Breast Cancer Treatment Guidelines
(2022 Edition)
Breast cancer is one of the common malignant tumors in women, ranking first in incidence among female malignant tumors and seriously endangering women’s physical and mental health. The most important thing is that it is the most effective way to treat breast cancer.
These guidelines were developed to further standardize the practice of breast cancer treatment in China, improve the level of breast cancer treatment in medical institutions, improve the prognosis of breast cancer patients, and ensure the quality and safety of medical care.
Breast cancer screening is an effective, easy, and cost-effective way to identify and detect patients with precancerous lesions with progressive potential and early invasive cancer in asymptomatic women, with the ultimate goal of early detection, early diagnosis, and early treatment, with the goal of reducing breast cancer mortality in the population. The ultimate goal is to reduce mortality from breast cancer in the population.
Screening is divided into group screening and opportunistic screening. Group screening refers to organized and planned screening of women of appropriate age in a district or institution; opportunistic screening refers to the provision of breast cancer screening services by health care providers in conjunction with routine outpatient services.
Starting age for women to be screened for breast cancer: opportunistic screening is generally recommended
40 years of age, but for those at high risk for breast cancer, screening can begin as early as
before age 40. There is no recommended age for cohort screening in China, but the international recommendation is to start at 40 to 50 years of age. The ages used are research or exploratory in nature, and there is a lack of age-specific cost-benefit analysis in strictly randomized controlled studies
Data.
(a) Breast cancer screening strategies for women in the general risk population.
- style=”margin-left: 96pt”>
- Monthly1time breast self-examination.
- Every1 to3years span>1clinical examination.
- style=”margin-left: 96pt”>
- Suitable for opportunistic and cohort screening.
- Every1 ~2years1times breastX line examination and/ or breast ultrasound.
- For areas where conditions are not available or for dense breast glands (glands that areCtype or
Type D), breast ultrasonography may be preferred.
- style=”margin-left: 96pt”>
- Monthly1time breast self-examination.
- annually 1clinical visit.
-
Opportunity screening (imaging if symptoms or suspicious signs are present).
- style=”margin-left: 71pt”>
- Monthly1monthlybreast self-examination.
- Annually 1clinical visit.
(B) Breast cancer screening strategies for high-risk populations.
Early screening (40 years of age) is recommended for those at high risk for breast cancer, with a recommended interval of screening of 40 years per year. family:Times New Roman”>1 time, and the overall principle of screening should be combined with breast X-ray and breast ultrasound and, if necessary, MRI and other imaging modalities can be applied if necessary.
People at high risk for breast cancer meet the following 3 conditions, namely: 1. those with a significant genetic predisposition to breast cancer (see genetic testing criteria in the next paragraph); 2. those with previous breast conduction
- Monthly1monthlybreast self-examination.
Ductal or lobular atypical hyperplasia or lobular carcinoma in situ (lobular carcinoma in situ, LCIS); 3. Prior chest radiotherapy.
Hereditary breast cancer – ovarian cancer syndrome genetic testing criteria are as follows [a,b].
- Have blood relatives with BRCA1/BRCA2carriers of the mutation.
-
Compliant with the following1one or more of the following conditions for breast cancer[c]: ① Age at onset ≤45years; ② Age of onset ≤50years of age and with1 or more close blood relatives. span>[d]also for breast cancer patients with age of onset ≤50 years and/or1one and more close relatives of any age with ovarian epithelial cancer/ Fallopian tube cancer/patients with primary peritoneal cancer; (iii) single individuals with2primary breast cancer[e], and age at first presentation ≤50 years; ④ any age of onset while 2and 2 or more consanguineous close relatives with breast cancer of any age of onset and/ or ovarian epithelial cancer, fallopian tube cancer primary peritoneal carcinoma; ⑤ a consanguineous male close relative with breast cancer.
6) Combined history of ovarian epithelial cancer, fallopian tube cancer, primary peritoneal cancer.
- style=”margin-left: 71pt”>
- Patients with ovarian epithelial carcinoma, fallopian tube carcinoma, primary peritoneal carcinoma.
- Patients with male breast cancer.
- Patients with ovarian epithelial carcinoma, fallopian tube carcinoma, primary peritoneal carcinoma.
-
Have a family history of (i) any of the above conditions in the first or second degree of consanguinity; (ii) any of the third degree of consanguinity with 2 or more breast cancer patients (at least1breast cancer patient with age at presentation ≤50. New Roman”>50 years) and/or ovarian epithelial carcinoma/tubal carcinoma/Patients with primary peritoneal carcinoma.
Note: a.Meets 1 condition or more suggests a possible hereditary breast cancer –ovarian cancer syndrome and warrants specialized evaluation. When reviewing the patient’s family history, paternal and maternal relatives with cancer should be considered separately. Early-onset breast
carcinoma and / or any age Ovarian epithelial, fallopian tube, and primary peritoneal cancers suggest a possible hereditary breast cancer –ovarian cancer syndrome. In some hereditary breast cancers
– ovarian cancer syndrome also includes prostate cancer, pancreatic cancer, gastric cancer, and melanoma in some families with hereditary breast cancer– ovarian cancer syndrome. b.Other considerations: individuals with limited family history, such as female first- or second-degree relatives <2, or female The likelihood of carrying the mutation is often underestimated in cases where the age of the relative is >45 years. Testing for mutations in the BRCA1/2 gene may be considered in patients with triple-negative breast cancer with an age of onset ≤ 40 years. c.Breast cancer includes invasive and intraductal cancers. d.Next of kin refers to first-, second-, and third-degree relatives. e. 2 primary breast cancers include bilateral breast cancers or 2 of different origin on the same side of the breast with definite primary breast cancer.
The diagnosis and differential diagnosis of breast cancer should be made in conjunction with the patient’s clinical presentation, physical examination, imaging, and histopathology.
Early stage breast cancer does not have typical symptoms and signs and is not easily noticed by patients, but is often detected by physical examination or breast cancer screening. The following are typical signs of breast cancer, most often seen in the middle and late stages of the cancer.
Changes in the corresponding biochemical parameters are observed. In the case of multiple bone metastases, elevated alkaline phosphatase may be seen.
- style=”margin-left: 68pt”>
- Tumor marker testing
CA15-3 and carcinoembryonic antigen are tumor markers of high value in breast cancer, mainly used for metastatic Breast cancer patients are monitored for their disease course. The combination of CA15-3 and carcinoembryonic antigen significantly improves the sensitivity of detecting tumor recurrence and metastasis. It is not suitable for screening and diagnosis of breast cancer because of its low sensitivity to localized lesions and can be elevated in certain benign diseases and malignancies of other organs.
Pathologic diagnosis is the basis for breast cancer diagnosis and treatment. A standardized pathologic diagnosis of breast cancer requires not only an accurate pathologic diagnosis, but also correct and reliable results of markers relevant to the selection of treatment options, prediction of efficacy, and prognosis of breast cancer. When making a pathologic diagnosis, clinicians need to provide a complete and definitive clinical picture, as well as a qualified, adequate, and complete tissue specimen.
(i) Specimen type and fixation.
The main types of breast specimens include hollow-core needle aspiration biopsy specimens, vacuum-assisted biopsy specimens, and various surgical resection specimens (minimally invasive mastectomy, local excision of breast masses, mastectomy for breast lesions, mastectomy alone, modified radical mastectomy specimens, and post-neoadjuvant chemotherapy specimens for breast cancer. and modified radical specimens after neoadjuvant chemotherapy for breast cancer).
The breast tissue should be fixed immediately after puncture or excision (no more than 1 hour is appropriate). Adequate phosphate buffer preparation of 4% neutral formaldehyde fixative should be selected. Biopsy specimen fixation time of 6 to 48 hours is appropriate. For excised specimens, they should be cut at intervals of 5 to 10 mm, and it is advisable to separate adjacent tissue pieces with gauze or filter paper The tissue pieces should be separated by gauze or filter paper to ensure adequate penetration and fixation of the fixative. Fixation time 12 to 72 hours is appropriate.
(B) Guidelines for taking materials and general descriptions.
After accepting the specimen, you must first check the specimen bag information and the information on the pathology request form (including name, gender, age, bed number, hospitalization number, specimen type and site, clinical diagnosis, senders, etc.).
- Grand examination and documentation: indicate the number of punctured tissues and the size of each tissue, including diameter and length.
-
Taking of material: all tissue is taken for examination. Intraoperative pathological diagnosis is not indicated for hollow-core needle aspiration biopsy specimens.
-
Taking: all tissue sent for examination is taken. If the tissue is clinically labeled as calcified and paracalcified, it should be recorded and noted and placed in separate embedding boxes. Vacuum-assisted biopsy specimens are not suitable for intraoperative pathologic diagnosis.
-
Grand examination and documentation: determine the specimen to be sent according to the surgeon’s label. The site of the specimen should be identified as marked by the surgeon. If not marked, contact the surgeon to clarify the location of the resected specimen. Measure the size of the specimen3diameters; if skin is present, measure the skin
size. Measure the size of the tumor or suspicious lesion 3 diameter lines. Record the location and appearance of the tumor or suspicious lesion. Record the total number of sections corresponding to each piece of tissue and their numbers.
-
Taking: intraoperative frozen retrieval: every other along the long axis of the specimen. span style=”font-family:Times New Roman”>5mmdid1section, and if there is a definite mass, take the material at the mass. In case of calcified foci, it is appropriate to take the material against Xlinear radiographs of the suspicious lesion or at the location of the marked probe. If there is no clear mass, take material from the suspicious lesion.
Regular specimen sampling: If the largest diameter of the mass or suspicious lesion is ≤ 5 cm, the specimen should be taken at least every 1cm of material should be taken, and if necessary 1 of material should be taken, and if necessary [ Roman”>[such as ductal carcinoma in situ (ductal carcinoma in situ, DCIS)] it is appropriate to remove the entire lesion and send it for examination. If the largest diameter of the mass or suspicious lesion is larger than 5 cm, at least 1 cm of material should be taken for every 1 cm. font-family:Times New Roman”>1 mass, e.g. a 6cm mass should be taken at least 6 Roman”>6 masses; if a diagnosis of DCIS has been made, it is recommended that the lesion be retrieved in its entirety. All other abnormalities of the breast parenchyma and skin need to be retrieved.
- General examination and documentation. For those who freeze and send another cut edge, the cut edge should be inspected and documented.
- Identify the site of the specimen according to the surgeon’s labeling. If not marked, contact the surgeon to clarify the location of the resected specimen.
-
Measure the specimen. 3the size of the diameter line, and if skin is attached, the size of the skin is measured.
- style=”margin-left: 56pt”>
- Place the specimen correctly according to the clinical markers, and it is recommended that each cut edge of the specimen
(surface cut edge, basal cut edge, upper cut edge, lower cut edge, inner cut edge, outer cut edge) are coated with different color dyes. Allow the color markers to dry slightly and then blot up the excess dye.
- Place the specimen correctly according to the clinical markers, and it is recommended that each cut edge of the specimen
- style=”margin-left: 80pt”>
- Smear the specimen every 2 hours along the long axis in the direction from surface to substrate. 3~5mmDo
1 section, cut the specimen into several pieces of tissue in parallel, and keep the pieces in the correct orientation and order.
-
Carefully locate the lesion and measure the tumor3diameter lines; in the case of post-chemotherapy specimens, measure the size of the tumor bed; in the case of post-localization specimens, describe the size of the residual cavity and the presence of residual lesions.
-
Measure the distance of the tumor, tumor bed, or remnant cavity from each margin and observe the nearest margin.
- style=”margin-left: 55pt”>
-
Record the section number corresponding to each piece of tissue and the corresponding retrieval content.
- Taking of material.
- Taking of material.
1)Cutting edge fetching: Frozen separately sent cutting edge except for cutting edge fetching.
There are 2 main methods of cutting edge retrieval for breast-preserving specimens: vertical cutting edge radial retrieval and cutting edge off-take retrieval. These two methods have their own advantages and disadvantages. Regardless of the sampling method, it is recommended that the cut edges of the six specimens be coated with different color dyes before sampling to allow accurate localization of the cut edges according to the different colors and correct measurement of the distance between the tumor and the cut edges during microscopic observation. The pathology report of the breast-conserving specimen needs to specify the status of the cut edge (positive or negative). “Positive margins“ are defined as ink-stained margins with DCIS or invasive carcinoma invasion. The definition of “negative margins“ is inconsistent, but most guidelines or consensus define “No tumor at the ink-stained margins“” is defined by most guidelines or consensus as “negative cut margin “. For negative cut margins, it is recommended that the closest distance of the cut margin to the tumor be reported and should be described as objectively and quantitatively as possible, rather than subjectively (e.g., proximity to the cut margin, etc.).
Radiographic sampling of the vertical incisional margin: based on the surgeon’s making of the breast-conserving specimen
-
orientation marks, cut the specimen perpendicular to the base into multiple slices in parallel (recommended interval 5 mm), and each section was observed. Describe the size and location of the tumor and the distance of the tumor from each cut edge. Take all the cut edges that are largely close to the tumor together with the tumor, and sample the cut edges that are largely distant from the tumor, and accurately measure the distance between the cut edges and the tumor during microscopic observation. Vertical marginal radiographs
The advantage is that the distance between the lesion and the margin can be measured correctly, but the disadvantage is that the workload is greater and only a sample can be taken from the margin that is largely distant from the tumor.
Severed margin retrieval: Six margins are severed, and the severed margins are fully retrieved and microscopically observed for margin involvement. The advantage of dissecting the margins is that the volume of material taken is relatively small, allowing microscopic observation of all margins in a relatively small number of sections. 2) Tumor and surrounding tissue sampling: 1) If the largest diameter of the mass or suspicious lesion
≤5cm, at least every 1cm along the largest section of the tumor or suspicious lesion should be taken. New Roman”>1cm, and if necessary (e.g., DCIS), all of them should be taken and sent for examination. The material is taken and sent for examination. If the maximum diameter of the mass or suspicious lesion is larger than 5 cm, at least 1 cm per 1 cm should be retrieved font-family:Times New Roman”>1 block; if a diagnosis of DCIS has been made, it is recommended that the lesion be taken in its entirety. If the specimen is post-neoadjuvant chemotherapy, the pathological diagnosis specification for post-neoadjuvant breast cancer (2020 version) is referred to for sampling. In case of surgical residual cavity: send representative sections, including suspected residual lesions. ② Other abnormalities of the breast parenchyma. (iii) Skin.
3) Additional margin sampling: If the margin was positive at the time of the initial excision, the margin needs to be sent again for examination. The supplemental margin can also be sent as a separate specimen with the resected tissue. If the surgeon has marked the true margin of the supplemental margin, the true margin can be colored with dye and the specimen can be attached perpendicular to the marked margin.
Continue to dissect and send for examination. If the specimen is small, all the tissue should be sent for examination.
- Grand examination and documentation: ① Place the specimen in the correct orientation to identify the quadrant where the tumor is located: modified radical specimens can be correctly positioned by identifying the axillary The modified radical specimen can be correctly positioned by identifying the axillary tissue (axillary tissue facing upwards). For simple resection specimens, positioning is based on the surgeon’s markings or, if the orientation is not marked, contact the surgeon to determine the correct orientation of the specimen. It is recommended that the basal cut edge of the specimen be coated with dye to allow microscopic visualization of the cut edge. ② Measure the size of the entire specimen and the accompanying skin and axillary tissue. Describe the appearance of the skin, such as the presence of surgical incisions, puncture points, scarring, erythema, or edema. The nipple is incised horizontally from the base and a horizontal section of the nipple is taken to visualize the transverse section of the milk ducts, and the rest of the nipple is incised perpendicular to the surface of the breast. The appearance of the nipple and areola is described, such as the presence of rupture and eczema-like changes. ④ The specimen is cut into continuous slices perpendicular to the base. ⑤ Carefully locate the lesion, record the location of the quadrant where the lesion is located, and describe the characteristics of the tumor (texture, color, borders, relationship to skin and deep structures). Measure the size of the tumor3diameters if there is a definite mass; measure the size of the tumor bed if it is a post-chemotherapy specimen; if it is a post-local excision specimen, then The size of the surgical residual cavity and the presence of residual lesions were described. Measure the distance of the tumor, residual cavity, and tumor bed from the nearest surface margin and basal margin. (6) Describe the condition of the non-tumor breast tissue. (7) After dissecting the axillary adipose tissue from the specimen, carefully search for lymph nodes, at least 15 lymph nodes for a standardized axillary sweep specimen. Describe the total number of lymph nodes and their maximum diameter, the presence or absence of fusion, and the presence or absence of adhesions to surrounding tissue. Note the connective tissue surrounding the lymph nodes.
- style=”margin-left: 96pt”>
- Take.
-
Taking of primary tumor and surgical residual cavity: In case of tumor: send the largest section of the tumor for examination; if the maximum diameter of the mass or suspicious lesion is ≤5cm, it should be taken at least every1cmfetch1 The patient should have >block, and if necessary (e.g.DCIS) it is advisable to All specimens are taken and sent for examination. If the maximum diameter of the specimen mass or suspicious lesion is >5 cm, then each family:Times New Roman”>1cmat least fetch1block, if diagnosed withDCIS, all lesions should be retrieved .
In case of post-chemotherapy tumor bed: refer to the Diagnostic Pathology Specifications for Post-Neoadjuvant Breast Cancer (2020 year edition) for sampling.
In case of surgical residual cavity: send representative sections, including suspected residual disease
Foci.
- style=”margin-left: 81pt”>
- Abnormal foci in the remaining tissues: papillae: the surface closest to the tumor is
overlying skin; basal cut margin closest to the tumor, taking a vertical section of the margin if possible; representative sampling of 1 block of breast tissue per quadrant in the surrounding quadrant.
Lymph nodes in the axilla: if the lymph node is negative by visual inspection, the entire lymph node is sent for histological examination; if the lymph node is positive by visual inspection, the tissue is dissected along the largest diameter of the lymph node and sent for examination, with attention to the connective tissue surrounding the lymph node to identify If the lymph node is positive to the naked eye, the tissue is dissected along the largest diameter of the lymph node and sent for examination.
Sentinel lymph node biopsy for breast cancer (Sentinel lymph node biopsy, < span style="font-family:Times New Roman">SLNB) has gradually replaced the traditional axillary lymph node dissection to assess the regional lymph nodes in patients with early-stage breast cancer, SLNB negative patients can avoid the need for a lymph node biopsy. span>negative patients can avoid axillary lymph node dissection.
- style=”margin-left: 96pt”>
- Definition of anterior lymph node metastases.
-
Isolated tumor cells (< isolated tumor cells, , ITC): tumor lesion diameter in lymph nodes≤0.2mm: tumor cells in lymph nodes, or on a single slice <200pcs. AJCCdefines it aspN0(i+). Most current clinical breast cancer guidelines considerITCnot clinically significant and recommend treatment as negative axillary lymph nodes.
-
Micro-metastases: tumor metastases with a maximum diameter >0.2mm, but not more than2mm < span style="font-family:Arial">. AJCCdefines it aspN1mi. ITCis fundamentally different from microtransfer, which ispN0 and the latter ispN1, and the identification of the two is very important. In this standard, it is recommended that the anterior lymph nodes be spaced2 mmsegmented into several pieces of tissue, mainly for the purpose of maximizing detection of micrometastatic lesions.
- style=”margin-left: 55pt”>
- Macro-metastases: the maximum diameter of tumor metastases > >2mm.
- Macro-metastases: the maximum diameter of tumor metastases > >2mm.
-
Intraoperative Pathologic Assessment: The primary goal of intraoperative pathologic assessment in the sentinel lymph node is to detect the lymph node. The main purpose is to detect metastatic lesions in the lymph nodes so that axillary lymph node dissection can be performed to avoid secondary surgery. However, there is controversy as to whether intraoperative pathologic evaluation of the anterior lymph nodes is necessary. The main methods of intraoperative pathologic evaluation include intraoperative cytograms and intraoperative frozen sections.
- Intraoperative cytology slides: lymph nodes are spaced at 2mmsections of lymph nodes were cut into several pieces of tissue, and each piece of tissue was carefully examined for the presence of metastases visible to the naked eye, and cytology prints were performed on each section. Pap staining andHEstaining are recommended. The advantages of intraoperative cytology printing are that the entire lymph node tissue can be preserved without tissue loss, different sections of the lymph node can be taken, it is inexpensive, requires little time, and is a simple procedure; the disadvantage is that it is difficult to identify scattered cancer cells (e.g., lobular carcinoma) in the high cellular background of the print. The intraoperative cytology print has good diagnostic specificity, but its diagnosis
Sensitivity is influenced by several factors.
-
Intraoperative frozen section: the lymph nodes are sliced at each interval. style=”font-family:Times New Roman”>2 mminto several slices of tissue, and each slice is carefully examined for the presence of metastases visible to the naked eye, and each slice is made into a frozen section for pathologic evaluation. The advantages of intraoperative frozen sectioning are good diagnostic specificity and avoidance of unnecessary axillary lymph node dissection due to false positives; the disadvantages are tissue loss, long time, high cost, and difficulty in assessing fatty lymph nodes.
-
Routine postoperative paraffin pathologic evaluation: postoperative paraffin sections are the gold standard for the diagnosis of anterior lymph nodes. It is the gold standard for the diagnosis of anterior lymph nodes and can significantly reduce the leakage of micro metastases. However, there is no unanimous opinion on how to section lymph nodes, whether serial sections are needed, how many serial sections should be cut, and how many intervals between serial sections. Recommended paraffin sectioning protocol.
1) cut the lymph nodes into several slices at 2 mm intervals; 2) embed each slice into paraffin blocks; 3) cut each block into at least (iii) at least one slice per wax block; continuous slicing at intervals of 150 to 200200200200200200. “font-family:Symbol”>m, cut 6 cuts.
(C) Pathologic diagnostic classification, grading, and staging scheme.
See Appendix 2 for histological typing based on 2012 and 2019 editions of the WHO Breast The exact differentiation of certain histological types is determined by immunohistochemistry.
The accurate histologic staging of invasive breast cancer is clinically important for individualized patient management. In the NCCN Breast Cancer Clinical Practice Guidelines for the postoperative adjuvant treatment of invasive breast cancer, the two types of breast cancer with a better prognosis, ductal carcinoma and mucinous carcinoma, have been developed as opposed to other types of invasive carcinoma.
The endocrine therapy and radiotherapy regimens for the two types of breast cancer with a better prognosis, ductal carcinoma and mucinous carcinoma, are different from those for other types of invasive breast cancer, and therefore the diagnostic criteria for these specific types of breast cancer should be strictly controlled. The NCCN clinical practice guidelines for breast cancer also set out surgical and preoperative adjuvant postoperative treatment options for inflammatory breast cancer, a type of breast cancer with a poorer prognosis, that are different from other invasive cancers. Medullary carcinoma was previously considered to have a better prognosis, but current studies suggest that its risk of metastasis is comparable to that of other highly malignant invasive carcinomas, and its diagnostic repeatability varies markedly between observers. Therefore the NCCN guidelines recommend that patients with invasive carcinoma with medullary features should receive the same treatment as invasive ductal carcinoma (invasive ductal carcinoma, IDC). Some specific types of breast cancer have more specific clinical features, such as invasive micropapillary carcinoma that is more likely to present with lymph node metastases, and even if a smaller percentage of invasive micropapillary carcinoma is present, the percentage should be noted in the pathology report. For mixed carcinomas, it is recommended to report the percentage of different tumor types and to report the expression of molecular biomarkers of tumors of 2 or more components separately.
-
Infiltrative breast cancer (see Appendix3): histologic grading is an important prognostic factor, and several studies have shown a clear correlation between histologic grading and prognosis in invasive breast cancer. The most widely used pathologic grading system for invasive carcinoma is the modified Scarff-Bloom-Richardson( Nottingham) histological scoring system, based on three important indicators: the proportion of glandular duct formation, cell heterogeneity, and nuclear schizogram count. Each index was evaluated separately and given a score of 1to. family:Times New Roman”>3scores, which were summed to classify the invasive carcinoma into 1, 2, 3There are three levels.
The assessment of the degree of glandular duct differentiation is for the whole tumor and needs to be evaluated under low magnification.
Assessment of the degree of glandular differentiation is for the whole tumor and needs to be evaluated at low magnification. Only structures with a clear central glandular lumen surrounded by polarized tumor cells were counted, expressed as a percentage of the glandular duct /tumor area.
Nuclear pleomorphism is assessed by selecting the area with the most significant pleomorphism. This assessment is based on the nuclear size, shape, and nucleolus size of the surrounding normal mammary epithelial cells. In the absence of surrounding normal cells, lymphocytes are used as a reference. When the nucleus is similar in size and shape to the surrounding normal epithelial cells and chromatin is evenly distributed, it is considered a 1 score; when the nucleus is larger than normal, with moderate variation in shape and size, and a single nucleolus is visible, it is considered a 2 points; when the nuclei are significantly different in size, with significant nucleoli and multiple nucleoli visible should be considered 3 points.
Only well-defined nuclear schizograms are counted, not nuclear densities or nuclear fragments. The nuclear schizogram counting area must be corrected for the diameter of the high magnification field of the microscope. The most actively proliferating areas are selected for nuclear schizograms counting, usually commonly at the tumor margins, and if heterogeneity in the tumor is present, areas with many nuclear schizograms are selected.
-
Mammary glandsGrading of DCIS: for DCIS< span style="font-family:Arial">, the pathology report should include grading and recommend reporting the presence of necrosis, histologic structure, lesion size or extent, and margin status. The current grading of breast carcinoma in situ is primarily a nuclear grading with the following diagnostic criteria.
Low nuclear grade DCIS: Consists of small, uniform cancer cells with stiff hitchhiking bridges, micropapillaries, sieve-like or solid structures. The nuclei are uniform in size, with uniform chromatin, inconspicuous nucleoli, and rare nuclear schwannomas.
Medium-grade DCIS: morphology is intermediate between low-grade and high-grade DCIS. Roman”>DCIS, with light –moderate differences in cell size, shape, and polarity. The chromatin varies in thickness, nucleoli may be seen, nuclear schizophrenia is visible, and punctate necrosis or acantholytic necrosis may occur.
Highly nuclear grade DCIS: composed of highly atypical cells that form micropapillar, sieve, or solid shapes. The nuclei are markedly pleomorphic, lacking polar alignment, with coarse clumped chromatin, pronounced nucleoli, and more nuclear schwannomas. Intraluminal necrosis with a large amount of necrotic debris is often seen in the lumen. However, intraluminal necrosis is not necessary for the diagnosis of high-grade DCIS, and sometimes the duct wall is lined with a single layer of cells, but the cells are highly heterogeneous, which can also be diagnosed as high-grade DCIS. Roman”>DCIS.
See Appendix 4. Tumor staging includes tumor size, extent of involvement (skin and chest wall involvement), lymph node metastases, and distant metastases. Correct tumor staging is the basis for guiding individualized treatment decisions. Patients with breast cancer should be staged clinically and pathologically.
Version 8 AJCC Breast Cancer Staging provides detailed provisions for the measurement of tumor size. Tumor size can be measured in a variety of ways, including clinical palpation, imaging assessment, gross pathological measurements, and microscopic measurements. The tumor size involved in breast cancer staging refers to the size of invasive cancer. Since physical examination, imaging, and gross examination cannot distinguish between invasive and intraductal cancers, microscopic measurement should be the most accurate method of measurement. If the invasive carcinoma is too extensive to be fully encapsulated by 1 wax block, the size of the tumor at the time of macroscopic examination will prevail. If the infiltrative carcinoma lesion is limited and can be fully embedded with 1 wax block, the tumor size is based on the size measured under the microscope. (1) If there are infiltrative and in situ cancer 2 components in the tumor tissue, the tumor size should be based on the measurement of the infiltrative component. The size of the tumor should be based on the measurement of the infiltrative component, and the extent and proportion of carcinoma in situ can be indicated. (2) Carcinoma in situ with microinfiltrate: If microinfiltrate is present, it should be indicated in the report and the maximum diameter of the microinfiltrate foci should be measured; if it is
multifocal microinfiltrates, the size of the infiltrate foci cannot be cumulative, and the multifocal microinfiltrates should be indicated in the report and the size of the largest infiltrate foci should be measured. (3) For 2 or more multiple tumor foci in the same quadrant that can be identified by visual inspection, the pathology report should indicate (more than 2 multiple tumor lesions in the same quadrant should be noted as multifocal tumors in the pathology report and measured separately. (4) For more than 2 multiple tumor lesions in different quadrants that can be determined by the naked eye, they should be noted as multicentric tumors in the pathology report. (more than 2 multiple tumor lesions in different quadrants should be noted as multicentric tumors in the pathology report and measured separately in size. (5) If the tumor tissue consists entirely of DCIS, its extent should be measured to the extent possible. Lymph node status is an important determinant of treatment and prognosis in breast cancer patients, and for lymph node metastases at staging thresholds (e.g., 1, 3, and 3) /span> and 10 metastases) nearby, the number of metastases in the lymph nodes should be particularly carefully observed to make an accurate pNstaging.
Staging of specimens after neoadjuvant therapy requires a combination of clinical examination, imaging, and pathologic examination information, based on surgical resection of the specimen for post-treatment yTyT and yN are determined based on the surgical resection specimen.
- style=”margin-left: 68pt”>
- Immunohistochemical and tumor molecular pathology assays and their quality control quality control
Estrogen receptor (estrogen receptor, estrogen receptor should be performed in all cases of invasive breast cancer. span style=”font-family:Times New Roman”>ER), progesterone receptor (progesterone receptor, PR), HER2 immunohistochemical staining, HER2 (2+) cases should be further tested by in situ hybridization. The significance of assessing ER and PR status is to identify the patient population that will benefit from endocrine therapy and to predict prognosis, and to assess the prognosis. span style=”font-family:Times New Roman”>ER and / or or PR positive patients can be treated with endocrine therapy such as tamoxifen and aromatase inhibitors. Standardized pathology reports for ER, PR need to report the intensity and percentage of positive cells. Definition of ER and PR positivity.
≥1% of positively stained tumor cells. The significance of assessing HER2 status is to identify the patient population suitable for HER2-targeted therapy and to predict prognosis. HER2 positivity is defined as.
strong staining of intact cytosol in more than 10% of cells as detected by immunohistochemistry
(3+) and / or in situ hybridization detected HER2 gene amplification (single copy HER2 gene >6 or HER2/CEP17 ratio >2.0). The ER, PR tests were referenced to the Chinese Breast Cancer ER, PR Detection Guidelines (see Annex 5 >). For HER2 testing, refer to the “Chinese Breast Cancer HER2 Testing Guidelines” (see Annex 5). =”font-family:Times New Roman”>6).
Ki-67 proliferation index plays an increasingly important role in the selection of treatment options and prognostic assessment of breast cancer The Ki-67 test should be performed in all cases of invasive breast cancer and the percentage of positively stained cells in the cancer cells should be reported. For Ki-67 counting, there is a lack of consensus. It is recommended that whole sections be evaluated at low magnification to see if the distribution of positive cells is uniform at.
If the distribution of positive cells in tumor cells is homogeneous, 3 or more invasive carcinomas can be randomly selected for high magnification field counting, yielding an average Ki-67 proliferation index.
If the positive cells are unevenly distributed in the tumor cells, there are obvious Ki-67 proliferation index high expression regions (hot spot areas). There are mainly 2 situations: 1) hotspots appear at the junction of tumor tissue margin and normal tissue, while Ki-67 proliferation index in tumor tissue is relatively low. span>proliferation index is relatively low, it is recommended to select ≥3 high magnification fields of invasive carcinoma in the tumor margin area for Ki-67 proliferation index assessment; ② in the presence of hot spot areas within the tumor tissue, the Ki-67 proliferation index of the whole section can be assessed by averaging the Ki-67 proliferation index, and the field of view should be selected to include the hot spot area including the ≥3 high magnification fields of infiltrating carcinoma were selected. When the Ki-67 proliferation index is between 10% to 30% of the threshold range, it is recommended to try to evaluate 500 or more invasive cancer cells to improve the accuracy of the results.
Laboratories performing immunohistochemistry and molecular pathology testing for breast cancer should establish complete and effective internal quality control, and units that are not equipped for testing should properly
Save specimens for testing by a qualified pathology laboratory. A qualified pathology laboratory should meet the following conditions.
-
Adequate standard operating procedures should be established and strictly followed, and each test should be well documented and archived. Repeatability analysis of staining results of different batches of the same tissue should be carried out. Instruments and equipment related to testing should be regularly maintained and calibrated. Any changes in procedures and reagents should be rigorously revalidated.
-
Laboratory technicians and pathologists involved in immunohistochemical and molecular pathology testing of breast cancer should undergo regular The laboratory technicians and pathologists engaged in immunohistochemistry and molecular pathology testing of breast cancer should undergo the necessary training, qualification assessment and competency evaluation.
-
External quality control of the laboratory can be achieved by participating in relevant external quality control activities. This is achieved by participating in relevant external QC activities. External QC should have a positive and negative compliance rate of 90% or more. External quality control activities are recommended to attend 1to2times.
The pathology report for invasive breast cancer (see Appendix 5) should include all elements relevant to the patient’s treatment and prognosis, such as tumor size, histologic type, histologic grade, presence of coexisting < span style="font-family:Times New Roman">DCIS, presence of vascular invasion, nerve invasion, papillae, cut margins, and lymph node status. It should also include ER, PR, HER2, Ki-67 , and other indicators. In case of post-treatment breast cancer specimens, pathological assessment of post-treatment response should be performed. The pathologic diagnostic report for DCIS should report the nuclear grade (low, intermediate, or high grade) and the presence or absence of necrosis (pink or punctate necrosis), the surgical margins, and the ER Roman”>ER and PR expression. For benign paracancerous lesions, it is appropriate to clearly report the name or type of lesion. The evaluation of breast-conserving specimens should include gross examination and microscopy.
The distance of the tumor from the nearest margin in the observation, and if the margin is positive, the type of tumor at the margin (carcinoma in situ or invasive) should be indicated. Lymphovascular /vascular invasion needs to be distinguished from luminal spaces caused by tissue contraction, which is often seen in breast cancer specimens. In contrast, constricted lumens are more commonly found within the tumor tissue, whereas vascular invasion is more reliably sought around the body of the tumor.
Breast cancer needs to be differentiated from benign diseases such as breast hyperplasia, fibroadenoma, cyst, intraductal papilloma, ductal dilation (plasmacytomastitis), breast tuberculosis, malignant lymphoma of the breast, mesenchymal sarcoma, and other tumors metastasizing to the breast from other sites. The differential diagnosis should be made between malignant lymphoma of the breast, sarcoma of mesenchymal origin and secondary malignant tumors of the breast that have metastasized to the breast from other primary tumors. The differential diagnosis requires a detailed history and careful physical examination, combined with imaging (breast ultrasound, breast X radiography and breast MRI) and finally cytology and / or pathological histology to clarify the diagnosis.
Breast cancer with palpable lumps on clinical examination accounts for about 80% of cases and can be diagnosed by surgical biopsy for pathology. The histological diagnosis can be made by surgical biopsy, and the diagnosis can be clarified as soon as possible with the help of a puncture biopsy in hospitals that have the conditions. However, breast cancer that is negative to clinical palpation increases the difficulty of diagnosis and requires imaging localization for lesion puncture or placement of a metal locator wire under the guidance of the breast X ray technique, followed by surgical excisional biopsy for definitive diagnosis.
A few patients with breast cancer have nipple discharge, which needs to be differentiated from breast hyperplasia, ductal dilatation, milk retention, intraductal papilloma, and papillomatosis. In the case of a few patients with breast cancer with nipple discharge, the diagnosis can be made by endoscopy and biopsy.
Breast cancer should be treated with a combination of therapies that take into account the biological behavior of the tumor and the patient’s physical condition, taking into account both local and systemic treatments, in order to improve the efficacy and quality of life of the patient.
-
LCIS: In classicLCIS the terminal ducts or alveoli in the lobules are solidly enlarged and filled with uniform consistent tumor cells. The tumor cells are small and uniform in size and poorly adherent. The nuclei are round or ovoid with uniform chromatin and inconspicuous nucleoli. The cytoplasm is lightly stained or lightly eosinophilic, and may contain mucus vacuoles that cause the nucleus to be deviated in an imprinted cell pattern, and the cytoplasm may be translucent. LCISincludes several subtypes: pleomorphic, exuberant, hyaline, and myxoid. The more important of these is the polymorphic subtype. In polymorphicLCIS, the tumor cells are poorly adherent, with significantly enlarged nuclei, markedly polymorphic, and may have prominent nucleoli and nuclear schizophrenia. The tumor is sometimes seen as acne-like necrosis or calcification, which needs to be differentiated from high-gradeDCIS. Atypical lobular hyperplasia (atypical lobular hyperplasia,< span style="font-family:Times New Roman">ALH) and LCIS are morphologically similar, but recidivate the terminal ductal lobule unit
(terminal ductal lobular unit, TDLU) to varying degrees. The diagnosis is made when ≥50% of the TDLU units are filled with diagnostic cells and dilated style=”font-family:Times New Roman”>LCIS and 50% when ALH. According to AJCC (version 8), the LCIS as a benign breast lesion, however, the panel believes it still needs to be applied with caution and recommends aggressive management of atypical LCIS.
LCIS has a relatively low risk of progression to invasive carcinoma, has a long interval between carcinomas, and has a high risk of progression to invasive carcinoma.
Bilateral breast and multiple quadrant onset are characteristic. Several studies have found that among women diagnosed with ALH and LCIS, the lifetime probability of developing cancer is < span style="font-family:Times New Roman">5% to 32%, with an average cancer rate of 8%. LCIS carcinoma is equally likely to occur in both breasts and is not limited to the primary LCIS site. Most believe that LCIS is a risk factor for cancer, while some studies consider LCIS to be a precancerous lesion. Some studies have shown that LCIS mostly progresses to invasive lobular carcinoma, but can also progress to IDC. This is a precancerous lesion that deserves attention, and its treatment requires a more effective and definitive approach.
LCIS may have no clinical symptoms or signs such as breast lumps, nipple discharge, nipple swelling and skin changes, and sometimes only hyperplasia-like changes. In Chinese women, breast X-ray, breast ultrasound and, if necessary, breast MRI should be performed. In patients who are to undergo breast-conserving surgery, preoperative breast X-ray examination must be performed. After mammographic Xray reveals calcifications, masses, or structural disturbances, they can be diagnosed by either puncture biopsy (including hollow-core needle puncture and vacuum-assisted puncture biopsy) or open biopsy. In patients with classic LCIS suggested by puncture biopsy, routine imaging follow-up can be performed without open biopsy. If the puncture biopsy suggests pleomorphic LCIS or if the puncture results are inconsistent with imaging, open biopsy is required to exclude DCIS and invasive carcinoma. span>and invasive carcinoma. LCIS has also been found on surgical biopsy for other breast lesions. Typical LCIS is very similar to low-grade DCIS and can be detected using E- calreticulin and P120 immunohistochemical staining to identify it.
LCIS may be given premenopausal tamoxifen (triamcinolone) if extensive resection is performed.
oxylamine) for 5 years; oral tamoxifen or raloxifene to reduce risk after menopause.
If polymorphic LCIS cannot be ruled out, total mastectomy with breast reconstruction as appropriate is feasible.
-
DCIS: also known as intraductal carcinoma, is a non-invasive carcinoma that occurs mostly in TDLU, which can also occur in the large ducts, is an in situ carcinoma confined to the ducts of the breast. TypicallyDCISin the breastXray mostly shows clusters of tiny calcified foci without masses, and malignant calcifications may also show tiny dot-like, linear, or branching calcifications. In practice, a grading model based on nuclear grading, taking into account necrosis, nuclear splitting and histology, is used to classify DCISas. /span>3 levels, i.e. low level, medium level and high level. High-gradeDCISoften consists of large pleomorphic cells with distinct nuclei and common nuclear divisions. Intraluminal necrosis is not necessary for the diagnosis of high-gradeDCIS. Low-gradeDCIS consists of small monomorphic cells with round nuclei, uniform size, homogeneous chromatin, inconspicuous nucleoli, and nuclear schizophrenia. The nuclei are round, uniform in size, chromatin is homogeneous, nucleoli are inconspicuous, and nuclear division is rare. The tumor cells are arranged in a rigid bridge, micropapillary, sieve, or solid shape. Intermediate-gradeDCISstructures were diverse, with cellular heterogeneity intermediate between high-grade and low-grade. “font-family:Times New Roman”>DCISbetween high and low grade.
DCIS may be IDC as a precursor lesion, and DCIS without treatment may eventually progress to IDC. Studies of DCIS that were initially misdiagnosed as benign and did not receive treatment have shown that progression from DCIS to IDC is not possible. span style=”font-family:Times New Roman”>IDC was 14% to 53%.
According to the breast characteristics of Chinese women, breast Xray, breast ultrasound and, if necessary, breast sound should be improved. -family:Times New Roman”>MRI if necessary. Patients undergoing breast-conserving surgery must be diagnosed with a preoperative breast X-ray. At least 90% of DCIS is in the breast.
DCIS is detected on screening X-ray. The majority of patients present with microcalcifications and some present with microcalcifications with mass shadows or dense shadows, about 10% of patients have palpable masses, about 6% of patients had false negative breast X radiographic findings.
- style=”margin-left: 80pt”>
- Local extended excision with whole breast radiation therapy.
- Total mastectomy, as appropriateSLNBand breast reconstruction.
For patients with simple carcinoma in situ, total axillary lymph node dissection is not recommended in the absence of evidence of invasive breast cancer or proven metastasis. However, a small percentage of patients with a clinical diagnosis of simple carcinoma in situ are found to have invasive carcinoma at the time of surgery and should be treated as such. The diagnosis of pure LCIS must be confirmed by surgical biopsy.
- Tamoxifen treatment is considered in the following cases5years to reduce the risk of ipsilateral breast cancer recurrence after breast-conserving surgery: 1) undergoing breast-conserving surgery (lumpectomy)
Patients treated with radiotherapy, especially ER-positive positive patients with DCIS; ER-negative patients with ER; ER-negative patients with DCIS patients the effect of tamoxifen treatment is uncertain. ② For DCIS patients undergoing total mastectomy, the risk of contralateral breast cancer can be reduced by oral tamoxifen or raloxifene postoperatively, but the clinical benefit of chemoprevention needs to be weighed against the adverse effects.
- style=”margin-left: 68pt”>
-
- Breast-conserving surgery plus radiation therapy.
- Breast-conserving surgery plus radiation therapy.
-
Total mastectomy combined with axillary lymph node dissection (modified radical surgery) for breast cancer with breast reconstruction as appropriate.
- style=”margin-left: 67pt”>
- Total mastectomy withSLNB, with breast reconstruction as appropriate.
- Total mastectomy withSLNB, with breast reconstruction as appropriate.
-
Breast cancer in the elderly. Local extended excision or total mastectomy (depending on surgical and anesthetic risk), endocrine therapy for receptor positive patients, as appropriateSLNB. .
The scope of breast cancer surgery includes both the breast and axillary lymph nodes. Breast surgery includes both extended tumor resection and total mastectomy. The axillary lymph nodes can be SLNB and axillary lymph node dissection, and the status of axillary lymph nodes should be understood except for in situ cancer. The choice of surgical procedure should take into account the clinical stage of the tumor and the patient’s physical condition.
-
Mastectomy: indications forTNMstaging in0Stage 0, Stages I, II and some Stages III with no contraindication to surgery, patients who are not eligible for breast-conserving surgery or who do not agree to breast-conserving surgery; patients with locally progressive disease or with distant metastases
Patients who are in a descending stage after systemic treatment may also opt for total mastectomy.
Halsted conventional radical mastectomy requires simultaneous removal of the pectoralis major and minor muscles, which is highly invasive and has a high complication rate. It has been replaced by a modified radical mastectomy with a high complication rate. The scope of resection includes the anatomical boundaries of the subclavian, inferior to the anterior rectus abdominis sheath, internal to the parasternal, and external to the latissimus dorsi muscle, together with complete excision of the pectoralis major fascia and the nipple-areola complex, and only when the pectoralis muscle is involved is part or all of the pectoralis muscle removed. Some authors believe that the pectoralis major fascia can be preserved, especially when immediate intraoperative prosthesis /expander reconstruction is required.
Current mastectomy has evolved from modified radical surgery to skin-preserving mastectomy + breast reconstruction The two treatments are similar, but the latter has better cosmetic results. In addition, mastectomy with preservation of the nipple areola is becoming more widely used in clinical practice, but long-term study data are lacking and patient selection needs to be further refined.
-
Breast-conserving surgery: strict indications for breast-conserving surgery. The medical unit performing breast-conserving surgery should have the equipment and technology for histological examination of breast-conserving surgical margins to ensure negative margins; equipment and technology for post-breast-conserving radiation therapy. The criteria for evaluating the cosmetic results after breast-conserving surgery are shown in Appendix 7.
Breast-conserving surgery is indicated for patients with a desire for breast conservation, complete excision of the breast tumor with negative margins, good cosmetic results, and access to postoperative adjuvant radiotherapy. Young age is not a contraindication to breast-conserving surgery; patients ≤ 35 years of age have a relatively high risk of recurrence and reoccurrence of breast cancer and should be fully informed of the possible risks when choosing breast conservation.
An absolute contraindication to breast-conserving surgery includes extensive or diffusely distributed malignancy.
Calcified foci with extensive or diffusely distributed malignancy and difficulty in achieving negative margins or ideal profile; T4 stage breast cancer, including invasion of the skin, chest wall, and inflammatory breast cancer; tumors with positive margins after extensive local excision that are not guaranteed to have negative pathological margins after re-excision; breast cancer in pregnancy, where postoperative radiotherapy is not predicted to wait until delivery; and patients who refuse to undergo breast-conserving surgery. Relative contraindications include tumor diameter greater than 3 cm and active connective tissue disease involving the skin, especially scleroderma and lupus erythematosus.
Treatment of axillary lymph nodes is part of the standard surgery for invasive breast cancer. Its primary purpose is to understand the status of the axillary lymph nodes in order to determine staging and select the best treatment option.
-
Breast CancerSLNB:SLNBwith the advantages of less trauma and fewer complications associated with SLNBis the earliest lymphatic drainage of breast cancer and tumor metastasis1. =”font-family:Arial”>one (or several) lymph nodes were excised for biopsy to assess axillary lymph node status,NCCNBreast Cancer Clinical Practice Guidelines recommendSLNB for early stage breast cancer patients with negative clinical axillary lymph nodes as the axillary lymph node management as the preferred surgical approach. BeforeSLNBsurgery, anterior lymph node tracing is required, and currentlySLNBThe commonly used tracing methods are dye (patent blue, isosulfur blue, methylene blue and nanocarbon), nuclear, dye combined with nuclear and fluorescence tracing methods. The most widely used tracing method is the blue dye method combined with nucleotide method. SLNBtechnology can accurately stage the axillary lymph nodes of breast cancer, and for patients with no clear metastasis in the axillary lymph nodes on clinical examination, the SLNB technique can be performed. SLNBis able to perform accurate axillary lymph node staging for patients with clinical examination of axillary lymph nodes without definite metastasis, and axillary lymph node dissection can be waived for patients with negative lymph nodes to reduce complications such as upper limb edema; ifthe technique can be used for patients with lymph nodes with no lymph nodes. span>SLNBpositive, axillary lymph node dissection can be performed.
- style=”margin-left: 97pt”>
- Armpit lymph node dissection: indications for axillary lymph node dissection include.
①Patients with positive clinical axillary lymph nodes and metastases confirmed by puncture /surgical biopsy; ②Patients with positive anterior lymph nodes and Patients who do not meet the ACOSOG Z0011 inclusion criteria such as T3, patients with more than T3, patients with more than “font-family:Times New Roman”>2 positive sentinel lymph nodes and those requiring total mastectomy; (iii) recent inadequate axillary lymph node dissection; (iv) sentinel lymph node verification test; (v) SLNBfailure; ⑥SLNB finding of clinically suspicious lymph nodes; ⑦T4.
⑧ Inability to perform SLNB; ⑨ Axillary recurrence after SLNB.
Usually, axillary lymph node dissection should include the anterior border of the latissimus dorsi to the lateral border of the pectoralis minor (Level I), the lateral border of the pectoralis minor to the medial border of the pectoralis minor
(Level II) of all lymph nodes. Clearing the axillary lymph nodes requires more than 10 to ensure a true picture of the status of the axillary lymph nodes. Only when Level I to II metastases are evident or Level III (medial border of the pectoralis minor muscle to the entrance of the axillary vein) Total axillary lymph node dissection at levels I-III is required only when enlarged metastatic lymph nodes are detected.
Breast defects after modified radical breast cancer surgery and breast deformities after breast-conserving surgery require reconstructive and reconstructive surgery and have become an essential part of the complete treatment plan for breast cancer. Breast reconstruction improves the quality of life and psychological satisfaction of postoperative patients. The number of breast reconstructions in China is increasing year by year, the methods are becoming more sophisticated, and the concept and awareness of breast reconstruction is increasingly recognized and accepted by oncologic surgeons.
The oncologic safety of breast reconstruction is certain. Whether, when, and how breast reconstruction is performed does not affect the postoperative survival of patients with breast cancer and
Survival time. Breast reconstruction has no impact on surgery or the detection of tumor recurrence or metastasis.
Normally, breast reconstruction does not interfere with the delivery of postoperative chemotherapy. Unless more serious complications (e.g., infection, incisional dehiscence, etc.) occur after immediate reconstructive surgery, they do not significantly affect the clinical application of chemotherapy and treatment outcomes. Adjuvant chemotherapy after immediate breast reconstruction does not increase the incidence of post-reconstruction complications, does not decrease the success rate of immediate breast reconstruction, does not affect wound healing, and does not affect the outcome of reconstruction. However, neoadjuvant chemotherapy can increase the incidence of flap infection and necrosis after immediate breast reconstruction. Chemotherapy can cause a decrease in immune function and resistance to infection, making it inappropriate to perform any breast reconstruction surgery during chemotherapy.
Neither autologous tissue reconstruction nor prosthetic reconstruction is a contraindication to radiation therapy and does not significantly affect the outcome of radiation therapy. Immediate breast reconstruction increases the technical difficulty of postoperative radiotherapy field design, but a well-designed radiotherapy plan does not affect radiotherapy outcomes. Radiotherapy affects the long-term aesthetic satisfaction and overall satisfaction with the reconstruction.
The basic principles of breast cancer resection mastectomy reconstruction are as follows.
-
Tumor treatment must be a priority. Any reconstructive surgery for breast reconstruction should not delay adjuvant breast cancer treatment and should not interfere with adjuvant breast cancer treatment.
- Breast reconstruction must be included in the overall treatment plan for breast cancer, and the physician has an obligation to inform the patient of the option to undergo breast reconstruction.
- During mastectomy, the skin, subcutaneous tissue, and important aesthetic nodes of the breast should be preserved as much as possible without violating oncologic principles.
The skin, subcutaneous tissues, and important aesthetic structures of the breast (such as the inframammary fold) should be preserved as much as possible during mastectomy without violating oncologic principles, to maximize the conditions for breast reconstruction and to improve the aesthetic outcome of the reconstructed breast and patient satisfaction.
-
The treatment of breast cancer should be done in a multidisciplinary team framework, including radiology, breast surgery, plastic surgery, imaging, pathology, psychology, nuclear medicine, immunology, etc.
Preoperative examination, evaluation and education for breast reconstruction: The patient’s condition should be tested and evaluated before surgery, analyzing oncologic conditions, medical conditions, tissue conditions, contralateral breast conditions, etc., and combining these conditions to choose a surgical option that is less invasive, simpler, less costly, with a lower complication rate and good results.
Types and stages of breast cancer that contraindicate breast reconstruction: stage IV invasive breast cancer, recurrent metastatic breast cancer. Breast reconstruction is usually contraindicated during radiotherapy and within six months after radiotherapy. For patients who have undergone radiotherapy or are planning to undergo radiotherapy, the timing and surgical method of breast reconstruction should be carefully chosen. Severe obesity and smoking, severe medical disease, and peripheral vascular disease are important risk factors for postoperative complications and are relative contraindications to breast reconstruction.
Treatment cycle and cost: 1) Breast reconstruction is a sequential treatment that usually requires multiple procedures to achieve desired results. Breast reconstruction is performed using the tissue expansion method. Immediate breast reconstruction has advantages over second-stage breast reconstruction in terms of overall treatment time and cost.
Basic approaches to breast reconstruction: These include skin-covered reconstruction and breast volume reconstruction. The methods of skin-covered reconstruction include tissue expansion and autologous flap grafting, while the methods of breast volume reconstruction include the application of prosthesis, flap grafting, and free autologous fat grafting. Commonly used skin flaps for autologous tissue breast reconstruction include.
dorsalis muscle flap, rectus abdominis muscle flap, inferior abdominal wall artery perforator flap, etc. Follow-up time: Follow-up for breast reconstruction should begin after surgery and continue until after surgery.
5 years or more, with regular follow-ups depending on the type of breast reconstruction. Observation indicators: include oncologic follow-up of breast cancer, breast shape and symmetry, incisional scar, donor area function, prosthesis integrity, envelope contracture, and other complications. If necessary, psychological changes and quality of life changes should also be included. Examination items: oncologic examination, breast surface measurements, photography, donor area motor function measurement, breast prosthesis contracture grading, and special examinations such as ultrasound and MRI if necessary. The patient should be given detailed postoperative instructions after breast reconstruction, including daily precautions, exercise, oncologic examinations, and review schedules.
- style=”margin-left: 68pt”>
- Radiation therapy after breast-conserving surgery for early breast cancer
-
Indications: In principle, all patients undergoing breast-conserving surgery need to receive radiation therapy. In principle, all patients undergoing breast-conserving surgery need to receive radiation therapy. For patients aged >70years with breast tumors≤2cm, no lymph node metastasis,ER =”font-family:Arial”>positive female patients who can receive standard endocrine therapy may be considered for omission of post-breast-conserving radiotherapy.
- style=”margin-left: 71pt”>
- Range of irradiation.
- Range of irradiation.
-
In units where available, strictly selected low-risk patients can be considered for In units where available, partial breast irradiation can be considered for carefully selected low-risk patients, with specific patient selection criteria and treatment modalities described in “(c)1. span>5)Partial breast irradiation” section.
-
Axillary lymph node dissection orSLNBwithout lymph node metastasis, the scope of irradiation is the affected breast.
- style=”margin-left: 56pt”>
- Patients with positive anterior lymph nodes and no axillary lymph node dissection for
- Patients with positive anterior lymph nodes and no axillary lymph node dissection for
in T 1 to Invasive breast cancer with stage 2 and 1 to 2 positive anterior lymph nodes may be considered for whole breast high level tangential field radiotherapy (i.e. The upper border of the tangential field is within 2 cm below the head of the humerus), and if intensity-modulated radiotherapy (intensity-modulated (IMRT) technique, care should be taken to outline and irradiate the low and median axilla and the affected whole breast as an integrated target area; however, for post-breast-conserving patients who do not meet this criterion, irradiation is recommended to include The affected breast, supraclavicular and axillary lymph node drainage areas.
-
Undergoing axillary lymph node dissection with a positive lymph node count of < span style="font-family:Times New Roman">1 to 3 patients, in order to minimize the risk of recurrence, irradiation of the lymphatic drainage area is recommended in principle, and patients with low risk of recurrence can be selected to be exempted from lymphatic drainage area The lymphatic drainage area can be waived for patients with low risk of recurrence. The scope of irradiation includes the affected supraclavicular and infraclavicular regions, and the internal breast irradiation should be decided on an individual basis. Young, Hormone Receptor (Hormone Receptor, HR) Negative, extensive vascular thrombus, primary focus medially. span>/The overlap of risk factors such as central quadrant, and high grade histology may increase the importance of lymphatic drainage area irradiation.
-
Receiving axillary lymph node dissection with Patients with lymph node metastases≥4, the target area should include the affected breast, supraclavicular/inferior and internal breast lymphatic drainage areas (provided cardiopulmonary safety is ensured).
-
Endoluminal irradiation is currently controversial. It is recommended to consider internal breast irradiation for patients with the following conditions: ① ≥4 lymph node metastases after axillary lymph node dissection.
② Primary tumor located in the inner quadrant or central region with axillary lymph node metastasis; ③ Age <35 The use of modern precision radiotherapy techniques is recommended for accurate internal breast irradiation.
Evaluate the dose of irradiation to normal tissues, including the heart, while capturing the benefits and risks of systemic therapy and radiotherapy for cardiac-related injury and internal breast prophylaxis. The benefits and risks of irradiation should be fully communicated in a multidisciplinary manner if necessary, or patients should be encouraged to participate in clinical trials.
-
Patients with complete axillary clearance do not require prophylactic irradiation. Axillary radiotherapy may be used in patients with the following high-risk factors for axillary recurrence, but the risk of tumor recurrence needs to be weighed against the risk of increased lymphedema with radiotherapy. High-risk factors include: (i) incomplete axillary clearance, based on the patient’s preoperative axillary metastatic lymph node load, intraoperative lymph node adhesion to surrounding vessels and the thoroughness of surgical clearance, comprehensive assessment of axillary examination and imaging before radiotherapy to determine whether lymph nodes remain; (ii) extra-peripheral lymph node invasion; and (iii) a high number of axillary lymph node metastases with a high percentage of positivity.
④ Positive axillary lymph nodes and total number of axillary lymph nodes cleared <10 . However, it is important to distinguish whether the low total number of axillary lymph nodes is due to inadequate surgical debridement or inadequate pathology sampling, and to communicate with the surgeon and pathologist as necessary.
-
For patients receiving whole-breast radiotherapy, tumor bed make-up is recommended for patients who meet the following criteria: 1) Invasive breast cancer: age ≤50 years of age, any grade, or 51 years of age, any grade, or 51 years of age, any grade, or 51 years of age, any grade, or 51 years of age, any grade. years to 70 years, any level high grade, or positive cut edge; ②DCIS: age ≤
50 years, or high level, or tangential margin <2 mm, or a positive cut margin. Patients with a low risk of recurrence who meet the following criteria may be considered for no tumor bed replacement: ① Invasive breast cancer: age >70 years, hormone receptor positive, low to mid grade with adequate negative margins (margin ≥2 mm); ②DCIS: age >50 years, detected by screening, tumor size ≤2. 5 cm, low to intermediate grade, and adequate negative margins (margin ≥3 mm). For patients who do not meet these criteria, the physician can weigh the pros and cons (tumor control and cosmetic outcome) based on the patient’s condition and make a
Individualized decision making.
-
Irradiation techniques: Post-breast-conserving radiotherapy can be delivered by three-dimensional conformal radiotherapy, fixed-field, or rotational intensity modulation irradiation techniques. Regardless of the technique, it is recommended to use CT to locate and outline the target area, which willCTimages into the 3D treatment planning system for planning evaluation to accurately assess the dose distribution to the target area and the organs at risk. CTlocalization should be performed by using a lead wire to mark the outer contour of the affected breast and the surgical scar of the primary breast to facilitate the identification of the whole breast and the tumor bed for supplemental irradiation. The scope should be determined. Breath control techniques, such as deep inspiratory breath-holding and prone positioning, may further reduce the dose to normal organs, primarily the heart and lungs, and are recommended in units where available.
Compared with 2D radiotherapy, 3D conformal and intensity modulated irradiation can help improve dose uniformity within the target area, reduce the dose to normal tissue, and better manage the interface between the breast and regional lymph node fields, which is advantageous in large breast volumes where regional lymph node irradiation is required. It is more advantageous in cases of large breast volumes where regional lymph node irradiation is required, but increases the complexity of the plan design. It is recommended that the choice of irradiation technique be individualized based on the patient’s condition, extent of irradiation, and comorbidities.
Mammary tumor bed replacement volume can be achieved with intraoperative radiation therapy, interstitial tissue insertion, electron beam or extra X ray irradiation. The surgeon is recommended to place a titanium clip at the tumor margin to provide a reference for tumor bed replenishment.
-
Irradiation dose and segmentation pattern: the recommended dose for the whole breast ± regional lymph nodes is < /span>50Gy/2Gy/25f. External irradiation of the tumor bed can be sequenced after whole breast radiotherapy with a sequential dose of10to16Gy/2Gy/5~8f ; in experienced units, simultaneous bed-synchronous irradiation can be considered, such as bed-synchronous irradiation dose60Gy/2.4Gy/25f . For patients who have whole breast irradiation only, it is recommended that a large fraction may be given
Cutting radiotherapy40Gy/15f or 42.5Gy/16f; in experienced units, it is also possible to use 43.5Gy/15f/3w segmentation pattern. After external irradiation tumor bed replenishment sequential in whole breast large segmentation radiotherapy, conventional segmentation pattern 10 to 16Gy/2Gy/5~8f or large split mode 10~10~12.5Gy/4 to 5f; in experienced units, the large split sequential replenishment mode can also be used 10 to
In experienced units, a large split irradiation pattern can be considered for patients with whole-breast + regional lymph node irradiation at the same dose as whole-breast large split irradiation.
-
Partial breast irradiation: Several studies suggest that in patients with low-risk breast cancer after breast-conserving surgery Partial breast irradiation may have the same efficacy as whole breast irradiation in patients with low-risk post-breast-conserving breast cancer. Patients are currently encouraged to participate in clinical trials related to partial breast irradiation; in addition to clinical trials, patients receiving partial breast irradiation need to be carefully selected and carried out in an orderly manner at experienced medical centers, taking into account their own technical conditions and patients’ wishes, with the following recommended indications: ① Age ≥50 years old; ②invasive cancer tumor size ≤3 cm
(T1, small T2) with negative cut margins ≥ 2 mm; (iii) simple low –medium grade DCIS, screening findings, tumor size ≤ 2. 5 cm, negative cut-off margin ≥ 3 mm; ④ SLNB
or axillary lymph node dissection confirmed as N 0 ; ⑤ single central lesion; ⑥ no lymphovascular invasion; ⑦ no extensive intraductal cancer component; ⑧ not receiving neoadjuvant chemotherapy; and ⑨ preferably ER positive and excluding invasive lobular carcinoma (not required).
Partial breast irradiation can be performed by intraoperative radiotherapy, proximity insertion, or external irradiation. Irradiation covers the breast tumor bed. Recommended doses include intraoperative radiotherapy 20Gy in a single session and brachytherapy 34Gy/3.4Gy/10f, 2 times per day.
at least 6 intervals Roman”>6 hours, total treatment time 5 days, or other equivalent biosegmentation dose pattern; external irradiation 38.5Gy/10f, 2 times per day for 5 days to complete. The follow-up results of the RAPID study suggest that the late cosmetic results of external irradiation as a segmentation modality for partial breast radiotherapy are relatively poor, and considering the actual situation of the relative shortage of gas pedals in China, it is also possible to use 38.5Gy/10f per day 1 time or 40Gy/10f per day1 exposure pattern.
-
Indications: Post-operative adjuvant radiotherapy should be considered for patients after modified radical surgery if any of the following conditions are met: ①The largest diameter of the primary tumor (1) The largest diameter of the primary tumor>5cm, or the tumor invades the breast skin or chest wall. ② Axillary lymph node metastasis≥4, or the presence of supraclavicular or internal breast lymph node metastasis. (iii) Primary tumor stageT1to2and axillary lymph node metastasis1to3 patients are recommended to receive radiation therapy after modified radical surgery. However, for those without significant high-risk recurrence factors, i.e., age≥50 years, tumor grade I-II, absence of vascular aneurysm emboli, number of axillary lymph node metastases 1 and hormone receptor positive, radiotherapy may be considered to be omitted. ④For patients who received neoadjuvant chemotherapy before modified radical surgery, the indications for postoperative radiotherapy are described in the “III.1. Postoperative Radiotherapy After Neoadjuvant Chemotherapy” Chapter.
- style=”margin-left: 71pt”>
- Range of irradiation.
- Range of irradiation.
- Patients requiring modified post-radiation therapy after radical surgery should be irradiated to the chest wall and upper and lower clavicular regions.
-
Inner breast irradiation is controversial and is recommended for patients with the following conditions: 1) lymph node metastasis after axillary lymph node dissection ≥4 .
②The primary tumor is located in the inner quadrant or central region and accompanied by axillary lymph node metastasis; ③
age <35 years old and with axillary lymph node (4) Diagnosis of internal breast lymph node metastasis on imaging at the time of initial diagnosis or pathologically confirmed internal breast lymph node metastasis without internal breast lymph node dissection. The use of modern precision radiotherapy techniques is recommended for internal breast irradiation in order to accurately assess the dose to normal tissues such as the heart and to capture the benefits and risks of systemic therapy and radiotherapy for cardiac-related injury and internal breast prophylaxis, with adequate multidisciplinary communication if necessary, or to encourage patients to participate in clinical trials.
-
For patients with complete axillary lymph node dissection, the target area of radiotherapy is not recommended to include the affected axilla. For patients with lymph node metastases found afterSLNB but without axillary dissection or incomplete axillary dissection, the radiotherapy target area should be considered to include the axilla.
-
Irradiation techniques: Radiation therapy after modified radical surgery can be performed by two-dimensional irradiation, three-dimensional conformal radiotherapy, fixed field or rotational intensity modulation. irradiation techniques. Regardless of the technique, it is recommended to use CT to locate and outline the target area and the organs at risk, and to place CTimages into the 3D planning treatment system for individualized planning evaluation to accurately assess the dose distribution to the target area and organs at risk. Also, regardless of the irradiation technique, care should be taken to add tissue compensators on the chest wall surface (40%~60%irradiation dose) to ensure adequate skin dose.
The irradiation field can be designed by referring to the traditional two-dimensional irradiation, e.g., single anterior field or anterior-posterior pair of fields can be used for supraclavicular irradiation, and electron beam field can be used for irradiation in the internal mammary lymphatic drainage area, but the supraclavicular and internal mammary areas are required 90% of the target volume should be irradiated at 90% of the dose. The chest wall can be irradiated with either tangential or electron beam fields, and when electron beam irradiation is used, the extent of irradiation can be based on the traditional two-dimensional distribution of the field, including the full surgical scar and free flap range.
Compared with 2D radiotherapy, 3D conformal and intensity-modulated radiotherapy helps to ensure that the target area
To achieve the prescribed dose, improve dose uniformity within the target area, reduce the irradiated dose to normal tissues, better manage the interface between chest wall and regional lymph node irradiation fields, and individualize patient treatment, but increase the complexity of plan design. Individualized selection of irradiation technique is recommended based on the patient’s condition, irradiation range and comorbidities. When using conformal intensity modulated radiotherapy, the target area should be accurately outlined to ensure cardiopulmonary safety without significantly increasing the dose to other normal organs, such as the thyroid, healthy breast, and affected shoulder joint.
-
Irradiation dose and segmentation pattern: the recommended dose after modified radical surgery is50Gy/2Gy/25f. In experienced units, large split radiotherapy may be considered40to~43.5Gy/15f/3w.
-
Radiotherapy with systemic therapy If adjuvant chemotherapy is indicated, postoperative radiation therapy should be administered after completion of adjuvant chemotherapy; if no adjuvant chemotherapy is indicated, postoperative8week to start radiation therapy. Adjuvant Herceptin therapy can be started at the same time as postoperative radiation therapy. Before starting radiation therapy, it is important to confirm the left ventricular ejection fraction (left ventricular ejection fraction, LVEF) is greater than50%, while keeping the irradiation dose to the heart as low as possible, especially if the affected side is left-sided. Adjuvant endocrine therapy can be performed concurrently with postoperative radiation therapy.
- style=”margin-left: 44pt”>
-
- Postoperative radiation therapy after neoadjuvant chemotherapy.
- Postoperative radiation therapy after neoadjuvant chemotherapy.
-
-
Neoadjuvant Post-chemotherapy breast-conserving radiotherapy: For patients undergoing breast-conserving surgery after neoadjuvant chemotherapy reduction, post-operative whole-breast+Tumor bed supplemental radiation therapy. The tumor bed target area is generally based on breast conservation after neoadjuvant chemotherapy
The actual extent of surgical excision is determined, and if necessary, reference should also be made to Pre-chemotherapy clinical staging and post-operative pathological staging are determined (the key is the accurate assessment of primary tumor regression and modality prior to surgery, as well as the guarantee of negative margins). All patients with positive postoperative pathological lymph nodes or patients with initial stage III clinical staging prior to neoadjuvant chemotherapy should be routinely irradiated postoperatively with a combined whole breast lymphatic drainage area. For patients with positive regional lymph nodes in initial stage II cN 1 stage, post-operative whole breast combined lymphatic drainage area irradiation is routinely performed after neoadjuvant chemotherapy in patients with ypN 0 stage. In principle, postoperative whole-breast combined lymphatic drainage area irradiation is still required; in clinical practice, some low-risk patients can also be selected for careful individualized exemption from lymphatic drainage area irradiation, such as those who have reached pCR after neoadjuvant chemotherapy for both primary and axillary lymph nodes, and those who are age >40 years of age, and no comorbid associated pathologic risk factors (e.g., histologic grade 3 , vascular carcinoma emboli, hormone receptor negative, etc.).
The dose of prophylactic radiotherapy after neoadjuvant chemotherapy followed by breast-conserving surgery is referenced to the no neoadjuvant chemotherapy scenario described previously.
-
Radiotherapy after modified radical surgery after neoadjuvant chemotherapy: No phase III randomized controlled clinical trial is available for adjuvant radiotherapy decisions after neoadjuvant chemotherapy. The results of phase III randomized controlled clinical trials are not available, but the current recommendation is to combine the patient’s clinical stage before neoadjuvant therapy and pathological stage after neoadjuvant chemotherapy with patient and tumor characteristics to make radiotherapy decisions. The indications for radiotherapy are as follows: (1) patients with initial stage III before neoadjuvant chemotherapy and positive axillary lymph nodes after neoadjuvant are recommended for postoperative radiotherapy; (2) patients with initial clinical stage II
(cN 1 stage) with negative postoperative pathological axillary lymph nodes after neoadjuvant chemotherapy, and whether to perform postoperative radiotherapy is controversial, and patients are encouraged to to participate in clinical studies. Patients with high-risk factors can be selected clinically for postoperative radiotherapy: age ≤ 40 years, ypT>2 cm, Vascular aneurysm peg-positive, poor prognosis molecular subtype (hormone receptor negative, HER2
positive and not on targeted therapy), etc.
The scope, dose, and fractionation pattern of radiation therapy after neoadjuvant chemotherapy are essentially the same as those of radiation therapy after modified radical surgery without neoadjuvant therapy. The need for postoperative radiotherapy after neoadjuvant chemotherapy for initially diagnosed locally advanced breast cancer (Locally Advanced Breast Cancer, LABC) is noted that significant skin invasion or diagnosis of inflammatory breast cancer = “font-family:Times New Roman”>LABC, consider irradiating the entire chest wall at 50 Gy min25 times followed by a top-up dose of 10 to 16 Gy to the chest wall in the free flap range; the number of skin surface fillers may be increased during radiotherapy to ensure adequate skin dose. Patients with supraclavicular or internal mammary lymph node metastasis at initial diagnosis should be irradiated with additional dose at the original supraclavicular or internal mammary lymph node metastasis site after local area prophylaxis irradiation. If complete remission of supraclavicular or internal mammary lymph nodes is achieved after chemotherapy, an additional dose of 10 Gy in 5 doses; if supraclavicular or internal mammary lymph nodes remain in remission after chemotherapy If residual supraclavicular or internal breast lymph nodes remain after chemotherapy, add 16-20Gyminutes8-10 doses. Patients were asked to undergo CT at the time of initial baseline evaluation to identify the initial lymph node metastasis site and puncture to clarify the pathologic diagnosis for subsequent radiotherapy to determine the extent of supplemental irradiation.
-
Radiotherapy after breast reconstruction: The indications for radiotherapy in patients with breast reconstruction after total mastectomy are the same as in patients with the same staging and no reconstruction. The radiotherapy indications are the same as for patients with the same staging and no reconstruction, but the risk of radiotherapy complications with reconstructive implants and the technical challenges of reconstruction need to be additionally weighed in the decision-making process. Autologous reconstructed tissue tolerates radiotherapy well, and radiotherapy does not increase the risk of complications in patients with autologous reconstruction. Because of the potential for atrophy of the autologous implant tissue after radiation therapy, it is possible to design the reconstructed breast volume slightly larger than the contralateral breast at the time of surgery. The use of prosthetic reconstruction is increasing each year, and radiotherapy increases the risk of implant contracture and reduces cosmetic outcomes. In staged reconstruction, radiotherapy interventions when
The machine can be before or after permanent prosthesis implantation. Radiotherapy prior to permanent prosthesis placement, with direct irradiation of the tissue expander, has little effect on subsequent prosthetic contracture, but has an increased rate of reconstruction failure. Radiotherapy after permanent prosthesis implantation has a low reconstruction failure rate but an increased complication of periosteal contracture. In addition, the timing of radiotherapy intervention needs to take into account the effect of delayed radiotherapy on tumor outcome due to permanent prosthesis implantation, and it is best not to delay radiotherapy too long for patients at high risk of recurrence. For patients treated with radiotherapy prior to permanent prosthesis implantation, to improve the success rate of reconstruction, the dilator injection procedure should be completed prior to radiotherapy positioning to ensure adequate tissue expansion, and saline should not be injected or withdrawn from the dilator until the end of radiotherapy to ensure consistent volume and location of the target area. Radiation therapy requires irradiation of the ipsilateral chest wall + regional lymphatic drainage area, which is irradiated according to the same principles as in patients without reconstruction. The dose of radiation therapy was conventional divided 50 Gy in 25 sessions, 5 weeks. Conventional radical surgery will leave 5% to 10% of the glands remaining, and the rich network of lymphatic vessels within the subcutaneous tissue is an important pathway for tumor metastasis to the axillary or internal breast lymph nodes, all of which are important targets for post-reconstructive chest wall radiotherapy. Because of the superficial location, part of the target area is located in the dose built-up area, special attention is paid when designing the radiotherapy plan to irradiate the whole target area in the presence of positional error. Depending on the extent of the built-up area of the radiotherapy technique used, it is recommended to irradiate 10 to 15 times on the surface of the chest wall skin pad with tissue filler to ensure adequate dose to the target area.
- Radiotherapy after local area recurrence: chest wall and supraclavicular lymphatic drainage areas are the most common sites of recurrence after radical or modified radical breast cancer surgery. A single recurrence in the chest wall is in principle treated with radiation after surgical resection of the tumor; if surgery is not possible, radiation therapy should be administered first. For patients who have not had prior radiation therapy, radiation therapy should cover the entire chest wall and the supraclavicular/subclavicular area. Supraclavicular recurrence
Patients who have not had prior postoperative radiation therapy need to be irradiated to include the entire chest wall and supraclavicular lymphatic drainage area on the affected side. If there is no recurrence of axillary or internal mammary lymph nodes, prophylactic irradiation of the axillary and internal mammary areas is not necessary. The dose for prophylaxis is DT 45 to 50 Gy/25f/5w >, recurrence site shrinkage of wilderness supplementation to DT 60 to 66Gy/30 to
33f/6 ~ 6.5w. In patients with recurrent tumors treated with prior radiation therapy, the decision to proceed with recurrent radiation therapy is based on the interval between tumor recurrence, the dose range and degree of adverse effects of the first course of radiation therapy, and the likely efficacy and adverse effects of recurrent radiation therapy. In the case of recurrent radiation therapy, only the recurrent tumor site is irradiated, and extensive prophylactic irradiation is not recommended.
Patients with locoregional recurrence require a cytologic or histologic diagnosis of the recurrence site before treatment.
To assess the patient’s basic condition (age, menstrual status, blood count, vital organ function, presence of other diseases, etc.), tumor characteristics (pathological type, differentiation, lymph node status, HER2 and hormone receptor status, presence of vascular aneurysm emboli, etc.), and treatment (e.g., chemotherapy, endocrine therapy, targeted drug therapy, etc.) are analyzed comprehensively, and physicians select the appropriate treatment based on treatment tolerability, risk of postoperative recurrence, tumor molecular typing, and treatment sensitivity, weighing the risks that treatment poses to patients – benefit, and if the benefit is likely to outweigh the risk for patients receiving chemotherapy, postoperative adjuvant chemotherapy may be administered. See Appendix 8 for stratification of risk of postoperative recurrence of breast cancer; see Appendix 9 for determination of molecular staging of breast cancer.
- Indications: ①positive axillary lymph nodes. ②Low number of metastases to lymph nodes (1to3 postmenopausal patients who have receptor-positive,HER2
negative, small tumor, tumor grade I, and several other prognostic factors, or if the patient is intolerant or unsuitable for chemotherapy, may also be considered for endocrine therapy alone.
③ For lymph node negative breast cancer, postoperative adjuvant chemotherapy is only indicated for those patients with high risk factors for recurrence (patients <35 years, tumor diameter >2cm, tumor grade II-III, vascular tumor emboli, HER2positive, ER/PR negative, etc.).
-
Relative contraindications: ①Pregnancy: Chemotherapy is usually contraindicated in patients in early pregnancy and should be chosen with caution in patients in mid-pregnancy. ②Obvious failure or cachexia.
③Patients who refuse postoperative adjuvant chemotherapy. ④Patients with severe infection, hyperthermia, water-electrolyte and acid-base balance imbalance. ⑤ Patients with gastrointestinal obstruction or perforation. ⑥Low bone marrow reserve function with pre-treatment leukocytes ≤ 3.5×109/L, platelets ≤80×109/L person. (7) Those with impaired cardiovascular, hepatic or renal function.
- Selection of adjuvant chemotherapy regimens: commonly used adjuvant chemotherapy regimens are listed in the Appendix10).
-
Commonly used regimens: 1) Anthracycline-based regimens, such asAC(doxorubicin) style=”font-family:Arial”>cyclophosphamide),EC(epirubicin) /cyclophosphamide). Although pirarubicin
(THP) has limited evidence-based medical evidence, it is feasible to replace doxorubicin with piroplicin in our clinical practice,and family:Times New Roman”>THP at a recommended dose of 40-50 mg/m2.
②A combination regimen of anthracyclines and paclitaxel, such as TAC (T: docetaxel).
③A sequential regimen of anthracyclines and paclitaxel, such as AC→paclitaxel (1 time per week), < span style="font-family:Times New Roman">AC→docetaxel (every 3 weeks), 1 dose), dose-intensive AC renewal paclitaxel (every 2weekly1), dose-intensiveAC renewal paclitaxel (weekly1 time). ④Anthracycline-free combination chemotherapy regimens: TC regimens (docetaxel /cyclophosphamide = “font-family:Times New Roman”>4 or 6 courses) for patients with some risk of relapse. ⑤ Capecitabine’s strong
chemotherapy (combined or sequential) may be considered in triple-negative breast cancer.
- HER2positive breast cancer: commonly used See the appropriate section in the Adjuvant AntiHER2Targeted Therapy after Breast Cancer section for options.
-
Caution: 1) The goal of adjuvant chemotherapy for early-stage breast cancer is to achieve cure. The goal of adjuvant chemotherapy in early stage breast cancer is to strive for cure, so standard and standardized chemotherapy is emphasized. The order of administration, infusion time and dose intensity of chemotherapeutic drugs should be noted during chemotherapy and used in strict accordance with drug instructions and contraindications. ③Select chemotherapy regimens according to the patient’s risk of relapse, tolerance level, patient’s wishes and evidence-based medical evidence, and develop support programs to prevent vomiting and bone marrow suppression. ④The number of cycles of different chemotherapy regimens varies, generally being 4to~8 cycles. If there are no special circumstances, it is not recommended to reduce the number of cycles and dose. Patients older than 70 years need to consider adjuvant chemotherapy on an individual basis. ⑤ Adjuvant chemotherapy is generally not administered concurrently with endocrine therapy or radiotherapy, and endocrine therapy is started after chemotherapy is completed; radiotherapy and endocrine therapy may be administered sequentially or concurrently. (6) Generally, the recommended first dose should be administered at the recommended dose, but if there are special circumstances that require adjustment, it should usually be no less than 85% of the recommended dose. The subsequent dose should be adjusted downwardonce according to the patient’s specific condition and the adverse effects after the initial treatment20% to25 The rate of treatment with adjuvant chemotherapy is >%. Only 2dose reductions per adjuvant chemotherapy regimen are generally allowed. (7) For premenopausal patients who are hormone receptor negative, ovarian function suppressants may be considered to protect ovarian function during adjuvant chemotherapy. It is recommended to use ovarian function suppressants before chemotherapy1to21times before chemotherapy. Roman”>2weeks of dosing, and after the end of chemotherapy2weeks of dosing, and after the end of chemotherapy2weeks of dosing, and after the end of chemotherapy family:Arial”>week after administration of the last dose of the drug. (8) Anthracyclines are cardiotoxic and should be evaluated at the time of useLVEF, generally every3months1times. ⑨ All chemotherapy patients are required to sign an informed consent form for chemotherapy first.
Neoadjuvant chemotherapy is systemic chemotherapy administered first before surgery or surgery plus local radiation therapy in order to reduce the clinical stage of the tumor and improve the resection and breast conservation rates.
- Indications: 1) inoperable downgrade to operable, clinical stage IIIA(excludingT3, N1, M0), IIIB, III, IIIC. (ii) Patients expecting descending breast conservation with clinical stage IIA, II, IIB, IIIA(onlyT3,N1,M0) stages that meet the indications for breast-conserving surgery other than tumor size. Neoadjuvant therapy may also be considered for patients who wish to reduce the size of the mass and preserve breast at a reduced stage. ③ Neoadjuvant therapy is feasible for inoperable occult breast cancer (where occult breast cancer is defined as breast cancer in which axillary lymph node metastasis is the first symptom and no primary site can be found in the breast).
-
Contraindications: 1) Undiagnosed histopathologically confirmed Breast cancer: recommended Histopathological diagnosis with ER, , , , , . family:Times New Roman”>PR, HER2, HER2 =”font-family:Arial”>andKi-67and other immunohistochemical indicators, cytology is not recommended as pathological diagnostic criteria. ②Women in early pregnancy are absolutely contraindicated: while female patients in mid- and late-pregnancy should carefully select neoadjuvant chemotherapy as a relative contraindication, which has been successfully applied in case reports abroad. ③Those with significant cardiovascular, hepatic or renal impairment. ④The primary tumor is an extensive in situ cancer component, and caution should be used for those who cannot clearly identify the presence of infiltrating cancer. ⑤ Tumors that are not clinically accessible or cannot be evaluated. ⑥Patients who refuse preoperative neoadjuvant therapy. (7) Patients with severe infection, hyperthermia, water-electrolyte and acid-base balance disorders. ⑧Insufficient bone marrow reserve with pre-treatment neutrophils ≤1.5××109/ L, platelets ≤75×10< span style="font-size:10pt">9/Lers.
- style=”margin-left: 71pt”>
- Selection of neoadjuvant chemotherapy regimens.
①For HR-positive/HER2-negative breast cancer Patients with needs such as downstaging or breast conservation are recommended for priority adjuvant chemotherapy advancement to the neoadjuvant phase.
- Selection of neoadjuvant chemotherapy regimens.
② For HER2-positive and triple-negative breast cancer patients For patients with HER2-positive and triple-negative breast cancer, the indications for neoadjuvant therapy can be relaxed, the efficacy of treatment can be evaluated early by neoadjuvant therapy, and ascending/ descending adjuvant therapy can be established by whether the pathology is in complete remission after surgery.
③ For HER2-positive breast cancer patients who meet the neoadjuvant indication, an anthracycline-containing regimen in combination with paclitaxel or a non-anthracycline regimen in combination with trastuzumab should be used
±Pattuzumab for neoadjuvant therapy. The addition of patuximab further improves pCR rates, with more benefit in HR-negative, lymph node-positive patients.
④ For patients with triple-negative breast cancer, conventional regimens containing anthracyclines and paclitaxel are recommended for neoadjuvant. Platinum can be used as part of neoadjuvant regimens for triple-negative patients to increase the probability of tumor regression and pCR, but the decision to add platinum should be weighed against the potential benefit versus harm, as it may not translate into future benefit of DFS. A BRCA1/2 pathogenic or suspected pathogenic mutation alone is not sufficient to justify the choice of platinum-containing therapy. For patients with underlying cardiac disease, neoadjuvant therapy with paclitaxel + platinum alone may be considered. PD-1/PD-L1 antibodies have not yet been licensed in China, and long-term toxicity and benefit are unknown, so adding immune checkpoint inhibitors to neoadjuvant therapy is not routinely recommended in this patient population.
-
Precautions: ①Histologic diagnosis and immunohistochemistry must be confirmed by hollow-core needle biopsy of the primary breast lesion before chemotherapy, and cytologic diagnosis can be used for regional lymph node metastasis. The neoadjuvant chemotherapy should be administered after a clear pathological histological diagnosis.
③Neoadjuvant chemotherapy is not recommended for stage I patients. ④In patients with treatment response or stable disease, it is recommended that all established cycle numbers be used before surgery. ⑤ Physical examination and imaging 2 aspects should be evaluated for breast primary and axillary lymph node metastases Efficacy should be evaluated according to the solid tumor efficacy assessment criteria RECIST or WHO criteria for evaluation
Efficacy. (6) If ineffective, suspend this chemotherapy regimen and switch to surgery, radiation therapy, or other systemic therapeutic measures (change chemotherapy regimen or switch to neoadjuvant endocrine therapy). (7) After neoadjuvant chemotherapy, even if the tumor disappears clinically, the patient must undergo the established follow-up surgery, depending on the individual case, either radical breast cancer surgery, modified radical breast cancer surgery or breast preservation surgery. (8) Postoperative adjuvant chemotherapy should be based on the cycle of preoperative neoadjuvant chemotherapy, its efficacy and postoperative pathological findings. The need for adjuvant radiotherapy and the extent of radiotherapy is recommended based on the clinical stage of the tumor prior to chemotherapy.
-
Systemic management: for neoadjuvant chemotherapy not achieving pCR (who have completed a full course of neoadjuvant therapy), especially in patients with triple-negative breast cancer, additional postoperative6to8 courses of Capecitabine therapy; HER2positive patients, priority is given to T-DM1intensive adjuvant therapy, or by continuing to complete trastuzumab in combination with patuximab co1year. Regardless of whether the pCR is achieved, some studies have shown that extended treatment with neratinib in specific populations “font-family:Times New Roman”>1year may further reduce the risk of relapse. For HRpositive patients, endocrine therapy is required. The need for endocrine therapy intensification and the manner of intensification can be assessed mainly based on the patient’s pre-neoadjuvant status.
The main goal of treatment for advanced breast cancer is not to cure patients, but to improve their quality of life and prolong their survival. The treatment is based on chemotherapy and endocrine therapy, with other treatment modalities such as surgery or radiation therapy considered when necessary. The patient’s primary tumor characteristics, previous treatment, disease-free survival, metastatic site, rate of progression, patient status, and other factors should be taken into account to choose the right treatment for the right time and for the right person.
Appropriate combination therapy and individualized drug use.
Staging evaluation of breast cancer patients with metastatic or recurrent presentation includes history, physical examination, laboratory tests, chest Xray or Xray or Xray. “font-family:Times New Roman”>CT, abdominal ultrasound, and bone imaging. Radiological examination of bone in patients with pain or abnormal bone imaging may also be considered with diagnostic abdominal CT or MRI, cranial CT or MRI. Evaluation of patients with PET-CT is not usually recommended, but PET-CT is optional when other findings are inconclusive or suspicious. span>is optional. Biopsy of metastases or first recurrence should be performed as part of the evaluation of the disease in patients with advanced breast cancer, along with detection of ER, PR, HER2, Ki-67, and other molecular markers to develop targeted treatment plans.
-
Patients who meet one of the following criteria may be considered for chemotherapy:< span style="font-family:Times New Roman">ER/PRnegative or low expression. (ii) Visceral crisis or symptomatic visceral metastases. ③ER/PR positive endocrine therapy resistant individuals (especially primary resistance).
-
Chemotherapeutic agents and regimens: see attached document for common chemotherapy regimens for advanced breast cancer. style=”font-family:Times New Roman”>11.
Commonly used chemotherapeutic agents for advanced breast cancer include anthracyclines, paclitaxel, vincristine, capecitabine, gemcitabine, platinum, and others. Individualized chemotherapy regimens should be developed based on the extent of the disease, molecular characteristics of the tumor, previous treatment and patient characteristics. The regimen should be developed with full consideration of the patient’s wishes, the incurability of the disease, and balancing quality of life and survival. The choice of single-agent or combination chemotherapy is reasonable at different stages of disease progression.
-
Single-agent chemotherapy: For patients with relatively slow tumor progression, low tumor load, no obvious symptoms, especially those who are poorly tolerated by the elderly Single-agent chemotherapy is preferred. Failure of anthracycline (paclitaxel) therapy is commonly defined as failure to treat with anthracycline (paclitaxel).
The anthracyclines (paclitaxel) relieve disease progression during chemotherapy, or after the end of adjuvant therapy recurrence of metastasis within 12 months. For patients who have failed prior anthracycline therapy, a single-agent or combination regimen based on paclitaxel (e.g., paclitaxel, docetaxel, and albumin-bound paclitaxel) is usually preferred; for patients who have failed both prior anthracycline and paclitaxel therapy, there is no standard chemotherapy regimen and other single-agent or combination regimens may be considered.
Commonly used single agents include: anthracyclines, such as doxorubicin, epirubicin, pirarubicin, and polyethylene glycolated liposomal doxorubicin; paclitaxel, such as paclitaxel, docetaxel, and albumin-bound paclitaxel; antimetabolites, such as capecitabine and gemcitabine The non-paclitaxel microtubule formation inhibitors, such as vincristine, eribulin, and euthyroxine; etoposide capsules and cyclophosphamide tablets, which are convenient to take orally, can be used as a backline treatment option.
-
Combination chemotherapy: suitable for patients with rapid disease progression, high tumor load or significant symptoms. The choice of combination chemotherapy regimens is varied and is based on previous evidence of evidence-based medicine, the interaction between combination drugs, the toxicity profile of the combination drugs, and the individual status of the patient.
1) For triple-negative breast cancer, the GP regimen (gemcitabine in combination with cisplatin), GC regimen (gemcitabine in combination with carboplatin), AP regimen (albumin paclitaxel in combination with cisplatin/ carboplatin), PC regimens (other paclitaxel drugs combined with carboplatin /cisplatin).
②Targeted therapy can be combined with either single agent or combination chemotherapy supported by evidence-based evidence. ③When combining chemotherapy, whether to use a continuous approach or to discontinue or maintain therapy after 4 to 8 courses needs to be weighed against efficacy, drug adverse effects, and patient quality of life. ④ For multiple courses of
There is no standard treatment for patients who have failed chemotherapy, and patients are encouraged to participate in clinical trials of new drugs or symptomatic supportive care. For triple-negative breast cancer, sacituzumab govitecan is an important targeted therapy option that has received US FDA approval, but clinical studies are yet to be conducted in China. ⑤ In HER2-positive patients, chemotherapy should be combined with anti-HER2-targeted drugs.
-
Maintenance chemotherapy: for patients who have completed4to6cycles of chemotherapy that are effective and well tolerated can be continued until progression or intolerable toxicity occurs. Those who have effective combination chemotherapy but cannot tolerate or do not want to continue combination chemotherapy can be considered for maintenance therapy, and can choose one of the original combination regimens for single-agent chemotherapy maintenance, and endocrine±targeted therapy maintenance can also be considered for hormone receptor-positive patients. Patient management should be enhanced during maintenance therapy, with regular assessment of efficacy and adverse effects.
- style=”margin-left: 44pt”>
-
- Indications.
- Indications.
-
-
Hormone receptors ERand//orPRpositive invasive breast cancer patients should receive postoperative adjuvant endocrine therapy. According to the latestASCO/CAPguidelines, althoughERimmunohistochemical staining for 1%< span style="font-family:Arial">to100%of the tumors were considered. span>ERpositive, butERpositive, butERpositive. Roman”>ERimmunohistochemical staining was 1%~10%forforERlow expression. The biological behavior of ERlow expression is usually associated withERnegative breast cancer, with less benefit in postoperative adjuvant endocrine, which should also be taken into account when making treatment decisions.
- style=”margin-left: 55pt”>
- Patients with carcinoma in situ who present with the following conditions may be considered for5years of endocrine therapy if.
①Patients requiring radiotherapy after breast-conserving surgery, especially those with positive hormone receptors among them
DCIS; (ii) patients who underwent only local excision of DCIS; (iii) patients who underwent total mastectomy with
- Patients with carcinoma in situ who present with the following conditions may be considered for5years of endocrine therapy if.
for the prevention of contralateral breast cancer.
-
Contraindications: ①Patients with contraindications to the use of endocrine drugs: history of deep venous thrombosis or pulmonary embolism. (2) Use with caution in patients with severe hepatic or renal impairment. (3) Pregnant women and those with previous allergies to endocrine therapeutic agents.
-
Drug selection: ① Adjuvant endocrine therapy in premenopausal patients The first choice is tamoxifen. ②For premenopausal patients with moderate to high risk of recurrence (age, mass size, lymph node status, histological grading, Ki-67proliferation index, etc., see “Expert Consensus on the Clinical Application of Ovarian Function Suppression in Early Stage Breast Cancer in China (2018Year Edition)”) Ovarian suppressants are recommended for use in adjuvant endocrine therapy. For younger (<35year-old) breast cancer patients, ovarian function inhibition plus aromatase inhibitors is more recommended. Tamoxifen or aromatase inhibitors plus ovariectomy or ovarian suppression for 5years. (iii) During tamoxifen treatment, patients may switch to an aromatase inhibitor if they are menopausal. ④Postmenopausal patients are preferred to third-generation aromatase inhibitors, which are recommended for initiation. ⑤Postmenopausal patients who cannot tolerate aromatase inhibitors may still choose tamoxifen.
- style=”margin-left: 71pt”>
- Caution.
- Caution.
- Patients should have their hormone levels measured prior to chemotherapy to determine menstrual status, with menopause defined in the Appendix12.
- The treatment duration of postoperative adjuvant endocrine therapy is5years, prolonged endocrine therapy needs to be individualized according to the patient’s situation and requires a combination of high risk factors for tumor recurrence and the patient’s wishes; for high-risk premenopausal patients, if tamoxifen treatment is completed 5years after tamoxifen treatment, the dose can be increased to10years, and if the patient becomes menopausal during the course of treatment, extended aromatization may be considered
enzyme inhibitor therapy until completion of 10 years of endocrine therapy.
-
Adjuvant endocrine therapy (except luteinizing hormone-releasing hormone agonists) is not recommended in conjunction with adjuvant chemotherapy, but is generally used after chemotherapy. Used after chemotherapy, can be used in conjunction with radiotherapy and trastuzumab therapy
- style=”margin-left: 55pt”>
- ERandPRnegative patients are not recommended for adjuvant endocrine therapy.
- ERandPRnegative patients are not recommended for adjuvant endocrine therapy.
-
Endocrine therapy in Monitoring and management of common adverse reactions: ① Contraception should be observed during tamoxifen administration and endometrial ultrasound monitoring is required every6days. 12months for 11months for Roman”>1time gynecologic examination. Bone density monitoring and calcium and vitamin D supplementation should be performed in patients on aromatase inhibitors. Formal anti-osteoporosis therapy is available for patients with severe osteoporosis. (iii) Patients should be monitored for lipids while on aromatase inhibitor therapy, and if necessary, patients with dyslipidemia should be treated accordingly. Serious adverse reactions to endocrine therapy require consideration of discontinuation or change of treatment regimen.
- style=”margin-left: 44pt”>
-
- Indications for preferred endocrine therapy: ①Patients older than35 years old.
- Indications for preferred endocrine therapy: ①Patients older than35 years old.
②Disease free survival >2 years (in combination with some targeted agents, this threshold can be exceeded as appropriate). (This threshold may be exceeded when combined with some targeted agents). (iii) Bone and soft tissue metastases only. (iv) Asymptomatic visceral metastases. ⑤ ER and / or PR positive. (6) Endocrine therapy can also be tried in patients with unknown receptors or negative receptors, if the clinical course is slowly progressing.
- style=”margin-left: 71pt”>
- Drug selection.
-
-
Recommendations for endocrine therapy in postmenopausal patients. Aromatase inhibitors include nonsteroids (anastrozole and letrozole), steroids (exemestane),ERmodulators (tamoxifen and toremifene), ERdownregulators (fulvestrant), pregnancy
Ketones (megestrol), androgens (fluoxymesterone), and high-dose estrogens (ethinyl estradiol).
-
Recommended endocrine therapy for premenopausal patients: based on suppression of ovarian function (mainly use of luteinizing hormone-releasing hormone agonists and surgical debulking), which can be treated with reference to postmenopausal breast cancer. If ovarian suppression is not performed, consider ERmodulators (tamoxifen and toremifene), progesterone analogs (megestrol), androgens (fluoxymesterolone), and high-dose endocrine therapy. Fluoxymesterone) and high-dose estrogens (ethinyl estradiol).
-
Both premenopausal and postmenopausal patients can be considered for targeted therapy in combination with endocrine therapy (). CDK4/6inhibitors, HDACHDACinhibitors, etc.).
- style=”margin-left: 71pt”>
- Options for first-line endocrine therapy in advanced breast cancer.
- Options for first-line endocrine therapy in advanced breast cancer.
- Aromatase inhibitors in combination withCDK4/6inhibitors (piperacillin, abecedrine) areHRpositive/HER2negative postmenopausal (spontaneous menopause or surgical debulking) or premenopausal but post-drug debulking breast cancer patients first-line endocrine therapy is preferred.
-
WhenCDK4/6inhibitors are not available, monotherapy with endocrine therapy is also feasible; postmenopausal (spontaneous menopause or surgical debulking) patients can be treated with fulvestrant, aromatase inhibitors (Aromatase Inhibitor, AI ), estrogen receptor
(Estrogen Receptor, ER) modulators (tamoxifen and toremifene) In premenopausal patients, ovarian function suppression (Ovarian Function Suppression, OFS) in combination with fulvestrant, OFS combined with AI, OFS combined with ER modulators, and simple ERmodulators.
- Premenopausal patients can be managed according to the postmenopausal model after the use of ovarian function inhibitors.
-
Options for second-line endocrine therapy in advanced breast cancer: after failure of first-line endocrine therapy After failure of first-line endocrine therapy, second-line endocrine therapy ± targeted therapy is still an option for patients with non-invasive crisis. Repeated use of adjuvant therapy or endocrine agents that have been shown to be resistant to first-line therapy is not recommended.
-
For patients who have not used< span style="font-family:Times New Roman">CDK4/6inhibitors: ①Fulvestrant in combination withCDK4/6inhibitors (piperacillin, abecedrine) areHR< span style="font-family:Arial">positive/HER2 negative postmenopausal (natural menopause or surgical debulking) or pre-menopausal but post-drug debulking breast cancer patients as a preference for second-line endocrine therapy. ② Steroidal/non-steroidal aromatase inhibitors (±OFS) or tamoxifen (±OFS) in combination withCDK4/6 inhibitors may also be used. For patients who have already used CDK4/6inhibitors, there is not sufficient evidence to support style=”font-family:Times New Roman”>CDK4/6inhibitors across lines of therapy.
-
When the above combination of small molecule-targeted single-agent endocrine therapy is also feasible; postmenopausal (spontaneous menopause or surgical debulking) patients can be treated with fulvestrant,AI, , and . , ERmodulators (tamoxifen and toremifene); premenopausal patients may useOFSin combination with fulvestrant,OFS >UnitedAI,< span style="font-family:Times New Roman">OFSUnitedER< modulators, simpleER Modifiers.
(3) Caution: 1) Tumor progression after two consecutive lines of endocrine therapy is usually indicative of endocrine therapy resistance. The tumor should be switched to cytotoxic therapy or entered into a clinical trial study. (2) During endocrine therapy, tumor progression should be evaluated every 2 to 3 months. family:Times New Roman”>1 time, and patients who have achieved therapeutic efficacy or stable disease should continue to be given maintenance therapy with the original endocrine drug, and if the tumor progresses, a decision should be made to change to another mechanism of endocrine therapy or to switch to other therapies such as chemotherapy depending on the condition.
At present, targeted therapy is available for HER2-positive breast cancer patients, and the main domestic drugs are trastuzumab The main domestic drugs are trastuzumab, patuximab, pyrrolizidine, T-DM1, lapatinib, etc.
- HER2Gene amplification: immunohistochemistry staining3+, FISHpositive or pigment in situ hybridization (CISH) positive.
-
HER2immunohistochemical staining (2+) in patients who require furtherFISHorCISH< span style="font-family:Arial">to detectHER2gene amplification.
- style=”margin-left: 71pt”>
- Must obtain before treatmentPathological evidence of HER2positivity must be obtained before treatment.
- Must obtain before treatmentPathological evidence of HER2positivity must be obtained before treatment.
-
Trastuzumab monoclonal antibody 6mg/kg(first dose8mg/kg< span style="font-family:Arial">) every3weekly regimen, or< span style="font-family:Times New Roman">2mg/kg(first dose4mg/kg) weekly regimen.
- style=”margin-left: 71pt”>
- Observation after first treatment4~8< span style="font-family:Arial">hours.
- Not usually used concurrently with adriamycin chemotherapy, but can be used sequentially.
- Observation after first treatment4~8< span style="font-family:Arial">hours.
- Can be used concurrently with non-anthracycline chemotherapy, endocrine therapy and radiation therapy.
-
Trastuzumab monoclonal antibody should be tested before starting treatment. span style=”font-family:Times New Roman”>LVEF, every3 during use “>3monthly monitoring1timeLVEF. In case of LVEF<45% or lower than pre-treatment during treatment -family:Times New Roman”>16%or more, treatment should be suspended and follow-up monitoringLVEFdynamic changes until recovery to 45%or more before continuing the medication. Trastuzumab therapy should be discontinued if recovery does not occur, or if it continues to worsen or if symptoms of heart failure develop.
- style=”margin-left: 44pt”>
-
- Indications: ① Primary infiltrative foci>1cm(T1cand above)HER2
- Indications: ① Primary infiltrative foci>1cm(T1cand above)HER2
-
Trastuzumab is recommended for patients with positive breast cancer. (2) Patients with HER2 positive lymph node negative breast cancer with a primary infiltrative focus of 0.6-1 cm (T1bN0) and patients with smaller tumors but micro-metastases in the axillary lymph nodes (pN1mi) may be recommended for trastuzumab. (iii) Primary infiltrates <0.5 cm (T1a) in T1a family:Times New Roman”>HER2-positive lymph node negative breast cancer patients are generally not recommended for trastuzumab, but patients with associated high-risk factors, such as hormone receptor negativity, high grade, Ki-67higher May be considered.
-
Relative contraindications: ①Pre-treatmentLVEF<40%. (2) The patient refused postoperative adjuvant targeted therapy.
- style=”margin-left: 71pt”>
- Treatment options: see Appendix for common treatment options13.
①Optional TCH (P), AC-TH (P) regimen, and for patients with high cardiac safety requirements, the TCH, TC4H (here C for CTX) and wPH regimens; for patients at high risk of relapse (e.g., lymph node For patients at high risk of relapse (e.g., positive lymph nodes), trastuzumab is recommended in combination with adjuvant chemotherapy with dual-targeted therapy with pertuzumab, 3 weeks 1 dose of 1. span>times at a dose of 420 mg (the first dose was 840 mg) for a total of 1 year; if ER+, consider also giving trastuzumab after the end of trastuzumab treatment family:Times New Roman”>1 year of neratinib intensification.
②Patients with small tumors (tumor diameter ≤1 cm) can be treated with the paclitaxel peri-therapy plus trastuzumab (wPH< /span>) regimen for treatment.
- Treatment options: see Appendix for common treatment options13.
-
Cautions: 1) Concurrent use with anthracyclines must be done with caution, but can be done in pre and post sequential phases. The use of anthracyclines in combination with non-anthracycline chemotherapy must be cautious. It can be used concurrently with non-anthracycline chemotherapy, endocrine therapy or radiotherapy. The duration of adjuvant therapy with trastuzumab remains1year.
HER2-positive breast cancer is highly sensitive to targeted therapy against HER2. The sensitivity of treatment is high and anti-HER2-targeted therapy should be included in the neoadjuvant regimen for this group of patients.
-
Selection and principles of neoadjuvant targeted therapy drugs: ①Trastuzumab and patuximab dual targeting is currently the preferred treatment strategy for neoadjuvant targeted therapy. ②ForHER2positive breast cancer patients who are eligible for neoadjuvant indication, an anthracycline-containing combination with paclitaxel regimen or non-anthracycline regimen combined with Trastuzumab
±Pattuzumab for neoadjuvant therapy. (iii) The addition of patuximab to neoadjuvant targeted therapy can further improve pathologic complete remission rates, with more benefit in HR-negative, gonadal-positive patients. ④ Patients with contraindications to anthracycline use, advanced age, or other cardiac disease concerns may benefit from an anthracycline-free regimen such as TCH
(P) regimens.
-
Caution: 1) Monitor the efficacy closely during neoadjuvant therapy and follow P. span>RECISTorWHO. Roman”>WHO criteria for evaluation of primary foci and/ criteria for evaluation of primary foci and/or lymph nodes, and patients who progress during treatment with trastuzumab may be considered for retention of trastuzumab in subsequent neoadjuvant therapy. (ii) Patients receiving neoadjuvant targeted therapy in the adjuvant phase should be supplemented with adjuvant trastuzumab±pattuzumab therapy up to 1year. (iii) For pCR that have not reachedHER2positive patients, priority is given to T-DM1intensive adjuvant therapy, or by continuing to complete trastuzumab in combination with patuximab co1 family:Arial”>year approach. Whether or not pCR is achieved, some studies have shown that extended treatment with neratinib in specific populations “font-family:Times New Roman”>1year may further reduce the risk of relapse. ④ There is insufficient evidence for neoadjuvant targeted therapy alone or in combination with endocrine therapy, and its use should be limited to clinical studies.
-
AdvancedHER2targeted therapy options for HER2-positive breast cancer (see Appendix14 for common treatment options)
Continued anti-HER2 therapy is important for HER2 The important treatment principle for positive advanced breast cancer is HER2 therapy.
- style=”margin-left: 72pt”>
- HER2First-line treatment options for advanced positive tumors.
- HER2First-line treatment options for advanced positive tumors.
- Trastuzumab and pertuzumab dual-targeted therapy in combination with paclitaxel is preferred. Other options include trastuzumab single-targeted in combination with paclitaxel, and trastuzumab in combination with other chemotherapeutic agents such as vincristine and capecitabine.
- For patients who have not used trastuzumab or are eligible for trastuzumab reintroduction (more than after the end of trastuzumab adjuvant therapy style=”font-family:Times New Roman”>1year or more for recurrent metastases), trastuzumab±pattuzumab-based first-line therapy should be preferred for patients who have not used trastuzumab or who are eligible for trastuzumab reintroduction. In contrast, patients with an interval of ≤6-12months between discontinuation of trastuzumab and relapse are recommended for second-line antiHER2 regimen.
-
ForHER2positive/HRpositive patients who are not suitable for chemotherapy or whose disease is progressing slowly can be considered for antiHER2therapy in combination with endocrine drugs as a first-line treatment option.
-
Treatment options for disease progression after trastuzumab±pattuzumab treatment.
- style=”margin-left: 55pt”>
- After disease progression on trastuzumab therapy, continued use of anti >HER2
targeted therapy.
- After disease progression on trastuzumab therapy, continued use of anti >HER2
-
The following treatment strategies are available when disease progresses after first-line therapy: ① For trastuzumab monotherapy ± patuximab treatment failure, single-agent emtrastuzumab (trastuzumab emtansine. T-DM1) may prolong progression-free survival
time and overall survival. ②Pyrrolitinib in combination with capecitabine prolonged progression-free survival compared with lapatinib in combination with capecitabine. (iii) Other anti-HER2-targeted agents: initumumomab combined with chemotherapy such as vincristine may also be used as an anti-treatment option for trastuzumab-non-resistant patients. HER2 as one of the treatment options. Combinations of two targeted agents alone (e.g., lapatinib in combination with trastuzumab) have also shown evidence of improved OS. ④Trastuzumab allows for cross-line therapy. ⑤ Those who have failed multiple lines of anti-HER2 therapy and do not have access to further therapy are recommended to participate in clinical studies.
- style=”margin-left: 96pt”>
- Caution.
①Trastuzumab, patuximab: LVEF<50% prior to treatment. Baseline assessment of cardiac function should be performed before application, and should be avoided for those at high risk of cardiovascular events. ②Concurrent anthracycline-based chemotherapy. Concomitant use of anthracyclines and other drugs with synergistic damaging effects should be avoided as much as possible. ③Cardiac function assessment should be performed regularly during treatment, and if LVEF decreases ≥15% from baseline or below normal range and decreases ≥10%, anti-HER2 therapy should be suspended on HER2 in family:Times New Roman”>3 to 4 weeks to recheck LVEF to re-evaluate the ability to continue anti-HER2 therapy. ④T-DM1: Normative platelet monitoring should be performed at baseline and during dosing, and the dose should be promptly reduced or discontinued in case of thrombocytopenia. In case of Grade 2 thrombocytopenia or above, be alert to the possibility of developing persistent thrombocytopenia, and if conventional platelet-raising therapy is not effective, promptly consult a specialist for consultation and management. ⑤Pyrrolitinib: Patient education should be provided before dosing for adverse effects such as diarrhea and management options, and diarrhea should be monitored and managed during dosing.
(vii) Traditional Chinese medicine treatment.
TCM helps to reduce the side effects of radiotherapy, chemotherapy, endocrine therapy and
adverse reactions, modulate patients’ immune function and physical status, improve cancer-related symptoms and quality of life, and potentially prolong survival, and can be an important adjunct to breast cancer treatment.
The main causes and mechanisms of breast cancer are internal injury, phlegm and blood stasis, and deficiency of positive energy. Based on the principle of dialectical treatment, the main treatment method of TCM is the use of Chinese herbal soup. In addition, adhering to the idea of TCM surgical treatment, with “Yin evidence“”Yang evidence“ on the treatment of breast cancer is a common clinical approach. Xiaojin Pill and Xihuang Pill are the treatment for breast cancer “yin evidence“”yang evidence“”. family:Times New Roman”>” is a representative Chinese patent medicine that is widely used in clinical practice. The safety and tolerability of patients are better with the proper use of proprietary Chinese medicines under the guidance of herbalists.
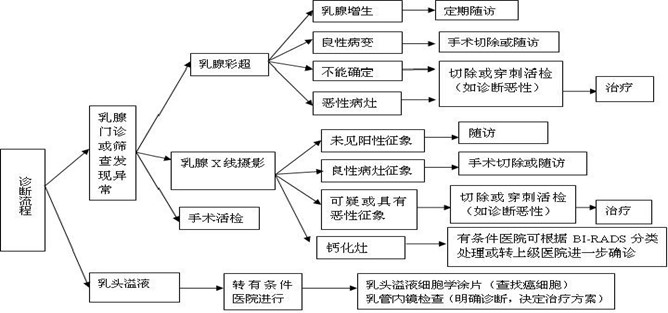
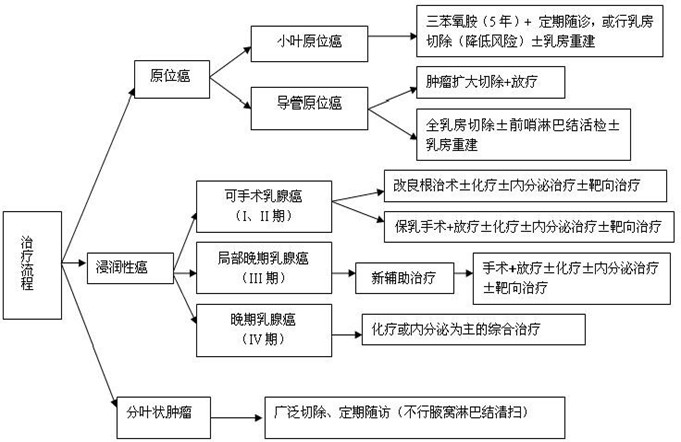 < span style="font-size:10pt">
< span style="font-size:10pt">
(a) Clinical physical examination: initially 2 years every 4 years. Roman”>4 to 6 months 1 time and thereafter 3
yearly every 6 months 1 < /span>times and 5 years later 1 time per year.
(ii) Breast ultrasound: every 6 months 1 time. /span>times.
(iii) Mammography X line: 1 time per year. /span>times.
(iv) X-ray chest radiograph or chest CT: 1 time per year.
(v) Abdominal ultrasound: every 6 months 1 time, 1 time, 1 time, and 1 time. /span>times, 3 years later to 1 times per year.
(vi) Patients with high risk factors such as axillary lymph node metastases 4 or more, baseline bone imaging and whole-body bone imaging will be performed yearly. font-family:Times New Roman”>1 time per year, which can be changed to every 2 years after 5 years. year1 time.
(vii) Routine blood, blood biochemistry, and breast cancer marker testing every 6 months 1 time and 1 time per year after 3 years.
(viii) 1 pelvic examination per year in patients on tamoxifen.
Attachments:1. /span>Basic Guidelines for Diagnostic Breast Imaging Reports
- style=”margin-left: 116pt”>
- Histologic Typing of Breast Cancer
- style=”margin-left: 114pt”>
- Histologic Grading of Invasive Breast Cancer
- Breast cancer of pTNM /span>Staging (AJCCstageNo. 8 Edition)
- Contents and Basic Format of Breast Cancer Pathology Report
- Breast CancerHER2/ neu FISHBasic format of test report
- Evaluation criteria for cosmetic results after breast preservation surgery
- Evaluation of the risk of recurrence after breast cancer surgery
-
Molecular Typing of Breast Cancer
- Commonly used adjuvant chemotherapy regimens
-
Common chemotherapy regimens for advanced breast cancer
-
Definition of menopause
- Common treatment options for postoperative adjuvant targeted therapy
- Common treatment options for postoperative adjuvant targeted therapy
-
-
AdvancedTargeted therapy for HER2positive breast cancer Common treatment options
- Treatment Guidelines for Breast Cancer (2022Evalidation Expert Group for the Preparation of Breast Cancer Guidelines (2022 Edition)
- Treatment Guidelines for Breast Cancer (2022Evalidation Expert Group for the Preparation of Breast Cancer Guidelines (2022 Edition)
- Commonly used adjuvant chemotherapy regimens
Annex 1
Essential Guidelines for Diagnostic Breast Imaging Reports
I. X-Ray Section
The report includes the following 5 aspects: indications for examination; guidelines for photographic technique; brief description of the components of the breast gland; clear description of important signs; comparison with previous films; and assessment of description; comparison with previous films; assessment categories and management.
(a) Indications for examination.
Asymptomatic screening; Xray diagnosis of breast disease; family history of breast cancer; history of breast disease; clinical findings Breast lumps, abnormal nipple overflow, skin abnormalities, local thickening, swelling, pain; other relevant examination findings of breast abnormalities; female over 40 years of age (especially senior childbearing or non-childbearing women) per at least once every 2 years for breast X-ray photography; women with menarche at 12 years of age should have a mammogram. The age of menarche before 12 years, age of menopause over 55 years, and other high-risk groups for breast cancer can be appropriately advanced.
(ii) Photographic techniques.
Conventional projection positions include bilateral medial-lateral oblique and cephalocaudal positions. For those with poorly visualized or incomplete breast parenchyma in conventional positions, additional positions can be selected according to the location of the lesion, including external medial, internal lateral, medial cephalopod axis, external cephalopod axis, caudal lobe, and sulcus position. The patient’s body can be placed in the position of the lesion, including medial, lateral, medial cephalopod axis, lateral cephalopod axis, caudal lobe, and sulcus.
(iii) A brief description of the glandular composition of the breast.
There are 4 types of fibroglandular tissue based on the density and distribution of the breast composition: Type A, fatty type; Type B, scattered fibroglandular type; C
type, unevenly dense type; type D, extremely dense type.
(D) Lesion localization.
- style=”margin-left: 84pt”>
- Localization: left, right, or bilateral.
- Site: including quadrant localization or clock face localization. Quadrant localization: outer upper quadrant, outer lower quadrant, inner upper quadrant, inner lower quadrant. Posterior areola, central region, and caudal axillary region do not require clock face localization or depth localization.
-
Depth: divided according to parallel to the chest wall3equal parts, anterior1/3(front), middle1/3(middle), back(middle), back(middle), back(middle), back(middle) =”font-family:Times New Roman”>1/3(rear) area.
- style=”margin-left: 60pt”>
- Distance from the nipple.
(v) Clear description of important signs.
Description of the lesion using a specialized vocabulary of breast X lines.
- style=”margin-left: 44pt”>
- Mass
Size, shape (round, ovoid, irregular), margin (clear, obscured, lobulated, indistinct, asterixis), density (dense, isointense, hypointense without fat, fat-containing density), concomitant calcification, other concomitant signs
- style=”margin-left: 44pt”>
- Calcification
Type and distribution.
- Distance from the nipple.
-
Types include: 1) benign calcifications: cutaneous calcifications, vascular calcifications, coarse or popcorn-like calcifications, coarse rod-like calcifications, and calcification of the skin. (1) benign calcifications: cutaneous calcifications, vascular calcifications, rough or popcorn-like calcifications, coarse rod-shaped calcifications, round calcifications, punctate calcifications, circular calcifications, calcified milk calcifications, suture calcifications, and dystrophic calcifications. ② Suspicious calcification: indeterminate calcification (BI-RADS 4B), coarse inhomogeneous calcification (BI-RADS 4B), fine polymorphic calcifications (BI-RADS 4B), fine-linear or fine-linear branching calcifications (BI-RADS 4C) ).
-
Distribution: scattered distribution ( mostly benign), regional distribution, cluster distribution, linear distribution (suspicious), segmental distribution (suspicious).
- style=”margin-left: 44pt”>
- Structural distortion
- Asymmetric dense
Spherical asymmetry (mostly normal variant), focal asymmetry, progressive asymmetry (suspicious)
- style=”margin-left: 44pt”>
- Other significant signs
Intramammary lymph nodes, skin lesions, isolated dilated ducts.
- style=”margin-left: 44pt”>
- Concomitant Signs
Dermal depression, nipple retraction depression, skin thickening, thickened trabecular structures, enlarged axillary lymph nodes, structural distortion, calcification, etc.
(vi) Comparison with previous films.
(vii) Assessment classification and management recommendations: A complete assessment classification should be given for each lesion, referring to BI-RADS.
- style=”margin-left: 44pt”>
- Incomplete assessment
BI-RADS 0: Existing images do not complete the evaluation and need to be combined with previous films or additional imaging. Other imaging studies recommended include: localized compression photography, magnification photography, compression magnification photography, special projection positions, or performing ultrasound.
- style=”margin-left: 44pt”>
- Assessment is complete
BI-RADS 1: Negative, breast X radiographs No abnormal findings, malignant probability 0, routine follow-up recommended.
BI-RADS 2: benign findings, presence of definite benign changes, no malignancy
- Structural distortion
signs, malignant potential 0, routine follow-up recommended. These include calcified fibroadenomas, cutaneous calcifications, multiple secretory calcifications, fat-containing lesions (lipid cysts, lipomas, and mixed-density malformations), intramammary lymph nodes, vascular calcifications, implants, and structural distortions with a history of surgery.
BI-RADS 3: high likelihood of benign, high likelihood of malignancy 0 to 2%, short-term follow-up is recommended. The expectation is that this lesion will stabilize or shrink on short-term (less than 1 years, typically 6 months) follow-up to confirm the judgment. The three signs of palpation-negative uncalcified well-defined masses, focal asymmetry, and punctate calcifications distributed in isolated clusters were classified as such. Conventional management advice: review of the diseased side of the breast with X radiography (usually 6 months), first 12 months and 24 months for bilateral breast X radiographic review, and if the lesions remain stable for 2 to 3 years, the original 3 categories were interpreted as 2 categories. If the lesion disappears or shrinks after follow-up, the judgment is changed to class 2 or class 1; if the lesion has progressed, biopsy should be considered.
BI-RADS 4: suspicious abnormalities without typical signs of malignancy, malignancy possible < span style="font-family:Times New Roman">2% to 95%, and biopsy should be considered. This category includes a large group of lesions requiring clinical intervention that lack characteristic morphologic changes of breast cancer but have the potential for malignancy. It is then subdivided into 4A, 4B, 4C, the clinician and patient can make the final decision on the management of the lesion based on its different malignant potential.
BI-RADS 4A: malignant potential 2% to 10%. Results are more reliable for benign biopsies or cytology and can be followed up routinely or 6 months later. A partially palpable solid mass with well-defined margins, such as an ultrasound-indicated fibroadenoma, a palpable complex cyst, or a palpable abscess, is included in this category.
BI-RADS 4B: malignant likelihood 10% to 50%. Need for pathology results
and imaging presentation are strictly compared, and the decision on benign pathologic findings depends on the consistency of imaging and pathology. Partially defined, partially infiltrated masses with puncture as fibroadenoma or fat necrosis are accepted and followed up. In contrast, further biopsies are required for puncture findings of papilloma or atypical hyperplasia.
BI-RADS 4C: malignant potential50% to 95%. Irregularly shaped solid masses with infiltrating margins or new clusters of small polymorphic calcifications can be classified in this category. Such lesions tend to be malignant and require further analysis in consultation with the pathology department in cases with benign pathological findings.
BI-RADS 5: Highly suspicious for malignancy, with a probability of malignancy ≥95%. There are typical imaging features of breast cancer, and appropriate clinical measures should be taken. Irregularly shaped, dense masses with stellate margins, segmental or linear distribution of fine linear and branching calcifications, and irregular stellate masses with polymorphic calcifications are all classified in this category.
BI-RADS 6: Biopsy-proven malignancy and clinically aggressive treatment is indicated. This classification is used for imaging evaluation where biopsy has confirmed malignancy but treatment has not yet been performed. It is primarily used to evaluate imaging changes after biopsy or to monitor imaging changes for preoperative treatment. Note that BI-RADS 6 is not appropriate for follow-up after complete resection of a malignant lesion. The final evaluation should be BI-RAD category 3 or 2 in cases where there is no tumor remnant after surgery that does not require further resection. . Suspected malignant lesions that are not in the same area as the biopsy should be separately sided, localized, evaluated for classification and management recommendations, and their final evaluation should be BI-RADS 4 or 5. New Roman”>5, biopsy is recommended.
II. Ultrasound section
(a) Reporting of ultrasound.
Content includes.
- style=”margin-left: 68pt”>
- Clinical history, examination indications
- Whether there is a relevant previous ultrasound for comparison
- Scope of ultrasound scan and examination technique
-
Lesion description: (1) Briefly describe the type of breast tissue in the scan area. (2) Lesion size measurement (at least measurement2diameters); small simple cysts do not need to be measured in their entirety. (3) Location of the lesion (using a bell-face description, also describe the depth of the lesion from the nipple). (4) Brief description of the lesion using ultrasound terminology.
- style=”margin-left: 44pt”>
- Combined with relevant clinical physical examination,< span style="font-family:Times New Roman">Xlinear photography,MRI or other imaging tests
- Overall assessment and management recommendations
(ii) Ultrasound assessment classification of breast lesions.
Referring to the NCCN guidelines for screening and diagnosis proposed by BI-RADS ( Breast imaging reporting and data system) classification criteria.
- style=”margin-left: 44pt”>
- Assessment incomplete
Class 0: The existing images do not complete the evaluation and require further evaluation with other imaging or comparison with previous exams.
- style=”margin-left: 44pt”>
- Complete evaluation
Category 1: Negative, no abnormalities seen (if normal intra-mammary or anterior axillary lymph nodes are found, they are also 1) Roman”>Category 1). Routine physical examinations (1 per year) are recommended.
Category 2: Benign lesions, including simple cysts and cumulus cysts; intra-mammary grafts; stable postoperative changes; fibroadenomas that do not change after follow-up. Recommendations Regular follow-up (every 6 months to 1 years 1 times).
Class 3: Benign may be large. These include solid masses with well-defined margins, round or oval shape, and a transverse diameter greater than the high diameter, which are likely to be fibroadenomas; they also include palpation
- Combined with relevant clinical physical examination,< span style="font-family:Times New Roman">Xlinear photography,MRI or other imaging tests
negative complex cysts and clustered microcysts. Short-term follow-up is recommended (every 3 to 6 months)
1 time), 2 years Those with no change at follow-up can be downgraded to 2 categories.
Class 4: suspicious for malignancy.
4A: Low-level suspicious malignancy (≥3%-≤10%). Pathology report results are generally nonmalignant and should be followed up 6 months or routinely after obtaining benign biopsy or cytology results. For example, a palpable, locally well-defined, substantial mass with ultrasound features suggestive of a fibroadenoma; a complex palpable cyst or possible abscess.
4B: A moderately likely malignant lesion (>10% to ≤50%). A combination of imaging and pathology findings is required. Partially well-defined and partially ill-defined fibroadenomas or fat necrosis can be followed, but papillomas may require excisional biopsy.
4C: more likely to be malignant (>50% to ≤94%), but not as grade 5 as typically malignant. Examples include irregular parenchymal masses with poorly defined borders or new clusters of fine pleomorphic calcifications. Lesions of this grade will likely be malignant in outcome. Pathology (e.g., fine-needle aspiration cytology, hollow-core needle aspiration biopsy, surgical biopsy) is recommended for definitive diagnosis.
Class 5: Highly suspicious for malignancy and clinically appropriate measures should be taken (almost certain malignancy). Ultrasound has characteristic abnormal signs and the risk of malignancy is greater than 95%. Definitive treatment should be initiated. When considering sentinel lymph node visualization and neoadjuvant chemotherapy, an image-guided hollow-core needle aspiration biopsy is appropriate to obtain a histologic diagnosis.
Class 6: Biopsy-proven malignancy and clinically appropriate measures should be taken. This category is used for the evaluation of images that are biopsy-proven malignant but not yet treated
up. The main focus is to evaluate imaging changes after biopsy or to monitor imaging changes prior to surgery with neoadjuvant chemotherapy.
III.
The report includes the following 6 aspects: indications for examination; scanning technique; brief description of the components of the breast gland A brief description of the components of the gland; description of significant signs; comparison with previous films; and assessment of classification and management.
(i) Indications for examination.
- style=”margin-left: 80pt”>
- Indications for examination
Diagnosis of breast cancer, breast cancer staging, evaluation of neoadjuvant therapy efficacy, axillary lymph node metastases of unknown origin, preoperative evaluation and postoperative follow-up of breast-conserving patients, post-mastopexy follow-up, screening of high-risk groups, MRI-guided puncture biopsy.
- style=”margin-left: 80pt”>
- Clinical history
The patient’s symptoms, signs, family history, risk factors, menstrual status and cycle, history of hormone replacement therapy or anti-hormone therapy, history of chest radiation therapy, history of breast surgery and pathology results, presence of anterior films and related investigations (breast X line photography, ultrasound, etc.).
- style=”margin-left: 68pt”>
- Pre-examination preparation
Premenopausal women with MRI exams should be scheduled as early as possible in the 2nd week of the menstrual cycle. span>week. This is not required for patients with confirmed breast cancer.
(ii) Scan sequence and parameters.
Enhanced scans are required for all breast MRI examinations, except for evaluation of prosthetic implants only. 1.The scan sequence includes at least: T1 weighted imaging non-fat suppression
sequence, T2 weighted imaging fat suppression sequence, dynamic enhancement T1-weighted imaging fat suppression sequence, diffusion-weighted imaging sequence. 2.Enhanced scan sequences: contrast agent selected is gadolinium diethylenetriaminepentaacetic acid, injected dose 0.1 to 0.2 mmol/kg, using a pressure syringe at 2 to 2. family:Times New Roman”>3 ml/s via the elbow vein, 10 seconds for rapid group injection, and after contrast injection at the same rate 15 ml of saline to flush the tube. Note that the T1-weighted imaging sequence before and after enhancement is preferably fat-suppressed and bilateral mammary glands are imaged simultaneously, and subtraction processing and dynamic enhancement curves are recommended. A total of 5 to 9 acquisitions were made after contrast injection, and the scan delay time was determined by 8 to 10 minutes is appropriate. 3. Diffusion-weighted imaging: single-excitation planar echo sequence transaxial position scanning with lipid suppression is generally performed to suppress the conventional use of frequency saturation or water excitation. The use of parallel acquisition techniques helps to reduce magnetic susceptibility artifacts and improve image quality, with a conventional parallel acquisition factor of 2 to 3. . Scanning generally uses 2 values of b, and routinely uses 0 or 50s/mm2 and 800 s/mm2 or 1000 s/mm2.
Imaging parameters: scanned layer thickness ≤ 3mm, intra-layer resolution <1.5mm, scan time <2 minutes.
Image post-processing: The dynamic enhancement scan sequence requires image post-processing and generates a time –signal profile (< span style="font-family:Times New Roman">TIC). Take care to find the area of interest where the lesion is largest and the enhancement is significant. The area of interest should avoid areas of hemorrhage, liquefaction, necrosis, and cystic changes, and the area of interest cursor should be no less than 5 voxels.
(C) Guidelines for diagnostic reporting of breast MRI.
Refer to BI-RADS criteria.
- Brief description of the composition of the breast gland: requires non-fat suppression on plain scanT1weighted imaging for evaluation. There are4types:Type A, fatty;Type Btype.
scattered fibroglandular type; C type, unevenly dense type; Type D, extremely dense.
-
There are four types of background parenchymal enhancement of the breast: almost no enhancement, mild enhancement, moderate enhancement, and marked enhancement.
- style=”margin-left: 44pt”>
- Description of signs: using breast style=”font-family:Times New Roman”>MRIspecialized vocabulary to describe the lesion.
(1) Point-like enhancement. (2) Masses: morphology (round, ovoid, irregular), margins (clear, irregular, burr), internal strengthening characteristics (uniform strengthening, inhomogeneous strengthening, circumferential strengthening, internal low signal separation), dynamic strengthening characteristics (early strengthening rate: slow strengthening, medium strengthening, fast strengthening; time
– signal profile: slow-rising sustained, fast-rising plateau, and fast-rising contour). (3) Non-mass-like enhancement: distribution (focal, linear, segmental, regional, multi-regional, diffuse distribution), internal enhancement features (uniform, inhomogeneous, clustered pebble-like, cluster-like circumferential enhancement). (4) Other signs and concomitant signs: intramammary lymph nodes, cutaneous lesions, nonenhancing lesions (preenhancing high-signal ducts, cysts, postoperative hematoma effusion), skin thickening, skin edema, nonenhancing masses, structural distortion, nipple retraction, skin retraction, pectoral muscle invasion, chest wall invasion, enlarged axillary lymph nodes. ⑤ Implants: type of prosthesis, position, and whether it is intact.
- Description of signs: using breast style=”font-family:Times New Roman”>MRIspecialized vocabulary to describe the lesion.
-
Localization of the lesion: left side /right side; quadrant and clock face localization; depth of lesion; distance from nipple.
- style=”margin-left: 44pt”>
- Comparison with previous films.
- Assessment classification and management recommendations.
- Comparison with previous films.
-
Assessment incomplete:< span style="font-family:Times New Roman">0Class: The evaluation is not complete with the existing images and needs to be combined with previous films or other imaging studies. GenerallyMR exams are less frequently used in this category.
- style=”margin-left: 96pt”>
- Assessment is fully.
BI-RADS 1: Negative, malignant probability 0 , routine follow-up is recommended.
BI-RADS 2: benign finding, malignant probability 0, with routine follow-up recommended. This includes non-enhancing fibroadenomas, cysts, non-enhancing old scars, breast prostheses, and fat-containing lesions (lipid cysts, lipomas, and malignant tumors).
BI-RADS 3: Probably benign lesions with less likelihood of malignancy 2%, and short-term follow-up is recommended. Stability needs to be determined by follow-up. The more suspicious cases can be followed up after 3 months and are usually reviewed after 6 months.
BI-RADS 4: suspicious for malignancy, but without typical signs of malignancy, possibility of malignancy < span style="font-family:Times New Roman">2%-95%, and biopsy should be considered. Such lesions do not have characteristic morphologic changes of breast cancer, but have the potential for malignancy. The lesions can also be subdivided into 4A, 4A, 4B, and 4C.
BI-RADS 5: high suspicion of malignancy, probability of malignancy ≥ 95%, and appropriate clinical measures should be taken.
BI-RADS 6: Biopsy-proven malignancy and clinically appropriate measures should be taken.
Annex 2
Histological typing of epithelial tumors of the breast
|
invasive breast cancer < /td> |
|
Infiltrative carcinoma, non-specific type |
|
Carcinoma with myeloid features |
|
Carcinoma with neuroendocrine differentiation |
|
Cancer with pleomorphic features |
|
Carcinoma with osteoblast-like interstitial giant cells |
|
Carcinoma with choriocarcinoma features< /p> |
|
Carcinoma with melanocytic features |
|
Carcinoma with eosinophilic features |
|
Cancer of the fat-rich type |
|
Glycogen-rich clear cell carcinoma |
|
Carcinoma with sebaceous features |
|
Microinvasive carcinoma |
|
Infiltrative lobular carcinoma (classic, pleomorphic) |
|
Small tube cancer |
|
Septate carcinoma< |
|
Mucinous carcinoma |
|
Mucinous cystic carcinoma |
|
invasive micropapillary carcinoma |
|
Carcinoma with sweat gland differentiation |
|
Chemical carcinoma |
|
Fibromatosis-like metastatic carcinoma< |
|
Squamous cell carcinoma |
|
Chemical carcinoma with mesenchymal differentiation (chondrogenic differentiation, osseous differentiation, other mesenchymal differentiation) |
|
Mixed septic carcinoma |
|
Rare and salivary gland type tumors |
|
Glandular follicular cell carcinoma |
|
Adenoid cystic carcinoma |
|
Secretory carcinoma |
|
Mucinous epidermoid carcinoma |
|
Polymorphic adenocarcinoma |
|
High-cell carcinoma with polarity flip |
|
Neuroendocrine tumors |
|
Neuroendocrine tumors,1level |
|
< span style="font-family:Arial">Neuroendocrine tumors,2level > |
|
Neuroendocrine carcinoma (small cell type, large cell type) |
|
epithelial–myoepithelial tumors |
|
Multimorphic adenoma |
|
Adenomyeloblastoma |
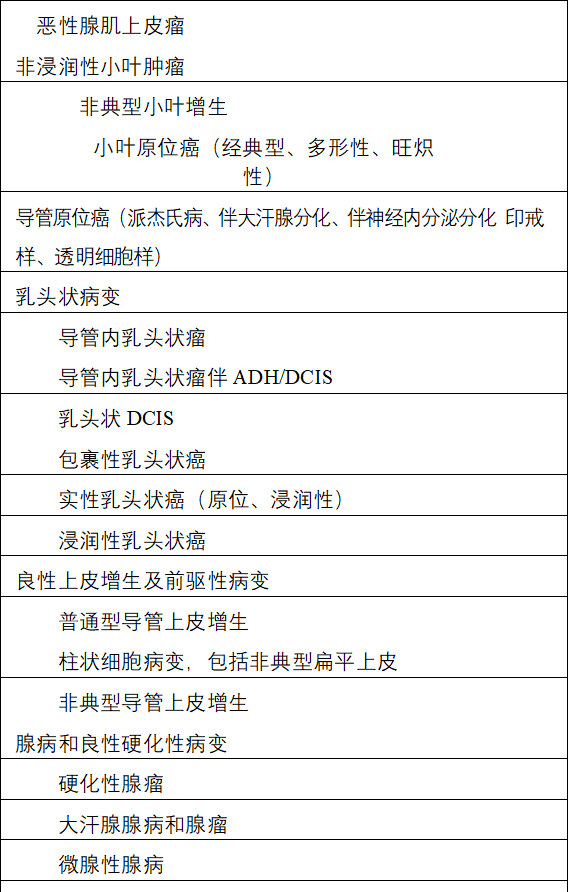 ,
,
|
Adenoma |
|
Ductal adenoma |
|
Lactating adenoma |
| < p style="margin-left: 37pt">Ductal adenoma |
Attachment 3
Histological grading of invasive carcinoma of the breast
According to the presence of glandular duct formation, nuclear pleomorphism and nuclear schizogram count 3 indicators for grading, and a modified Scarff-Bloom-Richardson grading system is recommended.
 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0836_20225.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0836_20225.png" alt=""/>
 Morphological characteristics Score
Morphological characteristics Score
Glandular duct structure 1
Most of the tumor components (>75%) 2
Moderate numbers (10% to 75%) 3
Few or none (<10%) Polymorphism of the nucleus
Small nuclei with regular and consistent morphology 1
Nuclei are medium sized and irregular
2
uneven size
Large nuclei with diverse morphology 3
Nuclear division count
 Depends on the field of view under the microscope 1 to 3
Depends on the field of view under the microscope 1 to 3
Examples of nuclear division counts in three different fields of view
|
field of view diameter (mmmm /span>) |
0.44 |
0.59 |
0.63 |
|
Area of view (mm2) |
0.152< |
0.274 |
0.312 |
Nuclear division count (number of nuclear divisions per 10HPF)
|
0~5 |
< span style="font-family:Times New Roman">0~9 |
0< span style="font-family:Arial">~11 |
1 |
|
6~11 |
10~19 |
12~22 |
2 |
|
≥11 |
≥19 |
≥22 |
≥22 =”font-family:Times New Roman; font-size:16pt”>3 |
Note: The glandular duct structure, nuclear pleomorphism and The three indicators of nuclear division count were scored separately: the total score was 3 to 5, and the histological grading was grade I; 6 to 7 points, histological grade II; 8 points, histological grade II; 8 to 9 points, histologically graded as grade III.
Attachment 4
pTNM staging of breast cancer
Primary tumor (invasive carcinoma) (pT)
pTX: Primary Tumor cannot be estimated
pT0: No primary Evidence of tumor #
pTis(ductal carcinoma in situ): ductal carcinoma in situ # (lobular carcinoma in situ has been removed from this classification)
pTis ( Paget’s disease): papillary Paget’s disease, not accompanied by invasive carcinoma in the breast parenchyma and / or carcinoma in situ (ductal carcinoma in situ and /or lobular carcinoma in situ) Component #
pT1: Maximum tumor diameter ≤20 mm (based on 5 mm, 10 mm can be subdivided into T1a, T1b, T1c)
pT1mi. Maximum tumor diameter ≤1mm (microinvasive carcinoma) pT1a:1mm
are counted as 2mm).
pT1b: 5mm >
pT2: < span style="font-family:Times New Roman">20 mm
pT3: Maximum tumor diameter > 50 mm
pT4: direct invasion of the chest wall and / or skin by tumors of any size (formation of ulcers or fleshy masses); tumor invasion of the dermis alone is not diagnostic T4
pT4a: Invasion of the chest wall (excluding simple pectoralis major and minor muscle involvement)
pT4b: skin ulcers, and / or ipsilateral satellite nodules visible to the naked eye, and /or skin edema (including orange peel signs) but less than the diagnostic criteria for inflammatory breast cancer (only microscopically visible skin satellite nodules without skin ulceration or edema are not diagnosed T4b)
pT4c: < span style="font-family:Times New Roman">T4a and T4b
pT4d: Inflammatory breast cancer ##
(Note: ypT after neoadjuvant chemotherapy should be calculated based on the largest residual tumor foci; areas of fibrosis associated with infiltrative paracancer treatment are not counted as tumor (maximum diameter; multifocal residuals should be labeled m)
Note: Tumor size is accurate to mm
#For the purpose of this list, these items should only be used in cases of previously diagnosed invasive carcinoma with no residual invasive carcinoma after preoperative (neoadjuvant) therapy cases
##Inflammatory breast cancer is a clinical –pathologic term characterized by diffuse erythema and edema (orange peel) involving 1/3 or more of the breast skin. The skin changes are attributed to lymphedema and are caused by intralymphatic tumor thrombi in the skin, which can be unremarkable in small skin biopsies. However, for the determination of invasive carcinoma in breast tissue or at least in cutaneous intralymphatic ducts and its biological indicators such as ER, PR, HER2 status, histological diagnosis is still mandatory. The above clinical changes with cutaneous intralymphatic neoplastic emboli without skin cannot be defined as inflammatory breast cancer. Localized breast cancer with direct invasion of the dermis or ulcerated skin without the above clinical changes in the skin as well as dermal lymphovascular neoplasia can also not be defined as inflammatory breast cancer. Therefore, the term inflammatory breast cancer should not be misapplied to locally advanced breast cancer. Rare cases exhibit all the features of inflammatory breast cancer, but the extent of skin lesion involvement is less than 1/3 and should be based on the size and dimensions of the underlying cancer.
Inch to classify.
Simultaneous ipsilateral multiple carcinomas (multicentric): Tstaging by the largest carcinoma and recording the size of the other carcinomas; note the exclusion of carcinomas with satellite nodes and complex shapes Cancer foci (pathology sampling combined with clinical imaging)
Regional lymph nodes (pN)
pNX: Cannot Evaluate regional lymph nodes
pN0: No regional Lymph node metastases or only ITCs
pN0(i-): no metastases on histology, negative immunohistochemistry
pN0 (i+): only ITCs: tumor cell clusters < span style="font-family:Times New Roman">≤0.2mm (multiple focal ITCs may be present in a single lymph node, the largest must ≤0.2mm; if the total number of ITCs cells is greater than 200, the diagnosis of micrometastasis should be made)
pN0 (< span style="font-family:Times New Roman">mol-): histologically non-metastatic, RT-PCR negative
pN0(< span style="font-family:Times New Roman">mol+): no ITCs detected, but RT-PCR positive
pN1mi: micro metastases (~200 cells, >0.2 mm, ≤2.0 mm)
pN1a: < span style="font-family:Times New Roman">1 to 3 lymph nodes with metastases and at least 1 tumor focus > 2.0
mm
pN1b: Metastasis to the ipsilateral internal mammary anterior lymph node (parasternal, trans
metastasis > 0.2 mm) and negative axillary lymph nodes.
pN1c: < span style="font-family:Times New Roman">N1a and N1b
pN2a: 4 to 9 axillary lymph node metastases (at least 1 tumor foci >
- style=”margin-left: 48pt”>
- mm)
pN2b: Clinical detection of internal breast (parasternal) lymph node metastases (with or without pathological confirmation) without axillary metastases
pN3a: ≥10 axillary lymph nodes with metastases (at least 1 tumor focus)
> 2.0mm) or subclavian lymph node (top of axilla) metastasis
pN3b: < span style="font-family:Times New Roman">pN1a or pN2a accompanied by cN2b (imaging-confirmed internal breast lymph node metastasis); or pN2a with pN1b.
pN3c: Metastasis to the ipsilateral supraclavicular lymph node
Staging: T1 including T1mi, while N1mi is relevant for staging; if the lymph node is only anterior, mark Nx (< span style="font-family:Times New Roman">sn)
Distant shift (< span style="font-family:Times New Roman">M)
Not applicable
cM0 (i+): no clinical or imaging evidence of distant metastasis; however, molecular biology or microscopic detection in circulating blood, in the bone marrow, or in other non-regional lymph nodes in patients without signs and symptoms of metastasis Tumor cell population with ≤0.2 mm in the tissue
pM1: clinical and imaging means to detect distant metastases and / or histologically confirmed metastases & gt;0.2 mm
|
Staging |
|||||
|
0Issue IAA family:Arial”>Issue IBIssue I T0N1miM0 |
Tis T1 T0, T1 T1N1miM0 |
N0 N0 |
N1mi |
M0 M0 M0 |
|
|
IIAIssue |
T0,T1 |
N1 |
M0 |
||
|
T2 |
N0 |
M0 |
||||
|
IIBPeriod |
T2 |
N1 |
M0 |
|||
|
N0 |
M0 |
|||||
|
IIIAIssue |
T0,T1,T2 |
N2 |
M0 |
T3 N1
, N2 M0
III B period T4 N0 , N1, N2 M0
IIIC period Any T N3 M0
Phase IV Any T Any N M1
Attachment 5
Contents and Basic Format of Breast Cancer Pathology Report
Pathology Number Hospitalization Number
Patient Name: Gender: Age: Department.
Specimen type: Bed number: Sending physician: Date received


What the naked eye sees
Modified radical specimen of left breast cancer, size 25cm×16 cm × 5.4 cm, with pike skin attached, area 12.5 cm×4 cm, with no abnormalities in the nipple skin. A mass of size 3.5 cm was seen in the external superior phenomenon from the nipple 3.4 cm×. =”font-family:Times New Roman”>2.5 cm×1.2 cm, the cut surface was grayish white and hard with poorly defined borders from the pectoralis fascia 1.2 cm. family:Times New Roman”>0.5cm, without involvement of the nipple skin. The peripheral mammary gland was partially grayish and tough. Several nodules were found in the axilla, with diameters of 0.2 to 1.8 cm.
Pathological diagnosis
After neoadjuvant therapy for breast cancer
(1) (modified radical specimen of left breast cancer)
Invasive carcinoma of the breast, non-specific type, grade III (3+3+2=8 points) with few high-grade ductal carcinomas in situ (approximately 5%), with visible vascular aneurysm emboli and nerve invasion
Incidence, some tumor cell regression with interstitial fibrosis and focal lymphocytic and histiocytic infiltration, consistent with mild post-treatment changes (Miller&Payne classification, grade 2 ). Tumor size 3.4 cm x 2.5 cm x 1.2 cm (invasive carcinoma component) without involvement of the nipple, skin or pectoralis muscle fascia. The peripheral breast showed adenopathic changes with some ductal epithelial normal-type hyperplasia.
Metastatic carcinoma of the lymph nodes (4/22) with partial lymph nodes with mild post-treatment changes
changes.
Posterior lymph nodes 2/3
Axillary lymph nodes 2/19
ypTNM Staging:ypT2N2Mx
Immunohistochemistry results: ER(+< /span>, 30% strong positive), PR (PR (–, <1%), <1%)
HER2 (2+) (FISH testing required) CK5/6 (CK5/6) (–), EGFR
(–), Ki- 67 (30%).
Signature of reporting physician: Date of diagnosis


Attachment 6
Basic format of HER2/neu FISH test report for breast cancer
Pathology Number Case Number
FISH test number
Name Gender Age Ethnicity
Ward Sending physician Sending material 1: Date of receipt Pathological diagnosis
Test results with graphs (optional)
HE staining Immunohistochemical staining (2+) /span>)
FISH
Total number of tumor cells ( ).
Total number of HER2 gene copies ( ), average HER2 gene copies per cell. Roman”>HER2 copy number per cell ().
Total CEP17 copy number (), average CEP17 copy number per cell (). Roman”>CEP17 copy number per cell
().
HER2 / CEP17 ratio =< /span>( )
FISH test results: draw “√” in the corresponding ( ) below Roman”>”√”
Average HER2 copy number / cells <4.0, ratio <2.0 (no amplification) Negative ( )
Average HER2 copy number / cells4.0 but <6.0, ratio <2.0 (no amplification) Negative ( )
Average HER2 copy number /cell4.0, ratio 2.0 or the average HER2 copy number / cells 6.0, ratio <2.0 (amplification) Positive ( )
Unable to determine ( )
HER2 Gene Heterozygosity: No□ Yes□ (%)
HER2 gene amplification signal distribution mode: punctiform □ Dot clusters or sheets□ Note
- style=”margin-left: 68pt”>
- If the test specimen is a needle-aspirated tissue specimen, it is recommended to perform the surgical specimen’sFISH
testing or retesting.
- style=”margin-left: 68pt”>
- In case of piecewise amplification, the region should be indicatedHER2/CEP17 ratio.
Attachment 7
Evaluation criteria for cosmetic results after breast preservation surgery
Ⅰvery good: the shape of the diseased side of the breast is the same as the opposite side.
II. Good: The diseased side of the breast is slightly different from the contralateral side, and the difference is not significant. III. Fair: significantly different from the contralateral side, but no severe deformity. Ⅳ. Poor: Severe malformation of the diseased side of the breast.
Attachment 8
Assessment of the risk of recurrence after breast cancer surgery
Dangerousness |
Evaluation Highlights |
|
|
Metastatic lymph nodes |
Other |
|
|
Low |
negative |
with the following6: size of the lesion in the specimen (pT) 2cm; grading1grade a; no vascular aneurysm embolismb< span style="font-size:16pt">;ERand/ orPRpositive;HER2no overexpression or amplification of the genec; age35years |
|
Moderate |
negative |
Following6at least1Article: size of the lesion in the specimen (pT)>2cm;grading2~Grade 3; with vascular aneurysm embolism; ER< /span>andPRnegative;HER2gene overexpression or amplification; age<35years |
|
1~3枚positive |
NoHER2gene overexpression and amplification andERand/< span style="font-family:Arial">or PRPositive |
|
|
height |
1~3positive |
HER2gene overexpression or amplification orERandPRnegative |
|
4 枚 Positive | ||
|
molecular typing |
Pathologic characterization |
Remarks |
|
LuminalA Type |
ERpositive PRPRPR Masculine and PR High Expression (>20%)a HER2negative Ki-67Low Expression (<14%)< /span> |
Ki-67high and low expression determination values may vary in different pathology experimental centers, generally using 20%~30%as a judgmentKi-67as a cutoff value for high and low |
|
Luminal B Type |
Tubular lumenBType (<) span style="font-family:Times New Roman">HER2 negative) ERER =”font-family:Arial”>and/orPRpositiveHER2< span style="font-family:Arial">negative andandKi-67high expression (≥14%< span style="font-family:Arial">) or PRPR =”font-family:Arial”>Low Expression (≤20%) |
|
|
Tubular lumenBtype (HER2 (Positive) ER ER =”font-family:Arial”>and/orPRpositive HER2positive (protein overexpression or gene amplification) Any statusKi-67 |
||
HER2over-expression type |
HER2positive (protein overexpression or gene amplification) ERERER =”font-family:Arial”>andPRnegative td> |
base-like type |
Non-specific invasive ductal carcinoma (triple negative) ERnegative,PRnegative,negative,HER2negative |
triple-negative breast cancer and Basal-liketype of breast cancer match about 80%. However, triple-negative breast cancer also includes some specific types of breast cancer such as medullary (typical) and adenoid cystic carcinoma, which recur |
|
Lower risk of transfer |
Attachment 10
Commonly used adjuvant chemotherapy regimens
TAC regimen
Docetaxel 75 mg/m2 iv day 1 of doxorubicin 50 mg/m2ivth day 1 day of cyclophosphamide 500 mg/m2 iv Day 1
21 days for 1 cycles for a total of 6 cycles (all cycles are supported with G-CSF).
Dose-dense AC→P scheme
Doxorubicin 60 mg/m span style=”font-size:10pt”>2 iv Day 1 of cyclophosphamide 600 mg. Roman”>600 mg/m2ivth1 day 14 days for 1 cycle, for a total of < span style="font-family:Times New Roman">4 cycles
Sequence with paclitaxel 175 mg/m. span style=”font-size:10pt”>2 iv 3 hours on 1 day
14 days for 1 cycles for a total of 4 cycles (all cycles are supported with G-CSF).
AC→P/T Program
Doxorubicin 60 mg/m2 iv day 1 of cyclophosphamide 600 mg/m2ivth day 1 day 21 is 1 cycle for 4 cycles
Sequential paclitaxel 80 mg//m2 iv 1 hours on day 1 per week 1 times a week for a total of 12
week
or paclitaxel 175 mg/m
or paclitaxel 175 mg2 iv 1hour on 1day, every 3 weeks 1 times, for a total of 12
week
or docetaxel 100 mg/m
or docetaxel 100 mg2 iv day 1, every 3 days Roman”>3 weeks 1 times, for a total of 12 weeks. TC Program
Docetaxel 75 mg/m. span style=”font-size:10pt”>2 iv Day 1 of cyclophosphamide 600 mg. Roman”>600 mg/m2ivth1 day
21 days for 1 cycle, for a total of 4 cycles.
AC Program
Doxorubicin 60 mg/m
Doxorubicin span style=”font-size:10pt”>2 iv Day 1 of cyclophosphamide 600 mg. Roman”>600 mg/m2ivth1 day
21 days for 1 cycle, for a total of 4 cycles.
FAC program
Fluorouracil 500 mg/m. span style=”font-size:10pt”>2ivth, 1, 8 days of Doxorubicin 50 mg/m2 iv Day 1
Cyclophosphamide 500 mg/m
Cyclophosphamide 2 iv Day 1
21 days for 1 cycle, for a total of 6 cycles.
EC Program
Epirubicin 90~100 mg/m 2 iv Day 1 Cyclophosphamide 600~830 mg Roman”>600 to 830 mg/m2ivth1 day
21 days for 1 cycle, for a total of 8 cycles.
FEC→T scheme
Fluorouracil 500 mg/m2 ivthl day epirubicin 100 mg/m2ivth1 day of cyclophosphamide 500 mg/m2 iv Day 1
21 days for 1 cycle, for a total of 3 cycles
Sequence with docetaxel 100 mg/ m2 ivday 1
21 days for 1 cycle, for a total of 3 cycles.
FEC→P program
Fluorouracil 600 mg/m. span style=”font-size:10pt”>2 ivth day 1Table Zoebixin 90 mg/m2ivth1 day of cyclophosphamide 600 mg/mm =”font-size:10pt”>2 iv Day 1
21 days for 1 cycle, for a total of 4 cycles
Sequence with paclitaxel 100 mg/m. span style=”font-size:10pt”>2 iv Day 1 per week 1. Roman”>1 times a week for 8 weeks.
Attachment 11
Common chemotherapy regimens for advanced breast cancer
Preferred single agent
Paclitaxel 80mg/m2, intravenous, first < span style="font-family:Times New Roman">1, 8, 8, 15 days, 28 days as a cycle or 175mg/m2, IV, day 1, 21 days span>days for one cycle.
Capecitabine 1000-1250mg/m2 orally 2 times daily on days 1-14, 2. family:Times New Roman”>21 days for one cycle.
Gemcitabine 800-1200mg/m2. static drip, doses 1, 8, 15 days and 28 days for one cycle.
Vincristine 25mg/m2 is given as an IV; or 60mg/m2 orally at 1, 8, 15
days, 28 days for one cycle.
Doxorubicin liposomal 50mg/m2, intravenous. Day 1, 28 days for one week
period.
Other single-drug regimens
Docetaxel 60-100mg/m2, IV for the first 1 day and 21 days for one cycle. Albumin-bound paclitaxel 100 mg/m2 or 125 mg/m2, IV, pp.
1, 8, < span style="font-family:Times New Roman">15 days.
28 days for one cycle .
or 260mg/m2, IV, first < span style="font-family:Times New Roman">1 day and 21 days for one cycle.
Carboplatin AUC 5 to 6, IV, day 1, 21-28 days for one cycle. Cisplatin 75mg/m2, IV, day 1. Roman”>1 day and 21 days for one cycle.
Epirubicin 60-90mg/m2 in a sedative drip. Day 1, 21 days for one cycle. Doxorubicin 60mg/m2, IV, for the first 1 day. Roman”>1 day and 21 days for one cycle. Or 20mg/m2, IV, day 1. Roman”>1 day, once a week.
Cyclophosphamide 50 to 100 mg, orally, 1 time daily on days 1-21, 28
days for one cycle.
Etoposide capsules 75-100mg orally on day 1-10 days, 21 days for one week
period.
Common chemotherapy regimens for combination chemotherapy
TX
Docetaxel 75mg/m2 1day
Capecitabine 950 to 1000mg /m2, orally, 2 times daily, the first 1-14 days 21 days for one cycle.
GT
Gemcitabine 1000-1250mg/m2 , drip, day 1, 8 paclitaxel 175mg/m2, IV, day 1.
or docetaxel 75mg/m2, IV, day < span style="font-family:Times New Roman">1 day
21 days for one cycle.
GC
Gemcitabine 1000mg/m2, static drip, day 1, 8 carboplatin AUC 2, static drip, day 1, 8day
21 days for one cycle
ET
Epirubicin 60-75mg/m2, IV, day 1 docetaxel 75mg/m2, IV, day 2 of a cycle of 21 days
Other options
CAF
Cyclophosphamide 500mg/m2 >, static drip, day 1Doxorubicin 50mg/m2, static drops, day 1
5-Fluorouracil 500mg/m< span style="font-size:10pt">2, intravenously, for the first 1, 1, 8 days
21 days for one cycle
FEC
5-Fluorouracil 500 mg/m2, intravenously, for the first 1, 8 days of epi-zolpidem 50mg/m2, static drip, first 1, 8 days
Cyclophosphamide 400mg/m2 >, static drip, day 1, 8
28 days for one cycle
AC
Doxorubicin 60mg/m2 The first day of cyclophosphamide 600mg/m2, IV, day 1 of a cycle of 21 days
EC
Epirubicin 75mg/m2 The first day of cyclophosphamide 600mg/m2, IV, day 1 of a cycle of 21 days
CMF
Cyclophosphamide 100mg/m2 >, orally, on days 1-14Methotrexate 40mg/m2, IV, day 1, 8
5-Fluorouracil 600mg/m< span style="font-size:10pt">2, intravenously, for the first 1, 1, 8 days
28 days for one cycle
Attachment 12
Definition of Menopause
Menopause is usually the permanent termination of physiological menstruation or the permanent loss of estrogen-synthesizing function of the ovaries due to breast cancer treatment. The criteria for menopause are as follows
After bilateral oophorectomy. Age ≥60 years.
Age <60 years without chemotherapy and treatment with tamoxifen, toremifene and ovarian function suppression The patient has been menopausal for 1 year or more without chemotherapy and tamoxifen, toremifene, and ovarian function suppression therapy, and has blood FSH and estradiol levels in the postmenopausal range; and is taking tamoxifen, toremifene, or taremifene for 1 year. Patients with menopause who are taking tamoxifen or toremifene and are <60 years of age must have continuous blood FSH and estradiol levels consistent with the postmenopausal range.
Also, it is important to note that
Women on LH-RH agonist or antagonist therapy cannot determine whether they are menopausal.
Women who are not menopausal before adjuvant chemotherapy, menopause cannot be used as a basis for determining menopause, because patients may stop ovulating or have no menstruation after chemotherapy, but ovarian function may still be normal or may recover.
For women with chemotherapy-induced menopause who are considering an aromatase inhibitor as endocrine therapy, effective ovarian suppression (complete bilateral ovariectomy or pharmacological suppression) or multiple consecutive monitoring of
is required. “font-family:Times New Roman”>FSH/ or estradiol levels have confirmed that the patient is in a postmenopausal state.
Annex 13
Common Treatment Options for Postoperative Adjuvant Targeted Therapy
AC→PH (P ) scheme
Doxorubicin 60 mg/m. span style=”font-size:10pt”>2 iv Day 1 of cyclophosphamide 600 mg. Roman”>600 mg/m2 iv th day 1 day 21 days for 1 cycle, for a total of < span style="font-family:Times New Roman">4 cycles Sequence
Paclitaxel 80mg/m2 iv 1 hour weekly treatment, total < span style="font-family:Times New Roman">1 cycles. /span>hour weekly therapy for 12 weeks
Trastuzumab first dose 4mg/kg iv for the first week and each subsequent trastuzumab 2mg/kg, iv per week, for a total of 1 year. It is also possible to change trastuzumab administration to 6 mg/kg iv every 3 weeks after paclitaxel chemotherapy for a total of 1 years. 1 year.
Pattuzumab 840mg iv (first dose) to 420mg iv on day 1, every 3
week, completing 1year.
ddAC→PH (P) program
Doxorubicin 60 mg/m. span style=”font-size:10pt”>2 iv Day 1 of cyclophosphamide 600 mg. Roman”>600 mg/m2 iv th day 1 day 14 days for 1 cycle, for a total of < span style="font-family:Times New Roman">4 cycles Sequence
Paclitaxel 175mg/m. span style=”font-size:10pt”>2 iv 3 h every 14 days for 1 cycle for a total of 4 weeks
period
Trastuzumab first dose 4mg/kg iv, first week, each subsequent trastuzumab dose
Anti-2mg/kg, iv weekly for 1 year. trastuzumab administration can also be changed to 6 mg/kg iv every 3 weeks to complete a total of 1 year. (All cycles are supported with G-CSF).
Pattuzumab 840mg iv (first dose) to 420mg iv on day 1, every 3
week, completing 1year.
TCH (P) program
Docetaxel 75 mg/m2 iv day 1 carboplatin AUC=6 iv day 1
21 days for 1 cycle for 6 cycles
Trastuzumab first dose 4mg/kg iv, first week, sequential trastuzumab 2mg/kg iv, weekly, or trastuzumab first dose 8mg/kg iv, first week, sequential trastuzumab 6mg/kg iv every 3 weeks for 1 years.
Pattuzumab 840mg iv (first dose) to 420mg iv on day 1, every 3
week, completing 1year.
AC→TH (P) program
Doxorubicin 60 mg/m2 iv Day 1 of cyclophosphamide 600 mg/m2 iv Day 1 21 days for 1 cycle for a total of 4 cycles Sequence
Docetaxel 100mg/m2 iv Day 1
21 days for 1 cycle, for a total of 4 cycles
Trastuzumab first dose 4mg/kg iv, week 1, and each subsequent trastuzumab dose 1.
Anti-2mg/kg for iv weekly, for a total of 11 weeks of sequential trastuzumab 6 mg/kg iv every 3
weekly to complete 1year.
Pattuzumab 840mg iv (first dose) to 420mg iv, dose 1 day, every 3 weeks, to complete 1 year.
TC4H
Docetaxel 75 mg/m2iv Part 1 day of cyclophosphamide 600 mg/m2 iv day 1 of
21 days for 1 cycle for a total of 4 cycles combined
Trastuzumab first dose 4mg/kg iv, first week 1 and each subsequent trastuzumab 2mg/kg, iv weekly for a total of 11 weeks of sequential trastuzumab 6 mg/kg iv every 3 weeks to complete 1year.
PH
Paclitaxel 80mg/m2 iv 1 hours weekly therapy for a total of 12 weeks combined
Trastuzumab first dose 4mg/kg iv, first week 1 and sequentially thereafter each trastuzumab 2mg/kg, iv weekly for 1 year. trastuzumab administration can also be changed to 6 mg/kg iv every 3 weeks for 1 years.
Attachment 14
Common Treatment Options for Targeted Therapy in Advanced HER2-positive Breast Cancer
1)HER2- positive advanced breast cancer first-line treatment regimen trastuzumab + docetaxel
Docetaxel 75 to 100 mg/m2, iv, day 1
Trastuzumab 8mg/kg (first dose) ~6mg/kg, iv day 1
21 days for 1 cycle.
Trastuzumab + docetaxel + capecitabine docetaxel 75mg/m2, iv, day 1
Capecitabine 1000mg/m2PO per day 2 doses on days 1 to 14 of trastuzumab 8mg/kg (first dose)~6mg/kg, iv, day 1 day 21 days for 1 cycle.
Trastuzumab + paclitaxel.
Paclitaxel80mg/m2, iv, 1 time per week
or 175mg/m2, iv, day 1, every 3 weeks1
Trastuzumab 4mg/kg (first dose) ~2mg/kg, iv, 1 time per week, or trastuzumab 8mg/kg (first dose) ~6mg/kg, iv, the first 1 day, and 3 weeks 1.
Trastuzumab +paclitaxel +carboplatin weekly
Paclitaxel 80mg/m2, iv, 1, 8, 15 days Kaplan AUC=2 iv, the 1, 8, 15day
Trastuzumab 4mg/kg (first dose)~2mg/kg, iv, 1 time per week
28 days for 1 cycle.
Trastuzumab +Vincristine
Vincristine 25mg/m2, iv, 1, 8, 15 days
Trastuzumab 4mg/kg (first dose)~2mg/kg, iv, weekly 1 dose per 28 days for 1 cycle.
Trastuzumab +Pattuzumab +DocetaxelDocetaxel 75-100mg/m2, iv, day 1
trastuzumab 8mg/kg (first dose) to 6mg/kg, iv, day 1 of patuximab “font-family:Times New Roman”>840mg iv (first dose) to 420mg, iv, iv, day 1 21 for day “font-family:Times New Roman”>1 cycle.
2) Other treatment regimens with trastuzumab lapatinib + capecitabine
Lapatinib 1250mg, PO< /span>, 1 dose daily, days 1 to 21 Capecitabine 1000mg/m2, PO, daily < span style="font-family:Times New Roman">2 times per day and 1 to 14 days per 21 days for 1 cycle.
Trastuzumab + lapatinib
Lapatinib 1000mg, PO< /span>, 1 time per day
Trastuzumab 4mg/kg (first dose) to 1. family:Times New Roman”>2mg/kg, iv, weekly 1times, or trastuzumab 8mg/kg (first dose) to 6mg/kg, iv, day 1, every 3 days Roman”>3 weeks 1 times.
Attachment 15
Breast Cancer Treatment Guidelines (2022 Edition) Development and Validation Expert Group
(in order of last name stroke)
Team leader: Xu Binghe
Deputy team leaders: Ma Fei and Wang Xiang
Members: Yu Tao, Wang Yongsheng, Wang Shusen, Wang Yong, Wang Shulian, Wang Jing, Fu Li, Sun Qiang, Li Guohui, Li Jing, Wu Gui, Ying Jianming, Zhang Qingyuan, Zhang Jin, Chen Jiayi, Jin Feng, Hu Xichun, Wei Wenqiang
Secretary: Li Suyi