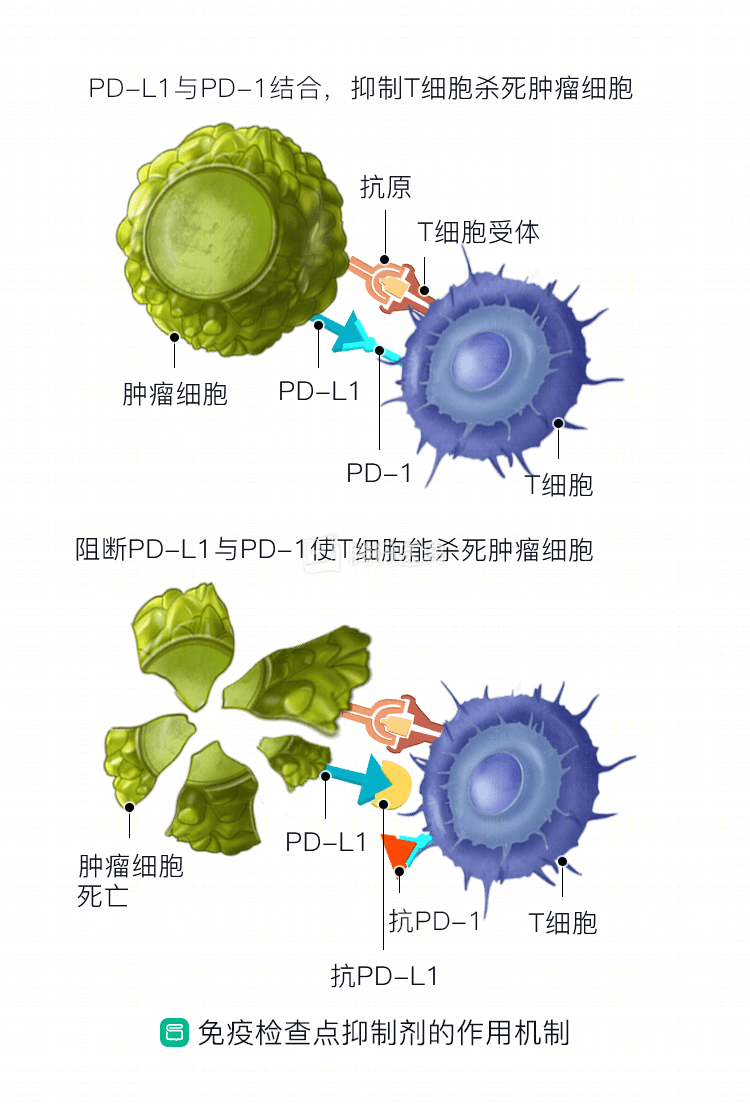
PD-1 is located on the surface of lymphocytes and acts as a “brake” for the immune system, scientifically known as an “immune checkpoint”. Tumor cells can express PD-L1, the “ligand” for PD-1, which binds to PD-1 and inhibits the lymphocytes from being “hunted” by the immune system. Therefore, if there is an antibody that can inhibit PD-1 or PD-L1, it can restore lymphocyte activity and allow the immune system to effectively attack the tumor. This is how PD-1/PD-L1 inhibitors came to be.
In 1992, Japanese scholars first discovered PD-1, naming it programmed death receptor 1 (Program death-1, PD-1).
In 2003, Professor Chen Ping of Yale University was the first to introduce PD-L1 antibodies to tumor therapy, finding that blocking PD-L1 cured 60% of tumor-bearing mice.
The first PD-1 antibody, nivolumab, began clinical studies in 2006 and showed results in early 2012. phase I studies showed that patients with advanced non-small cell lung cancer (NSCLC) who had received multiple treatments still had a remission rate of about 17% with Nivolumab.
In 2015, Nivolumab was approved by the US FDA as the first immune checkpoint inhibitor for advanced NSCLC, ushering in a new era of immunotherapy for lung cancer. On June 15, 2018, nabumab was launched in China for the treatment of lung cancer.
The other drugs in this class approved by the FDA for lung cancer are pembrolizumab, atezolizumab, and durvalumab.
II. CTLA-4 inhibitors
Similar to PD-1, the CTLA-4 receptor on the surface of lymphocytes inhibits lymphocyte activation when it binds to its ligand. Thus, antibodies against CTLA-4 restore the ability of lymphocytes to recognize and attack tumors.
CTLA-4 was discovered in 1987, and in 1996, studies confirmed that anti-CTLA-4 antibodies could prompt the immune system to kill tumors. in 2001, the first CTLA-4 antibody, Ipilimumab, was also studied in advanced prostate cancer and melanoma.
Multiple studies of Ipilimumab for advanced lung cancer are currently underway in this country and abroad, including in combination with Nivolumab and conventional chemotherapy. They are clinically proven to extend survival time for patients with advanced lung cancer and have fewer side effects than chemotherapy.
In addition to this, drugs targeting other immune checkpoint molecules are also being investigated.
What is immunotherapy? Why can it treat lung cancer?
The immune system is a key barrier that protects us from outside diseases. It recognizes tumor cells in most cases and kills them in their cradle. However, a few tumor cells have the ability to escape from immune surveillance, which is called immune escape, and even allows immune cells to promote “their own” growth in turn. Immunotherapy, which has become very popular in recent years, can “shine a light” on the immune system, allowing it to re-identify tumor cells, or fight them by boosting the immune response. This is considered to be an important treatment after surgery, radiation, chemotherapy, and targeted therapies that have a clear effect on tumors, and was listed in Science magazine as one of the top 10 discoveries in the world of science in 2013.
The only immunotherapies that have been shown to be effective in lung cancer are immune detection site inhibitors. Other approaches, such as CAR-T, are still in the research phase and their clinical use is uncertain.
Related reading:
Co-reviewed by: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Institute Dr. Kai Yin