How does a 48 year-old woman who has noticed a swelling in her left breast for six months and has noticed a significantly larger swelling in her breast with pain in the last 2 months manage it?
Breast examination initially suggests breast cancer
This woman found a swelling in the upper outer part of her left breast six months ago, about the size of an egg, hard and movable when pushed, with no pain at the time. The swelling in the breast increased significantly from 2 months ago to approximately 5 cm in size, and the swelling was intermittently painful with pins and needles. The patient recalled that no other member of her family had a malignant tumor.
The physician found no abnormalities in her general condition and focused on breast examination, which revealed bilateral breast asymmetry, an enlarged left breast with mild nipple invagination, and a mass felt in the upper part of the left outer breast that was more than 5 cm in size, hard in texture, and with an impalpable border and poor mobility. The doctor also felt a mass in the left axilla, which was judged to be several enlarged lymph nodes with a hard texture, some of which were fused and fixed in position, the largest being approximately 2 cm by 3 cm.
The above examination led to the initial suspicion of breast cancer, and further testing was recommended.
Imaging further suggested cancer, and bone metastases were found
.
The woman underwent multiple imaging tests on the advice of her doctor. Ultrasound, mammography, and magnetic resonance imaging (MRI) all suggested that the breast mass was highly likely to be malignant, and lymph node metastases were suspected. The physician recommended further whole-body examinations.
Thoracic CT showed enlarged mediastinum (located between the thoracic cavities in the middle of the chest) and left axillary lymph nodes, a left breast lesion, and lesions in some thoracic vertebrae, and abdominal CT also revealed lesions in some thoracolumbar vertebrae. The MRI of the thoracic spine revealed abnormal signals in some of the vertebrae of the thoracic spine, not excluding metastases, and further investigation is recommended.
Because the CT suggested a thoracic spine lesion, the physician recommended a whole-body bone radionuclide scan (ECT), which is the most commonly used primary screening method for bone metastases. eCT revealed lesions in part of the right rib, part of the thoracic spine, and the upper femur of the right thigh, suspecting multiple bone metastases. Although bone biopsy pathology is the gold standard for the diagnosis of bone metastatic carcinoma, it is less commonly used given its operational difficulty and risk.
Biopsy pathology confirms advanced stage, and treatment should not be abandoned
Biopsy pathology is the gold standard for diagnosis. After a puncture biopsy of the breast mass, pathology revealed invasive ductal carcinoma, grade II. The woman was diagnosed with invasive ductal carcinoma of the left breast cT3N2M1 stage IV with multiple bone metastases. Invasive breast cancer is a common histologic type of breast cancer, and invasive ductal carcinoma accounts for 80% of it. Her breast cancer was graded as grade II, suggesting a moderate degree of malignancy.
This woman has a large primary tumor in her breast and multiple bone metastases throughout her body, making her a stage IV breast cancer, or advanced breast cancer. However, advanced breast cancer does not mean that it is untreated, and the tumor can be effectively controlled with regular treatment. According to European statistics, the survival rate of patients with stage IV breast cancer at first diagnosis 5 years can reach 26%, which is even better than the overall survival of some malignant tumors. Therefore, even advanced breast cancer should not be abandoned for treatment.
Fighting the “good fight” of systemic therapy
For advanced breast cancer, systemic treatment is usually the primary treatment, supplemented by local treatment, to control tumor progression, relieve symptoms, prolong survival, and improve quality of life.
Specifically, systemic therapy is a constant battle in which the physician considers the characteristics of the tumor, the metastatic site and criticality of the disease, the patient’s tolerance and compliance with treatment, and the patient’s financial and psychological status. This woman’s immunohistochemical tests suggest that she is positive for estrogen receptor (ER) and progesterone receptor (PR), which is a hormone receptor-positive breast cancer, and endocrine therapy is usually given priority. A series of studies have demonstrated that endocrine therapy is no less effective than chemotherapy in hormone receptor-positive advanced breast cancer and has the following advantages over chemotherapy:
- Less impact on normal cells and fewer side effects;
- Slower onset of action than chemotherapy, but once effective, longer maintenance;
- Lower cost of treatment;
- Most of the drugs are administered orally and are easy to use.
In conclusion, for the right patients, endocrine therapy not only postpones the relief chemotherapy, but also has a higher quality of life and better patient acceptance during treatment. However, for some people who are resistant to endocrine therapy, have rapidly progressing tumors, and have metastases to internal organs, physicians will consider giving priority to systemic chemotherapy, which has a more rapid onset of action.
For those who decide to use endocrine therapy, physicians will consider menstrual status and prior endocrine drug use when choosing a drug. In postmenopausal patients, third-generation aromatase inhibitors, estrogen receptor downregulators, estrogen receptor modulators, and progesterone analogs can be considered, whereas premenopausal patients need ovarian suppression (OFS) before considering these drugs. Surgery and radiotherapy are gradually replaced by drugs due to their disadvantages in terms of reversibility, control and side effects, but surgery for OFS is also a suitable option for some patients who are financially disadvantaged or nearing menopause. Endocrine therapy should usually be used until the disease progresses or is intolerable.
This woman is not yet menopausal and should undergo OFS before choosing endocrine therapy. After surgery, the patient was treated with the aromatase inhibitor anastrozole (Anastrozole, 1 mg once daily).
Anti-bone metastasis therapy is essential
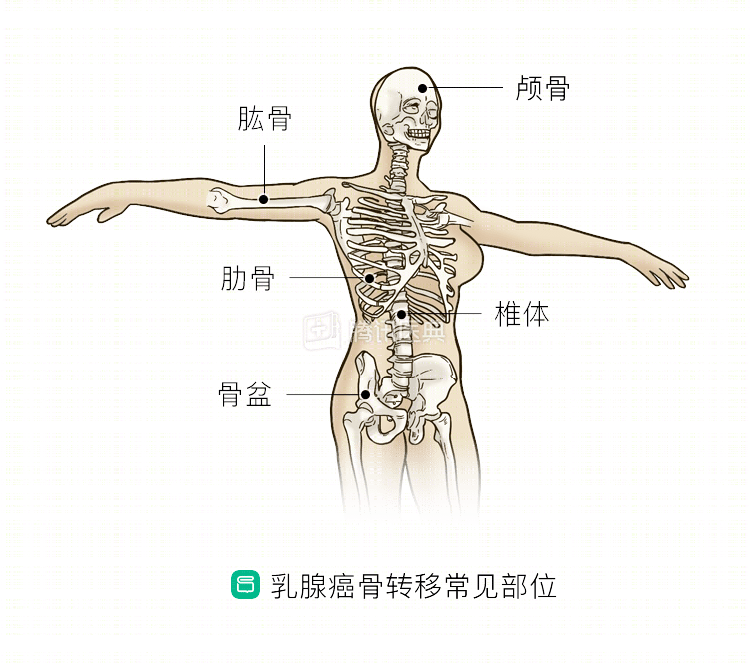
Bone metastases are the most common site of distant metastases from breast cancer. In advanced breast cancer, the incidence of bone metastases is 65% to 75%, and the vertebral body is the most common site of bone metastases from breast cancer. Bone metastases may cause bone pain, fractures, bone damage, and other bone-related symptoms. Although bone metastases themselves are usually not directly life-threatening, either bone pain or fractures can seriously affect quality of life.
The goal of treatment for breast cancer bone metastases is to reduce bone destruction, reduce symptoms such as fractures and pain, and improve quality of life. For those with bone metastases, a life expectancy of ≥3 months, and normal renal function, physicians may consider adding denosumab, zoledronic acid (Zoledronic Acid), or pamidronate disodium and Glucose along with chemotherapy or endocrine therapy, and supplementation with calcium and vitamin D. The optimal regimen for zoledronic acid is intravenous (IV) once a month, followed by every 3 months for 12 months, and is recommended until intolerable or when there is a significant decline in health status.
For this woman, the physician recommended zoledronic acid as an intravenous injection once a month.
Results after 1 year of treatment
After 1 year of systemic therapy and anti-bone metastasis treatment, the left breast was still large, the nipple was invaginated, the skin of the upper outer breast was congested, edematous, and locally broken, and the size of the swelling in the breast was not significantly different than before treatment.
Review of CT and MRI revealed a smaller lesion in the vertebral body than before treatment.
Because of complications such as skin breakdown, the surgeon recommended palliative left mastectomy + axillary lymph node dissection at this time.
To operate or not to operate? There is no definitive answer
Should you have surgery to remove the breast in the initial diagnosis of stage IV breast cancer? There is some debate about this.
Patients with good tumor properties (hormone receptor positive, HER-2 negative), only bone metastases, and young age may be considered for surgery to remove the primary site of the breast after adequate communication with the patient, or for patients who need relief or to avoid some of the complications that will occur (e.g., skin ulcers, bleeding, fungal infections, pain, etc.) after systemic therapy. The corresponding surgery will be performed after the end of systemic treatment.
For those with potentially large localized defects after tumor removal, breast surgeons work with plastic surgeons to achieve relatively optimal tumor control and healing.
Summary: The goal of treatment for advanced breast cancer is to control disease progression, improve quality of life, and prolong survival for a quality long-term survival. For hormone receptor-positive advanced breast cancer, endocrine therapy is an option, and some treatments targeting metastases are also available. During the treatment period, close follow-up is needed to determine the disease control, assess the treatment effect and toxic side effects through blood tests and imaging examinations, so as to adjust the treatment plan in time. The corresponding psychological support is also very necessary for patients with advanced breast cancer to help them build up the confidence to overcome the disease.