Nowadays, lung cancer has become the number one cancer in China, taking away 626,000 lives every year. In the face of a slightly abnormal lung test report, people often become nervous and feel at risk.
In recent years, the term “lung nodules” has become a hot search term on major medical websites. This is an imaging diagnosis, and any lung shadow less than 3 cm in diameter found on a chest X-ray or chest CT is called a lung nodule. .
As the awareness of “early diagnosis and treatment” of cancer spreads and CT imaging technology improves, more and more lung nodules are being detected.
According to overseas survey data, the detection rate of lung nodules among people aged 18-24 is more than 1‰, and the detection rate increases gradually with the age of people, and the detection rate among people aged 55-64 is nearly 2%.
Considering the air pollution and dietary habits, the incidence of pulmonary nodules in our population may be even higher.
However, the mixed information of good and bad makes the people confused, what is the relationship between lung nodules and lung cancer? Do the dreaded lung nodules have to be eliminated? Today, let’s talk about 5 facts about lung nodules, so that we can understand this clinical phenomenon clearly in a comprehensive and objective way.
If a lung nodule is detected and I am so worried, does it have to be lung cancer?
.
Fact: This worry is overwhelmingly superfluous.
Patients who get a “lung nodule” are more likely to have lung cancer.
When patients get a diagnosis of “lung nodules,” they are often extremely nervous and even anxious, but in the doctor’s opinion, it’s not that bad.
First, in terms of probability, the vast majority of lung nodules found for the first time are benign (inflammation, tuberculosis, scarring, lymph nodes, etc.) and less than 20% are likely to be malignant. Second, even in the case of lung cancer, the vast majority are in the early stages and with appropriate treatment will hardly affect the patient’s normal life expectancy.
Therefore, from the perspective of early diagnosis and treatment of cancer, the detection of lung nodules is a fortunate event that overwhelmingly ends in a comedy, and excessive worry mostly proves to be superfluous in the end. At this moment, the more important thing is to find a good doctor who can use his expertise to help you turn a happy ending into a reality at minimal cost. .
Is it easy to find lung cancer in lung nodules?
Fact: Ruling out lung cancer is a highly technical task.
One of the most important things to do after finding a lung nodule is to rule out lung cancer. However, most lung nodules are found incidentally on examination and are not accompanied by clinical symptoms. Ruling out lung cancer is not easy because there are no characteristic clinical signs and the nodules are small and do not have obvious imaging features.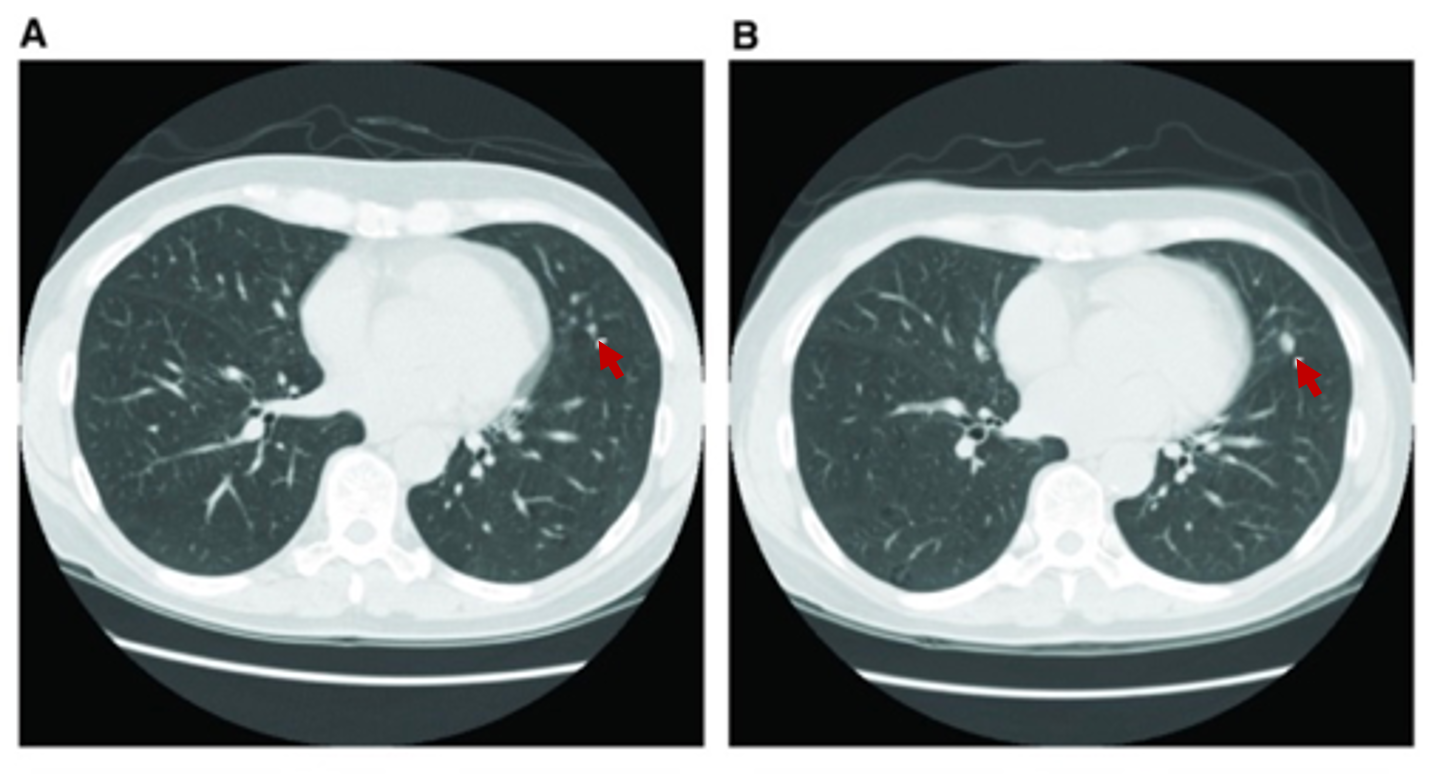
▲ (A 62-year-old woman with low-dose spiral CT detected a lung nodule that increased from 3 mm to 6 mm a year ago.)
Source: Early detection of lung cancer, F1000Res., 2016.5
There are 3 things that need to be accomplished in order to rule out lung cancer:
1) Clarify whether you are at high risk for lung cancer
This is critical when your doctor is assessing the benignity of the nodule!
These high-risk factors include the patient’s age, lifestyle habits, long-term environmental exposure, previous health status, and genetic information. For example, do you smoke or have you ever smoked? Is there a history of exposure to carcinogens (asbestos, radon, radium, etc.)? Have you ever had other cancers? Are there other lung diseases such as emphysema or pulmonary fibrosis? Have parents, brothers and children ever had cancer?
It is important to note that being at high risk does not mean that a lung nodule is necessarily lung cancer, nor does being at low risk mean that it is not; it is really a matter of probability.
② Complete a high-quality CT
Chest radiographs and low-quality CT are difficult to meet diagnostic needs, and PET-CT, a functional test with high expectations, is only suitable for identifying larger, solid nodules. Currently, high-resolution CT (HRCT) combined with various imaging techniques provides the most comprehensive and accurate characterization of pulmonary nodules.
③ It is most important to find a team that is both specialized and experienced.
This team needs to include thoracic surgeons, radiologists, and pulmonary physicians.
Considering the current shortage of medical resources in this country, which few patients have access to, it would be relatively more realistic to find an experienced surgeon at a larger medical center. 
What should I do after characterizing a lung nodule?
Fact: Benign lesions should be left alone, and malignant should be promptly biopsied.
After thorough consideration of the degree of risk for cancer, tumor site, and CT presentation, the physician will assess the risk of the lung nodule being lung cancer, and depending on the results of the assessment, the patient may receive the following treatment
1) If the imaging is clearly benign or the lesion is less than 6 mm in diameter, it does not require any further treatment
A subset of benign lesions have a very typical presentation on CT and the diagnosis can be confirmed on imaging alone, at which point a biopsy is not required.
As the quality of CT imaging has improved, many very small lung nodules have been detected. The likelihood of this portion of lung nodules being lung cancer is extremely low (<1%), and even if they are lung cancer, they are mostly inert tumors that grow slowly, can live peacefully with the body for a long time, and do not necessarily need to be removed from the body.
② If the lesion is more likely to be lung cancer and is estimated to be more malignant, timely biopsy or surgery is needed to clarify the diagnosis.
Some of the more malignant lung cancers have characteristic manifestations on CT, such as larger size, more solid components, and active growth of tumors and blood vessels. Timely surgical biopsy in such cases can avoid the risk of tumor metastasis during the waiting process.
Does it have to be surgically removed “just in time” if it is difficult to identify it?
Facts: Follow up for a period of time and then have surgery when the lung cancer is confirmed.
In the past, surgical resection used to be the preferred treatment option for pulmonary nodules, and the idea of “timely and complete removal of the lesion” was widely accepted by doctors and patients for some time.
However, as the understanding of pulmonary nodules progressed, it became clear that a significant proportion of resected pulmonary nodules were benign or low-grade malignant lung cancer. Compared with patients who do not have surgery, surgical patients do not benefit in terms of survival from the removal of the lesion; rather, the removal of lung tissue often affects the patient’s quality of life or creates problems for possible future lung surgery.
As a result, the indications for surgery for pulmonary nodules are becoming more stringent, and more patients are waiting for a period of time before surgery or biopsy to repeat CT exams to improve diagnostic accuracy by observing changes in the nodule, which is medically referred to as “follow-up”.
This is like judging a person by the first meeting alone, which is often wrong, but as the saying goes, “you can see people’s hearts with time”. There are more than a dozen combinations of follow-up plans, depending on the chance of a lung nodule being lung cancer, which need to be developed by a medical professional.
Should everyone diagnosed with lung cancer have surgery?
Fact: A high level individualized treatment plan is the answer that is right for you.
“Sometimes to heal, often to help, always to comfort.” A widely circulated interpretation of medicine on Dr. Trudeau’s epitaph.
We often say that maximizing the benefit to the patient is the central purpose of all medical practice. A qualified physician should evaluate the specific situation comprehensively and develop an individualized plan that is in the patient’s interest based on the degree of disease awareness.
For example, in the same case of an early stage lung cancer of 1.0 cm in diameter, the primary treatment goal for a 40-year-old patient is to remove the lesion in time to ensure a cure and return him to society as a healthy person.
When replaced with an 80-year-old, the patient’s survival is hardly benefited by surgery, and the risk of complications and low lung function associated with surgery can affect the quality of life in later life, when surgery is not an appropriate treatment option.
If we then switch to successful individuals in their 50s who are facing the last push of their careers, closely monitor the progress of the nodules and wait 3 to 5 years to achieve their career dreams before surgery, there will still be a good chance of cure.
In conclusion, you don’t need to worry too much after finding a pulmonary nodule, find a professional and experienced team, and the doctor’s expertise will help you get through this.
- Author: Wu Hao, Deputy Chief Physician of Thoracic Surgery, Peking University Shenzhen Hospital, M.D., Master’s Degree Supervisor; Standing Committee Member of the Guangdong Health Management Society for Thoracic Tumor and Lung Nodule Management, Member of the Thoracic Surgery Committee of Shenzhen Medical Association, Deputy Leader of the Minimally Invasive Group; has been engaged in clinical work of thoracic surgery for nearly 20 years, specializing in the application of thoracoscopy He specializes in the treatment of lung cancer, bronchiectasis, spontaneous pneumothorax, esophageal cancer, myasthenia gravis, mediastinal tumors, correction of funnel chest (Nuss surgery), hand sweating, etc. He studied under Professor Wang Jun, Director of Thoracic Surgery at Peking University People’s Hospital, who is the “first person to perform thoracoscopic surgery in China”.