Lung cancer that has progressed again after treatment is a hurdle for many patients to overcome. Treatment after progression is also complex, and treatment decisions are related to the mode of tumor progression (local progression or distant metastasis), the number (oligometastases or multiple lesions), the size, the patient’s general condition, the presence of concomitant disease, and the length of time the disease has been under control after prior use of standard therapy.
There is a need for a “multiple disciplinary team (MDT)” discussion to develop the best treatment plan that takes into account the individual patient’s situation with reference to professional guidelines.
Let’s take a look at Ms. He’s story and see how the MDT discussed and developed a plan for the difficult situation of brain metastases after first-line treatment for lung cancer .
Ms. He’s story
When Ms. He started coughing and coughing up sputum for no apparent reason a year ago, with recurrent episodes of coughing and hemoptysis, she went to the hospital for a thorough examination and was diagnosed with lung adenocarcinoma, which was advanced, with multiple metastases in both lungs and lost to surgery. Fortunately, her tumor tissue genetic testing suggested a L858R mutation on exon 21 of the lung cancer driver gene EGFR. This is a sensitive mutation site.
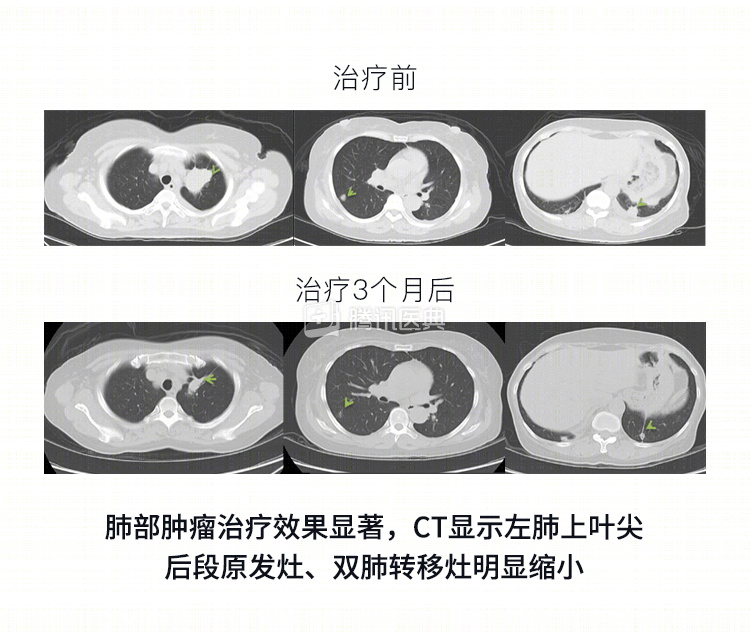
According to US and Chinese lung cancer guidelines, her doctor recommended targeted therapy with erlotinib (a first-generation EGFR inhibitor). After three months of treatment, Ms. He reviewed her CT and found that the tumor lesions had shrunk a lot, and some of them had almost disappeared.
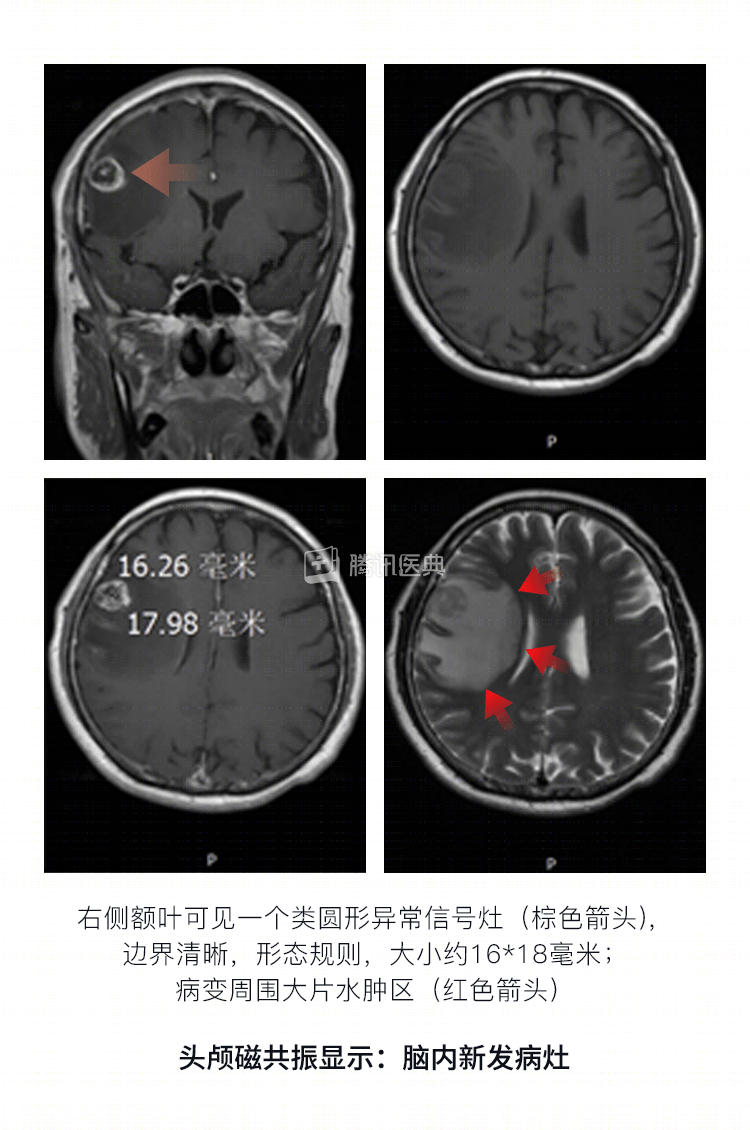
However, eight months later, she developed a headache with dizziness. The doctor suggested a cranial MRI, which revealed a metastatic lesion in the brain; and a chest CT suggested that the lesion in the chest was little changed from before.
Ms. He was puzzled: the lung lesion was well controlled, so why did it metastasize? Is it because the medication is no longer effective?
First MDT discussion: How are brain metastases managed?
The supervising physician called the first MDT discussion for her.
Medical oncologists:
Ms. He had well-controlled intrapulmonary lesions that lasted for 8 months and had no other clinical symptoms, and a single new intracranial lesion that was locally progressive.
Patients with EGFR mutations who develop local progression after targeted therapy are able to prolong tumor control by continuing to take the original drug and combining it with local therapy (i.e., treating brain metastases alone). Therefore, for Ms. He, the appropriate treatment is to continue erlotinib in combination with local therapy to deal with intracranial metastases.
Radiologists:
Whole brain radiotherapy (WBRT) combined with stereotactic radiosurgery (SRS) was previously recommended for a single brain metastasis like Ms. Ho’s. WBRT reduces the appearance of new intracranial lesions.
But recent studies have shown that SRS alone provides the same survival benefit while reducing the adverse effects of whole-brain radiotherapy, and that SRS is an elective treatment strategy for Ms. Ho, pending the surgeon’s first evaluation for surgical resection.
Surgeon oncologists:
The metastases are in a relatively superficial location in the brain, between 1 and 3 cm in size, and Ms. Ho is in fair health to have surgery. There are several benefits of performing surgery: 1. Removing the metastases can eliminate the irritation of the metastases to the surrounding brain tissue and quickly relieve the symptoms; 2. Obtaining the tumor tissue allows genetic testing and preparation for future targeted therapy; 3. Surgery can remove the entire tumor and achieve local cure. According to domestic and international clinical guidelines, surgical treatment is more appropriate.
Finally, doctors of all specialties agreed that aggressive intervention of brain metastases could bring comparative benefit to Ms. He and that surgical treatment is more appropriate, while continuing erlotinib.
One week later, Ms. He underwent successful surgical resection of her brain tumor in neurosurgery. Genetic testing for brain metastases showed that both mutations, L858R and T790M, were positive. The L858R mutation is a sensitive mutation that can control tumor development with erlotinib; T790M is a drug-resistant mutation that is ineffective with first-generation targeted drugs such as erlotinib, and the third-generation targeted drug, oseltinib, is a drug that specifically restrains this drug-resistant target, as described earlier.
Ms. He was again torn: Should we switch to axitinib immediately?
Second MDT discussion: do we need to switch to axitinib right away?
A second MDT discussion: do we need to switch to axitinib immediately?
A second MDT discussion was called by her supervising physician.
Surgeon oncologist:
Genetic testing of the brain metastases showed a T790M mutation (+), which may lead to erlotinib resistance. According to US and national guidelines, ositinib could be one of her subsequent treatment options, but the timing of its use needs to be discussed.
Medical oncologists:
Ms. Ho’s intracranial lesion has been resected. There are no other new distant metastatic lesions and the lung lesions are stable and controlled, and erlotinib is still effective against intra-pulmonary tumors, so erlotinib therapy can be continued to extend the overall benefit. After the disease has progressed, treatment can then be switched to oseltinib.
Finally, Ms. Ho continued treatment with erlotinib, and her disease is now well controlled.
Disclaimer:
Tumor disease and treatment options are extremely complex and treatment should be fully individualized, and this case does not represent a treatment decision for a “similar patient. Please seek professional advice from a competent physician regarding your specific treatment plan.
Co-authors: Dr. Zhiyong Chen, Guangdong Provincial People’s Hospital, Guangdong Lung Cancer Institute, Dr. Xuewu Wei