- Radiotherapy for lung cancer is a treatment that uses various types of radioactivity to kill tumors, including photon rays, high LET rays from various gas pedals, and alpha, beta, and gamma rays from radionuclides;
- Photon rays have the advantage of high penetration and low dose to the skin, which is beneficial for treating deeper tumors while protecting superficial normal tissues such as the skin;
- High LET rays precisely “envelop” the entire tumor target area, hardly harming the normal tissues around the lesion, with higher biological effects, which is more conducive to efficient tumor killing;
- Low LET alpha, beta, and gamma rays are “brachytherapy” modalities with the disadvantage of small irradiation range, uneven dose distribution, and long half-life of nuclides, which are suitable for patients with recurrent lung cancer or residual lesions.
Radiation therapy (radiotherapy), as the name implies, is a treatment that uses various types of radiation to kill tumors and is one of the classic “troika” of cancer treatment.
To understand the “power” of different types of radiation, one needs to understand the concept of linear energy transfer (LET), which refers to the efficiency of energy transfer along the path of ionizing radiation. For the same absorbed dose, the higher the LET, the more concentrated the energy produced, the stronger the biological effects, and the more “powerful” the radiation.
On this basis, let’s look at the three main types of radiation currently used in lung cancer radiotherapy.
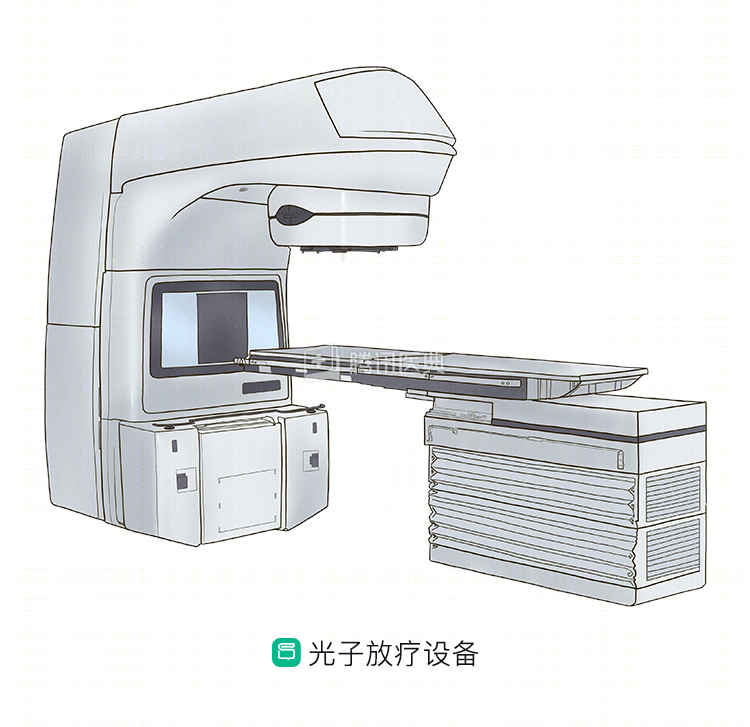
The first type: photon rays
.
The first is the most common type of photon ray, and is commonly used clinically as a 6- to 10-megavolt X-ray (megavolt is a unit of energy). It is a low LET ray (LET value 0.2 to 2 KeV/um). It has the advantages of high penetration, low skin dose (its highest dose point is in the range of 1.5-2.5 cm below the skin), and low backscatter, which facilitates treatment of deeper tumors while protecting superficial normal tissues such as skin.
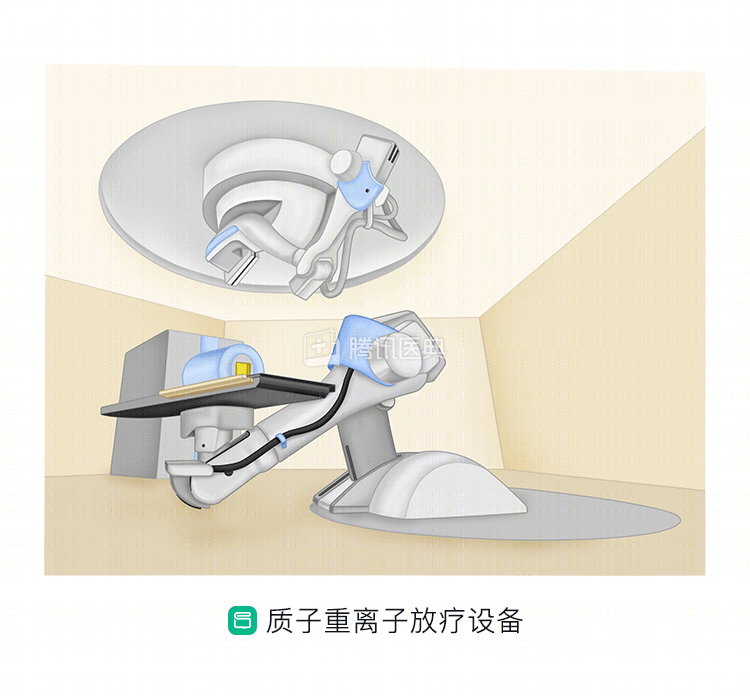
The second type: high LET rays from all types of accelerators
The second is the high LET rays produced by various types of gas pedals, which include both uncharged neutrons (LET values of 20-100 KeV/um) and charged protons, carbon ions (LET values of 100-1000 KeV/um), and so on.
The characteristics of high LET rays compared to photon rays are:
- The Bragg peak, without going into the terminology, is a high dose area with a low dose outside the peak (Figure); the width and depth of the “Bragg peak” and the shape of the particle beam can be adjusted to better match the shape of the lesion. During treatment, the “Bragg peak” of the particle beam overlaps the tumor lesion and precisely “envelops” the entire tumor target area, allowing high-dose irradiation of the tumor with little damage to the normal tissue surrounding the lesion.
- The biological effect is higher, which is more efficient in killing tumors.
The professional community has begun to explore the use of proton radiotherapy in lung cancer, and phase III clinical studies are underway overseas to compare the efficacy and adverse effects of protons versus photons (X-rays) in lung cancer.
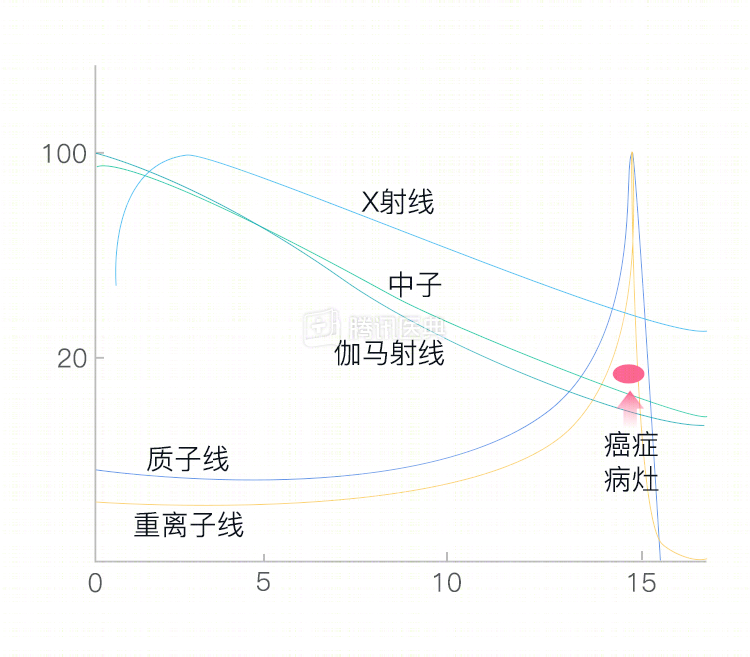
Figure: Bragg peak unique to high LET rays (proton and heavy ion lines)
Related reading
Third type: α, β, γ rays from radionuclides
These rays are also low LET rays. Unlike the first two types of radiation therapy, this type of radiation is used more as a “brachytherapy” modality. Most often, radionuclides (such as iodine-125, palladium-103, iridium-169, etc.) are “implanted” into the tumor under the guidance of imaging techniques such as CT.
The advantage is that the radiation dose is high in a certain area around the source, while the radiation dose outside the source decays rapidly, resulting in low damage to the normal tissue surrounding the tumor. It has the disadvantages of small irradiation range, uneven dose distribution, and long half-life of the nuclide. Therefore, it needs to be selected with caution after multidisciplinary expert discussion (MDT) and is mainly used for patients with recurrent lung cancer or residual lesions.
Related reading: