“Neoadjuvant chemotherapy”-chemotherapy before surgery
There is a mode of chemotherapy that is administered before surgery or radiation therapy called “neoadjuvant chemotherapy.
The professional community believes that surgery is possible for non-small cell lung cancer (NSCLC) staged in stages I through IIIA, but many tumors are in this range but are in bad locations or encircle important organs such as blood vessels, and may not be completely removed or may be too large to be removed if operated on directly. So, can we shrink the tumor a little bit first and then operate?
This is the idea of “neoadjuvant chemotherapy”.
This is the idea of “neoadjuvant chemotherapy.
Theoretically, neoadjuvant therapy has the following advantages:
Theoretically, neoadjuvant therapy has the following advantages
Which patients are candidates for “neoadjuvant chemotherapy”?
According to the National Comprehensive Cancer Institute, neoadjuvant chemotherapy is the most appropriate treatment for patients with cancer.
According to the NSCLC guidelines published by The National Comprehensive Cancer Network (NCCN), the primary population for neoadjuvant therapy is a subset of patients with stage IIIa NSCLC, such as:
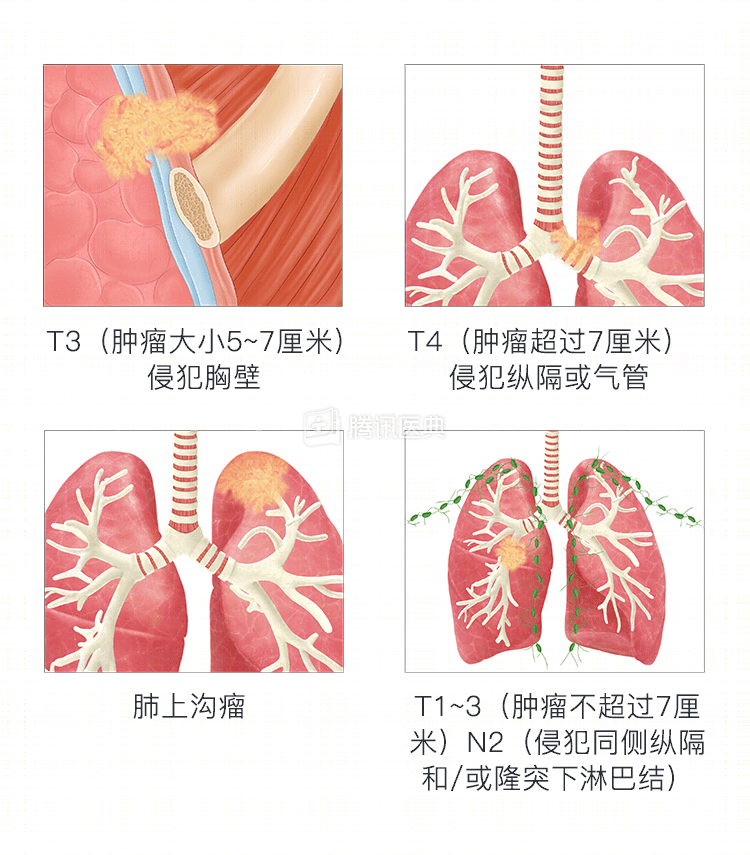
- T3 (tumor size between 5 and 7 cm) invading the chest wall;
- T4 (tumor greater than 7 cm) invading mediastinal structures or the trachea;
- Supraspinal sulcus tumor (T3-4N0-1), with N0 meaning no lymph node metastasis and N1 meaning invasion of the ipsilateral parabronchial lymph nodes and/or hilar/intrapulmonary lymph nodes;
- T1-3 (tumor not more than 7 cm)/N2 [invasion of ipsilateral mediastinal and/or infraluminal lymph nodes] lesions.
What regimen is used for “neoadjuvant chemotherapy”?
What is the most common neoadjuvant chemotherapy regimen?
The common neoadjuvant chemotherapy currently used is the platinum-containing two-drug regimen, which includes:
Cisplatin or carboplatin in combination with one of the following: vincristine/paclitaxel/docetaxel/pemetrexed (non-squamous cancers only)/gemcitabine.
If complications arise or are not tolerated with cisplatin, your doctor will adjust to a carboplatin-containing regimen.
How effective is neoadjuvant chemotherapy?
The objective efficiency of neoadjuvant chemotherapy is focused around 30% to 50%. Most studies have reported an overall survival benefit from preoperative chemotherapy, such as Burdett et al. collected 7 studies from 1990 to 2005 including 988 patients, and the analysis showed that neoadjuvant chemotherapy improved survival compared with adjuvant chemotherapy (chemotherapy administered after surgery).
However, no definitive conclusion has been reached as to whether neoadjuvant or adjuvant chemotherapy is better or worse, and medical doctors are still conducting research.
Many more efficient neoadjuvant therapies, such as neoadjuvant targeted therapy and neoadjuvant immunotherapy, are also being investigated as treatment modalities.
Co-reviewed by: Guangdong Provincial People’s Hospital Guangdong Lung Cancer Research Institute Dr. Haiyan Tu, deputy chief physician Dr. Yue-Li Sun Dr. Lun-Xi Peng