Gastric Cancer Treatment Guide
(2022 Edition)
I. Overview
Gastric cancer is a malignant tumor of epithelial origin that originates in the stomach. According to the latest data from China in 2020, gastric cancer has the third highest incidence and mortality rate among various malignant tumors. Globally, about 1.2 million new cases of gastric cancer occur each year, of which China accounts for about
40  . The proportion of early-stage gastric cancer in China is very low, only about 20
. The proportion of early-stage gastric cancer in China is very low, only about 20 , and most of them are already in the progressive stage when detected, with an overall 5-year survival rate of less than 50. The overall 5-year survival rate is less than 50
, and most of them are already in the progressive stage when detected, with an overall 5-year survival rate of less than 50. The overall 5-year survival rate is less than 50 . In recent years, as gastroscopy has become more common, the proportion of early-stage gastric cancer has increased each year.
. In recent years, as gastroscopy has become more common, the proportion of early-stage gastric cancer has increased each year.
The overall strategy for the treatment of gastric cancer is comprehensive treatment with a surgical focus. This guideline was developed to further standardize the practice of gastric cancer treatment in China, improve the level of gastric cancer treatment in medical institutions, improve the prognosis of gastric cancer patients, and ensure medical quality and medical safety. The gastric cancer referred to in this guideline refers to gastric adenocarcinoma (hereinafter referred to as gastric cancer), including cancer of the gastroesophageal junction.
II. Diagnosis
The diagnosis and differential diagnosis of gastric cancer should be made in the context of the patient’s clinical presentation, endoscopy and histopathological and imaging examinations.
(a) Clinical manifestations.
Patients with early gastric cancer often have no specific symptoms, but as the disease progresses, symptoms similar to gastritis and ulcer disease may appear, mainly: ① epigastric fullness and discomfort or vague pain, mainly after meals; ② loss of appetite, belching, acid reflux, nausea, vomiting, black stool, etc. vomiting, black stool, etc. In addition to the above symptoms, progressive gastric cancer often presents: ① weight loss, anemia and weakness. ②Stomach pain, such as pain that continues to worsen and radiates to the lower back.
This suggests possible invasion of the pancreas and abdominal plexus. Once perforated, gastric cancer may present with symptoms of gastric perforation in the form of severe abdominal pain. (3) Nausea and vomiting, often due to tumor-induced obstruction or gastric dysfunction. Cardia cancer may cause progressive dysphagia and reflux symptoms, and sinus cancer may cause pyloric obstruction and vomiting of food. Bleeding and black stool. Tumor invading blood vessels may cause gastrointestinal bleeding. The tumor invades the blood vessels and can cause gastrointestinal bleeding. When the amount of bleeding is small, only the stool is positive for occult blood.
Other symptoms such as diarrhea (patients have accelerated gastric emptying due to lack of gastric acid), symptoms of metastases, etc. Patients with advanced disease may develop severe wasting, anemia, edema, fever, jaundice, and cachexia.
(ii) Physical signs.
Gastric cancer in general, especially early stage gastric cancer, often has no obvious signs, but patients with progressive or even advanced gastric cancer may have the following signs: (1) deep pressure pain in the upper abdomen, sometimes accompanied by a mild feeling of muscle resistance, which is often the only sign available on physical examination; (2) an epigastric mass, and in progressive gastric cancer located in the pyloric sinus or gastric body, an epigastric mass can sometimes be found. (2) upper abdominal mass, sometimes upper abdominal mass can be found in progressive gastric cancer located in the pyloric sinus or gastric body; in female patients, pushable mass can be found in the lower abdomen, and Krukenberg’s tumor should be considered; (3) manifestations of gastrointestinal obstruction: gastric pattern and tremors can be found in pyloric obstruction; small intestine or mesenteric metastasis can cause partial or complete intestinal obstruction due to narrowing of the intestinal lumen; (4) ascites sign, bloody ascites can be found in case of peritoneal metastasis; (5) enlarged supraclavicular lymph nodes; (6) anterior rectal fossa mass; (7) umbilical mass (6) swelling in the anterior rectal fossa; (7) umbilical mass, etc. Among them, enlarged lymph nodes in the supraclavicular fossa, ascites sign, lower abdominal pelvic mass, umbilical mass, anterior rectal fossa mass and intestinal obstruction are all important signs indicating advanced gastric cancer. Therefore, careful examination of these signs not only has important diagnostic value, but also provides a good clinical basis for the development of diagnostic and treatment strategies.
(iii) Imaging.
- style=”margin-left: 110pt”>
- X-ray gas-barium double contrast angiography
Localization diagnosis is better than conventional CT or MRI, which can guide clinicians in the choice of surgical approach and extent of gastrectomy.
- style=”margin-left: 110pt”>
- Ultrasound
Ultrasonography (US) is used as a routine imaging test for patients with gastric cancer because it is easy to perform, flexible and intuitive, and noninvasive without radiation. After filling the gastric cavity, conventional ultrasound can show the hierarchical structure of the gastric wall and determine the depth of infiltration, which is a useful supplement to T-staging of gastric cancer; color Doppler flow imaging can observe the blood supply in the lesion; ultrasound double imaging can observe the microcirculatory perfusion characteristics of the lesion and surrounding tissues based on the morphological characteristics of the lesion; in addition, ultrasound examination can detect metastasis of important organs and lymph nodes in the abdominopelvic cavity, and metastasis of lymph nodes in the neck and supraclavicular region. The ultrasound examination can detect the metastasis of important organs and lymph nodes in the abdominopelvic cavity and the metastasis of lymph nodes in the neck and supraclavicular region.
- style=”margin-left: 110pt”>
- CT
CT examination should be the preferred clinical staging tool, and multilayer spiral CT is widely available in China, especially recommended for combined thoracoabdominopelvic large-area scans. In the absence of contraindications to CT contrast enhancement, enhanced scans are used, and continuous scans with a layer thickness of about 1 mm are routinely used, and multiplanar reconstruction images are recommended to help determine the tumor site, the relationship between the tumor and surrounding organs (e.g., liver, pancreas, diaphragm, colon, etc.) or blood vessels, and to distinguish the tumor from local lymph nodes, improving staging confidence and accuracy. To better visualize the lesion, oral negative contrast (usually 500 to 800 ml of water orally before scanning) is recommended to fully fill the gastric cavity and dilate the gastric wall, and the supine position is routinely used for scanning.
The sensitivity of CT for progressive gastric cancer is about 65%. The sensitivity of CT for progressive gastric cancer is about 65 -90
-90  , and
, and
Early gastric cancer is about 50
: T-staging accuracy is 70 -90
-90  , N staging is
, N staging is
40  -70
-70  . Therefore, CT is not recommended as the first diagnostic method for the initial diagnosis of gastric cancer, but is recommended as the imaging method of choice for the staging of gastric cancer.
. Therefore, CT is not recommended as the first diagnostic method for the initial diagnosis of gastric cancer, but is recommended as the imaging method of choice for the staging of gastric cancer.
- style=”margin-left: 110pt”>
- MRI
Recommended for those allergic to CT contrast or for those with suspected metastases on other imaging studies.MRI is useful to determine the status of peritoneal metastases and may be used as appropriate. Enhanced MRI is the preferred or important complementary test for liver metastases from gastric cancer, especially when liver-specific contrast is injected to help diagnose and determine the number and location of metastatic lesions. MRI has good soft tissue contrast, and with the advancement of MRI scanning technology, for progressive esophagogastric cancer, CT is not able to make a clear diagnosis or the tumor is not diagnosed by plain scan. In the case of progressive esophagogastric cancer, where CT scan is not definitive, or where the tumor prevents endoscopic ultrasonography (EUS), MRI is recommended as appropriate based on the strength of the center.
- style=”margin-left: 110pt”>
- Positron Emission Computed Tomography
Positron emission tomography-computed tomography (PET-CT) can assist in the staging of gastric cancer, but is not routinely recommended. PET-CT can be used to assess the patient’s systemic condition if distant metastases are suspected on CT, and in addition, studies have shown that PET-CT is useful for radiotherapy or
Targeted therapy is also valuable for evaluating the efficacy of targeted therapy, but is not routinely recommended. In some histological types of gastric cancer, there is a negative correlation between tumor and normal tissue metabolism, such as mucinous adenocarcinoma, indolent cell carcinoma, and hypofractionated adenocarcinoma, which are usually 18F-FDG low uptake, and should be used with caution in these patients.
- style=”margin-left: 110pt”>
- Single-photon emission computed tomography
Bone scan is the most widely used, experienced, cost-effective, and sensitive method for detecting bone metastases from gastric cancer, but has a false-negative rate in the spine and lesions confined to the bone marrow, and can be combined with MRI to improve detection. Bone scan is feasible for patients with high suspicion of bone metastases.
- style=”margin-left: 110pt”>
- Tumor markers
Widely used in clinical diagnosis, and the combination of tumor markers provides us with dynamic observation of tumor development and clinical efficacy evaluation and patient prognosis, thus improving the detection rate and differential diagnostic accuracy. It is recommended that CA72-4, carcinoembryonic antigen (CEA), and CA19-9 are routinely recommended, and that methemoglobin may be further tested in some patients
(alpha-fetoprotein, AFP) and CA125, which is of diagnostic and prognostic value for peritoneal metastases and AFP for specific pathological types of gastric cancer. specific growth factor, pepsinogen
(pepsinogen, PG) I and PG II have yet to be recognized for their sensitivity and specificity. Currently, automated chemiluminescent immunoassays and their accompanying reagents are commonly used for tumor marker detection.
- style=”margin-left: 110pt”>
-
Gastroscopy
- Screening.
- Screening.
- style=”margin-left: 62pt”>
-
Screening target: Stomach cancer has a low incidence in the general population (33/100,000) The incidence rate of gastric cancer in the general population is low (33/100,000), and endoscopy for gastric cancer screening requires a large amount of human and material resources and low patient acceptance. Therefore, only screening for people at high risk of gastric cancer is a potentially effective method. In China, it is recommended that people over 40 years of age or those with a family history of gastric cancer should be screened for gastric cancer. Those who meet any of the following items 1 and 2-6 should be classified as the high-risk group for gastric cancer and are recommended to be screened: 1) age 40 years or older, regardless of gender; 2) population in areas with high incidence of gastric cancer; 3) H. pylori infection; 4) previous pre-cancerous gastric diseases such as chronic atrophic gastritis, gastric ulcer, gastric polyp, post-surgical residual stomach, hypertrophic gastritis, pernicious anemia; 5) first-degree relatives of gastric cancer patients; 6) presence of other high-risk factors for gastric cancer (high salt, pickled diet, smoking, heavy alcohol consumption, etc.).
- style=”margin-left: 56pt”>
- Screening method: see Figure 1.
Serum PG test: The screening of gastric cancer in China uses a PGⅠ concentration of ≤70 μg/L and a PGⅠ/PGⅡ≤3.0 as the standard for the high-grade population of gastric cancer. The risk of gastric cancer was stratified based on the results of serum PG testing and H. pylori antibody testing, and further screening strategies were determined.
Gastrin 17 (G-17): Serum G-17 concentration testing can diagnose atrophic gastritis in the gastric sinus (reduced G-17 levels) or confined to the gastric body (elevated G-17 levels).
Barium meal of the upper gastrointestinal tract: Barium x-ray may detect gastric lesions, but is not as sensitive or specific and has been replaced by endoscopy, which is not recommended for gastric cancer screening.
Endoscopic screening: endoscopy and endoscopic biopsy are the current gold standard for the diagnosis of gastric cancer.
- Screening method: see Figure 1.
In recent years, painless gastroscopy has developed rapidly and has been applied to endoscopic screening for people at high risk for gastric cancer, greatly improving patient acceptance of gastroscopy.
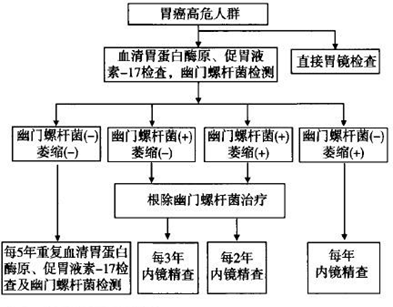
Figure 1 Stomach Cancer Screening Methods
- style=”margin-left: 134pt”>
- Endoscopy Technique
- style=”margin-left: 62pt”>
-
Plain white light endoscopy. Plain white light endoscopy is the basis of endoscopic techniques, where the lesion or suspected lesion area is first observed with white light endoscopy to document the natural state of the lesion area before proceeding to other endoscopic techniques.
-
Chemical staining endoscopy: Chemical staining endoscopy is based on conventional endoscopy in which a pigmented dye is sprayed onto the mucosal surface to be observed. The mucosal surface to be observed is sprayed with pigment dye to make the contrast between the lesion and the normal mucosa more obvious. Physical staining (indigo carmine, methylene blue): the relationship between the dye and the lesion is physical coverage, as the microstructure of the lesion surface is different from the surrounding normal mucosa, the dye coverage produces a different reflection of light, thus highlighting the
The boundary between the lesion area and the surrounding normal tissue. Chemical staining (acetic acid, epinephrine): refers to the chemical reaction between the dye and the lesion area, which changes the color of the lesion area and highlights the lesion border.
- style=”margin-left: 62pt”>
-
Electron staining endoscopy: electron staining endoscopy allows clear visualization of the superficial mucosa with special light.
- Magnification endoscopy: Magnification endoscopy can magnify the gastric mucosa and observe the small concave structures on the surface of the gastric mucosal glands and the subtle changes in the morphological characteristics of the mucosal microvascular network, which can be used to identify the benignity and malignancy of gastric mucosal lesions and to determine the boundary and the malignant lesions. The boundary and extent of malignant lesions.
- EUS: EUS is an endoscopic technique that combines ultrasound technology with endoscopic technology. It is used to assess the extent of gastric cancer invasion and lymph node status.
-
Other Endoscopic Techniques: Laser Confocal Microendoscopy: Displays microscopic structures that can be magnified up to 1000 times for the purpose of optical biopsy. Fluorescence endoscopy: an endoscopic imaging system based on fluorescence can detect and identify precancerous lesions and some occult malignant lesions that are difficult to detect by ordinary endoscopy. However, the above methods require high equipment requirements and are still less routinely promoted in clinical practice.
-
Gastroscopy Guideline: Gastroscopy is a necessary tool to confirm the diagnosis of gastric cancer, to determine the location of the tumor, and to obtain tissue specimens for pathology. It can determine the location of the tumor and obtain tissue specimens for pathological examination. Adequate preparation is necessary before endoscopy, and the application of debulking agents and demulcent agents is recommended. After transoral insertion, the endoscope is inserted directly into the lumen from the upper esophagus to observe the esophagus, cardia, gastric body, gastric sinus, pylorus, duodenal bulb and duodenal descending part in turn. When exiting the scope, the scope was passed through the duodenum, gastric sinus, gastric angle, gastric body, fundus cardia, and esophagus. In order to fully observe, apply the rotating body and flexing end of the mirror
and inversion of the mirror to observe the entire upper gastrointestinal tract, especially the greater and lesser curves, anterior and posterior walls of the gastric wall, and to observe the mucosal color, smoothness, mucus, peristalsis, and endoscopy. The mucous membrane color, smoothness, mucus, peristalsis and the shape of the internal cavity were observed. If a lesion is found, the specific location and extent of the lesion should be determined and recorded in detail on the record sheet. If mucus and air bubbles are present during the examination, they should be flushed with water or de-foaming and de-mucolytic agents in a timely manner before continuing observation. To ensure complete observation of the entire gastric cavity, additional images should be kept if lesions are found. At the same time, the clarity of each image should be ensured. A minimum of 40 images is recommended by national experts. Image enhancement techniques such as pigmented endoscopy/electronic staining endoscopy or magnification endoscopy may be used if necessary and appropriate.
- style=”margin-left: 134pt”>
- Endoscopic staging of early gastric cancer: see Figure 2.
1) Endoscopic staging of early gastric cancer according to the 2002 Paris staging criteria and
Update of Paris staging criteria in 2005. Superficial gastric cancer (Type 0) is divided into elevated lesions (0-Ⅰ), flat lesions (0-Ⅱ), and depressed lesions (0-Ⅲ). Type 0-Ⅰ is subdivided into tipped (0-Ⅰp) and untipped (0-Ⅰs) types. type 0-Ⅱ is divided into 3 subtypes, 0-Ⅱa, 0-Ⅱb, and 0-Ⅱc, based on the slight elevation, flatness, and slight depression of the lesion.
2) Type 0-Ⅰ and type 0-Ⅱa are defined by an elevation height of 2.5 mm (biopsy clamp closure thickness), and type 0-Ⅲ and type 0-Ⅱc are defined by a depression depth of
- style=”margin-left: 62pt”>
-
mm (biopsy forceps open individual forceps thickness). Lesions with both slight elevation and slight depression were classified into 0-IIc+IIa and 0-IIa+IIc types according to the elevation/depression ratio. Lesions with a combination of augmentation and slight depression were then classified into 0-III+IIc and 0-IIc+III types according to the augmentation/slight depression ratio.

Figure 2 Microscopic staging of gastric cancer schematic diagram
3) The flow of the refined investigation and follow-up of early gastric cancer is shown in Figure 3.
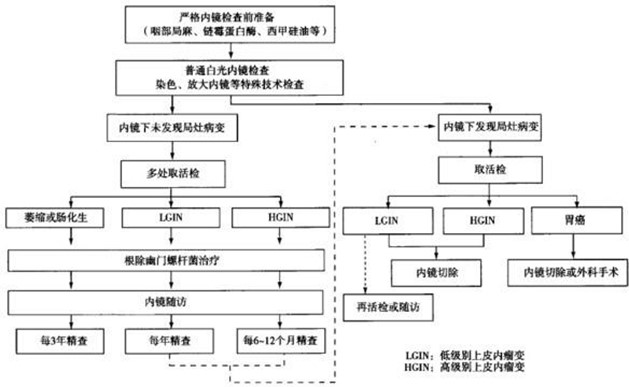
Figure 3 Gastric Cancer Precise investigation and follow-up process
- style=”margin-left: 134pt”>
- Biopsy pathology examination.
- style=”margin-left: 118pt”>
- If special endoscopic techniques such as endoscopic observation and staining reveal no detectable
Suspicious lesions may be removed without biopsy.
- style=”margin-left: 62pt”>
-
Biopsy site: In order to improve the positive biopsy rate, attention should be paid to the selection of biopsy site when taking biopsy for different types of lesions.
1) Tender lesions: Biopsies should be taken from the head of the lesion, not the tip of the lesion.
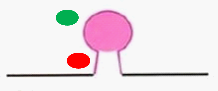
②Bulbar lesions: should be biopsied at the top of the lesion, not the base of the lesion
The lesion should be biopsied at the top of the lesion, not at the base.

 ③ Ulcerative lesions: should be biopsied on the medial side of the ulcerative dike, not the base of the ulcer or the lateral side of the ulcerative dike.
③ Ulcerative lesions: should be biopsied on the medial side of the ulcerative dike, not the base of the ulcer or the lateral side of the ulcerative dike.
 < span style="font-family:Times New Roman; font-size:10pt">
< span style="font-family:Times New Roman; font-size:10pt">
Appropriate biopsy site  Inappropriate biopsy site
Inappropriate biopsy site
- style=”margin-left: 62pt”>
-
Suspected early-stage neoplastic lesions: 1 to 2 biopsies for lesions less than 2 cm in diameter, with 1 additional biopsy for each additional 1 cm in diameter; tendency to progress For gastric mucosa with a tendency to progress, 6 to 8 pieces were taken avoiding necrotic areas.
- style=”margin-left: 56pt”>
- Guidelines for handling gastroscopic biopsy specimens.
1) Specimen pre-processing: Immediately after the biopsy specimen is removed from the body, the specimen is flattened so that the basal level of the mucosa adheres to the filter paper.
- Guidelines for handling gastroscopic biopsy specimens.
② Specimen fixation: Place the specimen in an adequate (>10x specimen volume) 10 
Neutral Buffered Formalin Solution (with 4 
formaldehyde). The fixation time before embedding must be
greater than 6 hours and less than 48 hours.
③ Paraffin embedding: Remove the filter paper and embed the tissue in a vertical orientation. When embedding, the burned forceps should not directly touch the specimen, and the wax surface should be de-heated before clamping the tissue to prevent burns to the tissue.
4) Hematoxylin and eosin (HE) staining standard: trim the wax block, cut 6 to 8 consecutive tissue surfaces, and retrieve them on the same slide. Routine HE staining and sealing.
- style=”margin-left: 110pt”>
- EUS
EUS is considered the most accurate method for local staging of gastrointestinal tumors, and is as good as or better than CT in T-stage (especially early-stage cancer) and N-stage of gastric cancer, and is often used to distinguish between mucosal and submucosal lesions, to dynamically observe the relationship between the tumor and adjacent organs, and to significantly improve local T- and N-staging by EUS-guided puncture biopsy of lymph nodes. However, EUS is an operator-dependent test and is therefore recommended in hospitals or centers with high medical standards. For the proposed endoscopic mucosal resection
changes with blurred borders and uniform internal echogenicity.
Guidelines for ultrasound gastroscopy: a standardized procedure and a comprehensive, unobstructed scan are the basis for accurate staging. For accurate assessment of the first lymph node, retraction from the duodenal bulb is recommended. Staging should be performed during retrieval and images of typical tumors and important anatomic landmarks should be retained, if possible with dynamic multimedia data to improve staging accuracy and provide retrospective possibilities. The scanning process should pay attention to the filling of the gastric cavity and to the selection of the appropriate probe frequency and proper probe placement, with clearer images at the appropriate focal length and avoiding compression of the lesion leading to incorrect staging.
(D) Diagnostic criteria and content of gastric cancer.
- style=”margin-left: 110pt”>
- Qualitative diagnosis
Gastroscopy with biopsy of the lesion and pathological examination should be used to determine whether the lesion is cancerous, the degree of differentiation of the tumor and the expression of specific molecules, and other properties and characteristics closely related to the nature and biobehavioral characteristics of gastric cancer itself. In addition to the conventional histological types, the Laurén typing and HER2 expression status should be clarified.
- style=”margin-left: 110pt”>
- Staging diagnosis
The main purpose of the staging of gastric cancer is to understand the severity and characteristics of the disease prior to the development of a treatment plan, in order to provide an adequate basis for selecting a reasonable treatment modality. The severity of gastric cancer can be focused on the depth of local infiltration, the degree of lymph node metastasis, and the presence or absence of distant metastasis, and appropriate ancillary tests should be selected to obtain a more accurate staging in clinical practice.
Diagnostic information.
- style=”margin-left: 110pt”>
- Clinical manifestations
Clinical manifestations are not the primary basis for the diagnosis of gastric cancer, but the presence of comorbidities and concomitant diseases should be fully considered in the development of a treatment strategy that will impact the overall treatment measures.
(v) Differential diagnosis.
- style=”margin-left: 110pt”>
- Benign gastric ulcer
In contrast to gastric cancer, benign gastric ulcers generally have a longer duration, have a history of recurrent painful typical ulcers, are effectively treated with antacids, and are not associated with loss of appetite. Unless combined with bleeding, pyloric obstruction and other serious comorbidities, there are no obvious signs, no recent significant weight loss, anemia, abdominal mass or even enlarged lymph nodes in the left supraclavicular fossa. More importantly, on barium X-ray and gastroscopy, benign ulcers are often less than 2.5 cm in diameter, with round or oval niches, neat margins, and peristaltic waves passing through the lesion; gastroscopy reveals a flat mucosal base, covered with white or yellowish-white moss, with edema and congestion of the surrounding mucosa and concentration of mucosal folds towards the ulcer. In contrast, cancerous ulcers are very different from this; see the section on diagnosis of gastric cancer for detailed features.
- style=”margin-left: 110pt”>
- Gastric lymphoma
Accounting for 2 of gastric malignancies -7
-7  . 95 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0941_202223.png" alt=""/>The primary malignant lymphoma of the stomach above is non-Hodgkin’s lymphoma, which often extensively infiltrates the stomach wall and forms a large shallow ulcer. Upper abdominal discomfort, gastrointestinal bleeding and abdominal masses are the main clinical manifestations.
. 95 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0941_202223.png" alt=""/>The primary malignant lymphoma of the stomach above is non-Hodgkin’s lymphoma, which often extensively infiltrates the stomach wall and forms a large shallow ulcer. Upper abdominal discomfort, gastrointestinal bleeding and abdominal masses are the main clinical manifestations.
- style=”margin-left: 110pt”>
- Interstitial tumor of the gastrointestinal tract
Mesenchymal-derived tumors, which account for about 3 , the tumor grows distensibly and may infiltrate submucosa or subplasma to form spherical or lobulated masses. Tumor microsomia
, the tumor grows distensibly and may infiltrate submucosa or subplasma to form spherical or lobulated masses. Tumor microsomia
The symptoms are not obvious and may include epigastric discomfort or ulcer-like gastrointestinal symptoms, while in larger tumors, an abdominal mass may be palpable, often with signs of upper gastrointestinal bleeding.
- style=”margin-left: 110pt”>
- Gastric neuroendocrine tumor
Neuroendocrine neoplasm (NEN) is a heterogeneous group of tumors that originate from peptidergic neurons and neuroendocrine cells, all of which have malignant potential. These tumors are characterized by the ability to store and secrete different peptides and neuramines. Although gastroenteropancreatic NEN is a rare disease, accounting for less than 2 of gastrointestinal malignancies, NEN is currently the most prevalent tumor in the United States. NEN is now the second most prevalent gastrointestinal malignancy after colorectal cancer in the United States. The diagnosis of NEN is still based on histological biopsy pathology as the gold standard, but conventional HE staining is no longer sufficient to adequately diagnose NEN, and immunohistochemical staining for synaptophysin and chromogranin A is now mandatory for the diagnosis of NEN, and NEN needs to be graded according to nuclear schizophrenia and Ki-67 percentage.
of gastrointestinal malignancies, NEN is currently the most prevalent tumor in the United States. NEN is now the second most prevalent gastrointestinal malignancy after colorectal cancer in the United States. The diagnosis of NEN is still based on histological biopsy pathology as the gold standard, but conventional HE staining is no longer sufficient to adequately diagnose NEN, and immunohistochemical staining for synaptophysin and chromogranin A is now mandatory for the diagnosis of NEN, and NEN needs to be graded according to nuclear schizophrenia and Ki-67 percentage.
- style=”margin-left: 110pt”>
- Benign tumors of the stomach
About 2 percent of all gastric tumors The tumors can be divided into epithelial cell tumors and mesenchymal histomas according to their tissue origin, with the former commonly being gastric adenomas and the latter being more common as smooth muscle tumors, lipomas, and nerve sheath tumors. They are generally small in size and develop slowly. Gastric sinus and body are the most frequent sites. It is mostly without obvious clinical manifestations. Barium x-ray is a round or oval filling defect rather than a niche; gastroscopy shows a submucosal mass.
The tumors can be divided into epithelial cell tumors and mesenchymal histomas according to their tissue origin, with the former commonly being gastric adenomas and the latter being more common as smooth muscle tumors, lipomas, and nerve sheath tumors. They are generally small in size and develop slowly. Gastric sinus and body are the most frequent sites. It is mostly without obvious clinical manifestations. Barium x-ray is a round or oval filling defect rather than a niche; gastroscopy shows a submucosal mass.
(a) Terms and definitions.
Malignant tumors derived from epithelial cells of the gastric mucosa. 2.
Pre-cancerous lesions of gastric cancer, 2 terms intraepithelial neoplasia and heterogeneous hyperplasia can be used to refer to
Used. There are 3 diagnoses involving gastric intraepithelial neoplasia/heterozygosis.
- style=”margin-left: 62pt”>
- No intraepithelial neoplasia (heterogeneous hyperplasia): benign lesions such as inflammation, chemosis, and reactive hyperplasia of the gastric mucosa.
-
Indeterminate intraepithelial neoplasia (heterogeneous hyperplasia): not a final diagnostic term, but used when it is difficult to determine the nature of tissue and cellular changes in the gastric mucosa. A pragmatic description used when it is difficult to determine the nature of morphologic changes in gastric mucosal tissue and cells. It is often used in small biopsy specimens, especially those with a clear inflammatory background, when it is difficult to distinguish the nature of lesions (e.g., reactive or proliferative lesions) such as epithelial hyperplasia of the gastric notch located in the hyperplastic zone of the mucosal neck region and epithelial hyperplasia of the intestinal epithelium in the area of chemosis. In such cases, the diagnosis can be clarified by deep cuts and retrieval of material.
- Intraepithelial neoplasia (heterogeneous hyperplasia): epithelial hyperplasia of the gastric mucosa characterized by the presence of varying degrees of cellular and structural heterogeneity that is neoplastic in nature but without clear evidence of infiltrative growth. The lesion involves the entire length of the lesser concavity, including the surface epithelium, which is an important basis for diagnosis. Based on histological and cytological features, gastric intraepithelial neoplasia (heterogeneous hyperplasia) can be divided into two types: adenomatous (intestinal type) and lesser concave or pyloric type (gastric type). On gross examination, gastric mucosal intraepithelial neoplasia (heterogeneous hyperplasia) can be polypoid, flattened or mildly indurated in growth. Depending on the extent of the lesion, gastric mucosal intraepithelial neoplasia (heterogeneous hyperplasia) is classified as low-grade or high-grade grade 2.
- style=”margin-left: 62pt”>
-
Low-grade intraepithelial neoplasia: minor structural changes in the mucosa; mild to moderate heterogeneity of the glandular epithelium with elongated but still polar nuclei located at the base of the glandular epithelium; nuclear division is seen. For polypoid lesions, low-grade adenomas may also be used.
-
High-grade intraepithelial neoplasia: marked heterogeneity of mucosal glandular structure; cells change from columnar to rectangular, with large nuclei and a larger nucleoplasmic ratio than the nucleus. The nucleus is large, the nucleoplasm ratio is increased, and the nucleolus is obvious; nuclear schizophrenia is increased and pathological nuclear division is seen. Of particular importance are the extension of the nucleus to the lateral aspect of the gland lumen and the loss of cell polarity. For polypoid lesions, high-grade adenomas may also be used.
Invasive carcinoma confined to the mucosa or submucosa, with or without lymph node metastasis.
Cancerous tissue invading the intrinsic musculature or deeper, with or without lymph node metastasis. 5.
Esophagogastric junction adenocarcinoma is an adenocarcinoma that spans the esophagogastric junction. Anatomically, the esophagogastric junction is the site where the tubular esophagus becomes the cystic stomach, i.e., the end of the esophagus and the beginning of the stomach, corresponding to the level of the peritoneal reflex or the Hitchcock angle or the lower edge of the esophageal sphincter, which does not necessarily coincide with the histologic squamocolumnar junction.
(ii) Specimen type and fixation.
The common specimen types used in daily practice include: endoscopic biopsy specimens, EMR/ESD, palliative/radical resection specimens (proximal gastrectomy specimens, distal gastrectomy specimens, and distal gastrectomy specimens). The following types of specimens are commonly used in daily practice: endoscopic biopsies, EMR/ESD, palliative/radical resection specimens (proximal gastrectomy specimens, distal gastrectomy specimens, and total gastrectomy specimens).
- style=”margin-left: 110pt”>
-
- The specimen should be fixed promptly and adequately with 10
 Neutral buffered formalin fixation
Neutral buffered formalin fixation
- The specimen should be fixed promptly and adequately with 10
Fixing solution (with 4  formaldehyde) should be fixed immediately (also within half an hour for surgically excised specimens if possible), the fixative should be more than 10 times the volume of the specimen, the fixation time should be 6 to 72 hours, and the fixation temperature should be normal room temperature.
formaldehyde) should be fixed immediately (also within half an hour for surgically excised specimens if possible), the fixative should be more than 10 times the volume of the specimen, the fixation time should be 6 to 72 hours, and the fixation temperature should be normal room temperature.
- style=”margin-left: 62pt”>
- Endoscopic biopsy specimens: after specimen isolation, the tissue should be immediately removed from the biopsy forceps by the endoscopist or assistant with a small toggle needle and should be Spread it flat, take a small piece of filter paper, put the spread mucosa flat on the filter paper, and immediately put it into fixative to fix it.
-
EMR/ESD specimen: The specimen should be spread by the endoscopist with the mucosa facing upward and fixed with a non-rusting fine steel needle on a cork board (or foam board). The specimen should be fixed on a cork board (or foam board) with a non-rusting fine steel needle to avoid excessive stretching that may distort the specimen and should not be wrinkled, and marked in the oral and anal directions, and immediately immersed completely in fixative.
-
Radical resection specimen: usually the gastric wall is opened along the greater curvature of the stomach, or if the tumor is located in the greater curvature, the gastric wall is opened along the greater curvature avoiding the tumor, with the mucosa facing upward, and fixed on a cork board (or foam board) using a large-headed needle. (If the tumor is located in the greater curvature, open the gastric wall along the greater curvature avoiding the tumor, with the mucosa facing upward, and use a large-headed needle fixed to a cork board (or foam board) with gauze on the board.
(iii) Guidelines for obtaining materials and general description.
At the time of pickup, basic information should be verified, such as name, sending department, bed number, hospitalization number, specimen type, quantity, etc.
- style=”margin-left: 110pt”>
- style=”margin-left: 62pt”>
-
Take: All mucosa should be taken, and the mucosa should be wrapped in filter paper to avoid loss, and eosin should be added drop by drop to facilitate identification by the technician during embedding and sectioning. The different sizes should be separated into different dehydration boxes to prevent small pieces of biopsy tissue from being missed or over-cut. When embedding, attention should be paid to the need to bury the flattened mucosa in a vertical position.
(i.e., the mucosa is embedded perpendicular to the bottom surface of the cassette). The number of tissue slices in a wax block should not exceed 3 slices, and the block should be embedded in a parallel direction. The edge of the wax block should not contain a white border of tissue as much as possible.
Remove with a knife, recommending 6-8 consecutive tissue slices per slide for continuous observation.
- style=”margin-left: 48pt”>
-
- Grand body examination and documentation: Measure and record specimen size (maximum diameter)
- Grand body examination and documentation: Measure and record specimen size (maximum diameter)
×minimum diameter×thickness), and the length and width of the esophagus and stomach should be measured separately for specimens from the esophagogastric junction. The color of the mucosal surface, the presence of obvious lesions visible to the naked eye, the regularity of the contour of the lesions, the presence of obvious elevations or depressions, the presence of erosions or ulcers, etc. The size of the lesions (maximum diameter × minimum diameter × thickness), the general typing (see Appendix), and the distance of the lesions from each cut edge (at least the closest distance between the lesions and the lateral mucosal cut edge) are recorded. Clinicopathologic communication or schematic drawings of specimen extension and reconstruction by the surgeon are recommended for complex specimens.
-
- Taking: EMR/ESD specimens should be taken in their entirety. Take the specimen perpendicular to the nearest lateral cut edge. The lateral and basal mucosal margins can be marked with ink or carbon ink.
(different colors can be applied to the oral and anal sides for easy identification if available) to allow localization of the margins for microscopic observation and evaluation of the tumor margins. The specimen of esophagogastric junction should be taken in the direction of oral-anal side to better show the relationship between the tumor and esophagogastric junction. The specimens should be taken at 2-3 mm intervals in parallel, and all the specimens should be taken. If the specimen is too large, it can be reshaped by dividing 1 strip into multiple strips and marking a, b, etc. respectively. Embedding is done in the same direction (embedding the cut surface of the first and last block, and then flipping 180° if the first and last blocks have lesions under the microscope to ensure that the final section is observed around the cut edge of the mucosa), and the order/site of embedding corresponding to the tissue block is recorded. Record the site corresponding to the tissue block
(it is recommended to attach photos or schematics and mark them well). It is recommended that multiple resected specimens be numbered and taken separately, without consideration of the lateral cut margin, otherwise as for single resected specimens.
- style=”margin-left: 62pt”>
- Grand body examination and documentation: The pylorus and cardia should be correctly positioned according to their characteristics. Measure the length of the greater and lesser curves of the stomach and the volume of the gastric omentum; examine the mucosal surface, which should describe the site, size of the tumor (for specimens after neoadjuvant therapy, measure the size of the tumor bed; for specimens after endoscopic mucosal resection, describe the size of the ulcer/mucosal defect area/scar and the presence or absence of tumor remnants), number, gross staging (see Appendix), appearance description, depth of infiltration, extent of infiltration, and the distance between the tumor and the incisional margin on both sides and the circumferential The distance between the tumor and the cutting edge on both sides and the circumferential cutting edge. The mucosa of the gastric wall other than the tumor should be observed for other changes such as congestion, hemorrhage, ulceration, perforation, etc.; the plasma membrane surface should be observed for congestion, hemorrhage, exudation, perforation, tumor infiltration, etc.; the gastric wall around the tumor should be observed for thickening and elasticity; if there is another delivered spleen, duodenum, etc., they should be described in turn. Proximal
Gastric cancer suggested to report the relationship with esophagogastric junction: involvement/non-involvement of esophagogastric junction (relationship between tumor and esophagogastric junction: tumor located completely in esophagus, not involving esophagogastric junction; tumor center located in distal esophagus, involving esophagogastric junction The tumor center is located in the esophagogastric junction; the tumor center is located in the proximal stomach and involves the esophagogastric junction). If the esophagogastric junction was involved, the distance (in cm) of the tumor center from the esophagogastric junction was recorded (for Siewert typing, see Appendix). The relationship to the duodenum is recommended for distal gastric cancer.
- style=”margin-left: 62pt”>
- Taking: A strip of tissue can be taken from the center of the tumor from the oro-lateral incision margin to the anal incision margin (including the tumor, parietal mucosa, and both ends of the incision margin), and the orientation of the tissue block is recorded. The orientation of the block should be recorded (photos or diagrams should be attached and marked). It is recommended to take the relationship between the two ends of the cut edge and the tumor longitudinally, or to take the two ends of the cut edge transversely if the tumor is far from the two ends of the cut edge. If the tumor is distant from the two margins, the two margins can also be taken transversely. The closed edges of the occluders should be removed for observation. The deepest tumor invasion and suspected circumferential margin involvement should be taken. For early stage carcinoma or radical surgery specimens with inconspicuous lesions after neoadjuvant therapy, it is recommended that all the suspicious lesions and the tumor bed should be sampled. The surrounding mucous membrane should be taken separately for areas of erosion, roughness, congestion, hemorrhage, ulceration, or perforation, or for nodules in the surrounding esophagus/gastric wall and the esophagogastric junction. If other adjacent organs are present, they should be observed. The lymph nodes should be taken as grouped by the surgeon. If the surgeon does not send the grouped lymph nodes, the perigastric lymph nodes should be grouped according to the area of lymph node drainage. The number and size of the lymph nodes should be described, whether they are fused or not, whether they are adherent to the surrounding tissue, and if so, the connective tissue surrounding the lymph nodes should be noted. All detected lymph nodes should be sampled. Radical treatment without neoadjuvant therapy
A minimum of 16 lymph nodes, preferably more than 30 lymph nodes, should be detected in the specimen. The recommended tissue size is no larger than 2.0cm x 1.5cm x 0.3cm.
(iv) Pathologic diagnostic staging, grading, and staging scheme.
- style=”margin-left: 62pt”>
-
Histologic staging (see Appendix): both WHO (gastrointestinal tumors) and Laurén staging are recommended ( intestinal, diffuse, mixed, unstaged).
- style=”margin-left: 48pt”>
- Histologic grading
The glands were classified as highly differentiated, moderately differentiated, and poorly differentiated (high grade, low grade) based on their degree of differentiation.
- style=”margin-left: 48pt”>
- Staging of gastric cancer
Recommend the American Joint Committee on Cancer (AJCC) and the Union for International Cancer Control (UICC) jointly developed staging.
- style=”margin-left: 48pt”>
- Pathologic evaluation of radical surgery specimens after neoadjuvant therapy
The basic features of pathological changes after neoadjuvant therapy include tumor cell regression and regression, extensive necrosis, fibrous tissue proliferation, interstitial inflammatory cell infiltration, and calcium salt deposition. Large cell-free mucus lakes may appear, which cannot be considered as tumor remnants. It is appropriate to use the criteria of the College of American Pathologists/The National Comprehensive Cancer Network (NCCN) guidelines for grading the efficacy of gastric cancer (see Appendix).
(v) Pathology report content and guidelines.
The pathology report of gastric cancer should include all elements relevant to patient treatment and prognosis, such as specimen type, tumor site, gross staging, size and number, histologic type, subtype and grade, depth of infiltration, vascular and nerve invasion, peripheral
- Histologic grading
mucosal condition, lymph node condition, circumferential and bifurcation margin condition, etc. The recommended report ends with the pTNM staging.
- style=”margin-left: 62pt”>
- General description: including specimen type, tumor site, general staging, size (tumor size should be measured in three dimensions) and number.
-
Subject tumor: histologic type and grading, Laurén’s staging (intestinal, diffuse, mixed, or indeterminate), depth of infiltration (including intramucosal, myxomucosal, submucosal, superficial myxomucosal, deep myxomucosal, and subplasmic) The infiltration depth (including lamina propria, myxomucosa, submucosa, superficial myxomucosa, deep myxomucosa, subplasma layer, plasma layer and surrounding tissues or organs. For submucosal invasive carcinoma, the depth of submucosal infiltration should be measured for endoscopic resection specimens, and it is recommended to differentiate between SM1 (depth of submucosal invasion<500 μm) and SM2 (depth of submucosal invasion>500 μm); for radical resection specimens, it is recommended to differentiate between SM1 (upper 1/3 of submucosa), SM2 (middle 1/3 of submucosa), and SM3 (lower 1/3 of submucosa), and SM3 (lower 1/3 of submucosa). submucosal layer lower 1/3), margins (endoscopic resection specimens include lateral and basal margins, radical resection specimens include oro-lateral and anal margins and circumferential margins; the condition of the margins should be described, including invasive carcinoma or intraepithelial neoplasia/heterogeneous hyperplasia; the distance from the margins is recommended), lymphovascular/vascular infiltration (especially for endoscopic resection specimens, if lymphovascular/vascular infiltration is suspected, it is recommended to do Immunohistochemistry CD31/CD34, D2-40 to determine the presence of lymphovascular/vascular infiltration; EVG staining to determine the presence of venous invasion), and nerve invasion. Ulcerative lesions or ulcer scarring of the stomach can influence EMR/ESD surgery and determination of prognosis and is an important element of the pathology report.
- style=”margin-left: 48pt”>
- Paraneoplastic: intraepithelial neoplasia/heterogeneous hyperplasia and extent, presence of gastritis and class
- Paraneoplastic: intraepithelial neoplasia/heterogeneous hyperplasia and extent, presence of gastritis and class
type.
- style=”margin-left: 110pt”>
- Lymph node metastasis: number of metastatic lymph nodes/total number of lymph nodes. It is appropriate to report
Number of metastatic cancer invading lymph nodes outside the tegument.
- style=”margin-left: 110pt”>
- Response to treatment (in cases of neoadjuvant therapy).
- Other lesions in combination should be reported.
- style=”margin-left: 62pt”>
-
Gastric adenocarcinoma and esophagogastric The immunohistochemical detection of HER2 and mismatch repair proteins (MLH1, PMS2, MSH2, MSH6) and/or MSI should be done for adenocarcinoma of the junction. PD-L1 testing should be performed in units where available.
-
Remarked reports include significant relevant medical history (e.g., relevant tumor history and neoadjuvant therapy history).
- style=”margin-left: 48pt”>
- pTNM staging.
(F) Several issues in endoscopic resection pathology report.
- pTNM staging.
- Depth of tumor invasion: The depth of tumor invasion is determined based on the premise of negative vertical margins, and the depth of submucosal infiltration is also one of the important indicators to determine whether the lesion is completely resected. The deeper the invasion of the submucosa, the higher the possibility of lymph node metastasis. The depth of submucosal infiltration is measured according to the degree of destruction of the mucosal muscle layer within the tumor tissue. If residual mucosal muscle layer is still visible in the tumor tissue, the distance to the infiltrative front of the tumor is measured using the lower edge of the residual mucosal muscle layer as the reference. If there is no mucosal muscle layer in the tumor tissue, the distance to the front of tumor infiltration is measured from the most superficial surface of the tumor.
-
Cutting edge condition: electrocautery changes in the tissue specimen are an indication of the cutting edge of the ESD specimen. Negative margins are the absence of tumor cells in all horizontal or vertical electrocautery margins of the resected tissue. Negative cut margins, but the cancer foci are close to the cut margins, the distance between the cancer foci and the nearest cut margin should be recorded; positive horizontal cut margins, the number of blocks of positive cut margins should be recorded.
For positive vertical margins, the location of the tumor cells should be recorded (lamina propria or submucosa ). The changes in the electrocautery margin can have an impact on the observation of the tissue structure, the morphology of the cells and their nuclei, and if necessary, immunohistochemical staining can be done to help determine whether there are cancer foci remaining in the margin.
- style=”margin-left: 62pt”>
- Vascular invasion: The presence of lymphatic vessels and vascular (veins) invasion in ESD specimens is an important factor in assessing the need for surgical treatment. The deeper the tumor invasion, the more attention should be paid to the condition of vascular invasion. Special staining or immunohistochemical staining (e.g., CD31/CD34, D2-40) of tumor tissue with submucosal infiltration often reveals vascular invasion that is easily overlooked in HE staining.
-
The presence of ulcers and other lesions of the mucosa: ulcers or ulcer scarring of the stomach can influence ESD surgery and the determination of prognosis and is An important element of the pathology report. The non-neoplastic lesions of the surrounding mucosa, including inflammatory, atrophic, and septic changes and their severity, should also be documented.
-
pT1 hypofractionated carcinoma, vascular invasion, and positive cut margins should be re-surgically expanded. In other cases, endoscopic resection is sufficient, but regular postoperative follow-up is required.
- Histologic features of poor prognosis include: hypodifferentiation, vascular and lymphovascular infiltration, and positive cut margins.
-
Positive cut margins were defined as tumor less than 1 mm from the cut margin or cancer cells visible at the electric/ultrasound knife cut margin.
IV.
(a) Principles of treatment.
The principle of comprehensive treatment should be adopted, that is, according to the tumor pathological type and clinical stage, combined with the patient’s general condition and organ functional status, the multidisciplinary team (MDT) model should be adopted. The MDT model (including gastrointestinal surgery, gastroenterology, medical oncology, endoscopy center, radiotherapy, intervention, imaging, rehabilitation, nutrition, molecular biologists, bioinformaticians, etc.) should be applied in a planned and rational manner to achieve radical or maximum tumor control, prolong patient survival, and improve quality of life.
- style=”margin-left: 62pt”>
- Early gastric cancer without evidence of lymph node metastasis can be considered for endoscopic treatment or surgery depending on the depth of tumor invasion, without adjuvant radiotherapy or chemotherapy after surgery.
-
Locally progressive gastric cancer or early gastric cancer with lymph node metastasis should be treated with a combination of mainly surgery. Depending on the depth of tumor invasion and whether it is accompanied by lymph node metastasis, direct radical surgery or preoperative neoadjuvant chemotherapy can be considered before radical surgery. For locally progressive gastric cancer with successful radical surgery, adjuvant treatment (adjuvant chemotherapy and, if necessary, adjuvant chemoradiotherapy) should be decided according to the postoperative pathological stage.
-
Recurrent/metastatic gastric cancer should be treated with a combination of drug-based therapy, palliative surgery, radiotherapy, interventional therapy, radiofrequency therapy, and other local therapies at the appropriate time. The best supportive therapy such as analgesia, stenting, and nutritional support should also be given aggressively.
(ii) Endoscopic treatment of early gastric cancer.
Treatment of early gastric cancer includes endoscopic resection and surgical procedures. Compared with traditional surgery, endoscopic resection has less trauma, fewer complications, and recovery
fast, low cost, and comparable efficacy, with 5-year survival rates exceeding 90 . Therefore, several international guidelines and this consensus recommend endoscopic resection as the preferred treatment for early gastric cancer. The main endoscopic resections for early gastric cancer include EMR and ESD.
. Therefore, several international guidelines and this consensus recommend endoscopic resection as the preferred treatment for early gastric cancer. The main endoscopic resections for early gastric cancer include EMR and ESD.
- style=”margin-left: 110pt”>
- Definitions and terms related to endoscopic treatment
- style=”margin-left: 62pt”>
- Entire resection: The lesion is removed endoscopically in its entirety and a single specimen is obtained.
- Horizontal/vertical margin positivity: After fixation of the endoscopically resected specimen, the specimen was sectioned vertically at 2 mm intervals and was considered positive for horizontal margin if there was tumor cell infiltration at the lateral margin and positive for vertical margin if there was tumor cell infiltration at the basal margin. If there is tumor cell infiltration in the basal margin, it is called positive vertical margin.
-
Complete resection: A whole resected specimen with negative horizontal and vertical margins is called a complete resection.
- style=”margin-left: 72pt”>
- Curative resection: complete resection with no risk of lymph node metastasis is achieved.
- Curative resection: complete resection with no risk of lymph node metastasis is achieved.
-
Non-curative resection: one of the following conditions is present: ①Non-complete resection, including non-complete resection and/or positive margins; ② the presence of risk factors associated with the risk of lymph node metastasis, such as submucosal invasion deeper than 500 μm, vascular infiltration, poorly differentiated tumor, etc.
-
Local recurrence: Tumor lesions found in and around the original resection site within 1 cm more than 6 months after surgery.
-
Residual: Tumor lesions found within 1 cm of the original resection site and surrounding area within 6 months after surgery.
- style=”margin-left: 72pt”>
-
Concomitant recurrence: refers to gastric cancer endoscopic within 12 months after treatment, new
Recurrence: secondary lesions that existed at the time of endoscopic treatment but were missed and were detected by endoscopy within 12 months after surgery.
-
- style=”margin-left: 62pt”>
- Heterochronic recurrence: defined as New lesions were found more than 12 months after treatment. Most of the lesions appeared adjacent to the primary lesion in the stomach and had the same type of pathological tissue.
- Preoperative evaluation for endoscopic treatment: The decision to perform ESD or EMR needs to be based on the following.
-
Histologic type: Histopathologic type is usually determined by histopathologic examination of the biopsy specimen, although it has been reported that Histopathological type can be predicted to some extent by endoscopy, although sufficient evidence is lacking.
-
Size: Measurement of lesion size by conventional endoscopic methods is prone to error, making it difficult to accurately determine preoperative lesion size. Therefore, post-excisional tissue measurements and pathological examination are generally used as the final results.
- Whether an ulcer is present, note whether the lesion is ulcerated and, if so, whether it is an active ulcer or an ulcerated scar. Ulcer histopathology Defined as a mucosal defect of at least UL-II depth (deeper than the mucosal muscle layer). On preoperative gastroscopy, active ulcers generally appear as white exudate covering the surface of the lesion, excluding superficial erosions. In addition, when the ulcer is in the healing or scarring phase, the mucosal folds or folds converge toward a center.
-
The depth of infiltration is now routinely determined by endoscopy in early gastric cancer, and magnification endoscopy is recommended to assist in this determination. . When the aforementioned methods are difficult to determine the depth of infiltration, EUS can be used as an adjunctive diagnostic measure with significant effect.
- style=”margin-left: 48pt”>
- Endoscopic treatment techniques
- Endoscopic treatment techniques
- EMR: EMR refers to the endoscopic excision of mucosal lesions in whole or in separate blocks for the diagnosis and treatment of superficial tumors of the gastrointestinal tract. There is a lack of sufficient
Prospective studies of EMR for the treatment of early gastric cancer are not recommended.
- style=”margin-left: 62pt”>
- ESD: ESD is currently recommended as the standard procedure for the endoscopic treatment of early gastric cancer.
-
Definition: ESD is a new technique developed on the basis of EMR, in which special electrodissection knives, such as IT knife, Dual knife, Hook knife, etc., are selected for different sites, sizes and depths of infiltration of lesions. The endoscopic approach gradually separates the tissue between the mucosal layer and the intrinsic muscular layer, and finally peels off the diseased mucosa and submucosal layer completely.
- style=”margin-left: 56pt”>
- Steps: The procedure is divided into 5 steps: ①Marking around the lesion.
②Submucosal injection to significantly lift the lesion; ③Circumferential dissection of the mucosa; ④Submucosal dissection to completely separate the mucosa from the lamina propria and complete excision of the lesion in one pass.
5 Trauma management: including trauma vascularization and margin inspection.
- Steps: The procedure is divided into 5 steps: ①Marking around the lesion.
-
Other treatment techniques: Other endoscopic treatments include laser therapy, argon knife, and microwave therapy, which can only remove the tumor, but cannot obtain a complete pathological specimen. They can only remove the tumor, but cannot obtain the complete pathological specimen, nor can they confirm whether the tumor is completely removed. Therefore, they are mostly used for the treatment of precancerous gastric lesions, which require close follow-up after treatment and are not recommended as the first choice of treatment for early gastric cancer.
- style=”margin-left: 48pt”>
-
Indications for endoscopic treatment of early gastric cancer (Table 1)
-
Table 1 Absolute and relative indications for endoscopic treatment of early gastric cancer Absolute and relative indications for endoscopic treatment
|
Depth of infiltration > |
Divergence |
undifferentiated |
|||
|
cT1a(M |
UL(– |
≤
2cm |
>
2cm |
≤
2cm |
>
2cm |
|
) |
* |
||||
|
)
UL(+ |
≤
3cm |
>
3cm |
|||
|
< span style="font-family:imitation-song; font-size:14pt">)
* |
|||||
|
cT1b(SM) |
|||||

 absolute indications
absolute indications
* Only for ESD
Relative indications
Absolute indications for endoscopic treatment of early gastric cancer: Intramucosal visible to the naked eye
(cT1a) differentiated carcinoma, there must be no ulceration (scarring) occurring, i.e., UL (–). Endoscopic treatment may also be considered when one of the above criteria is exceeded for depth of invasion, lesion diameter, degree of differentiation, and combined ulceration UL(+), with minimal risk of lymph node metastasis. Patients with recurrent localized mucosal lesions after EMR/ESD treatment may be managed with expanded indications.
- style=”margin-left: 110pt”>
- Contraindications for endoscopic treatment of early gastric cancer
The more recognized contraindications to endoscopic resection in China are: (1) early gastric cancer with clear lymph node metastasis; (2) cancer invading the lamina propria; (3) patient
coagulation disorders. In addition, the relative surgical contraindication to ESD includes a negative lift sign, which is the inability to form a local augmentation of the submucosal layer at the base of the lesion after saline injection, suggesting adhesions between the submucosal and muscular layers at the base of the lesion; ESD treatment at this time is associated with a higher risk of perforation, but with skill in ESD, ESD can be safely performed even if the lift sign is negative.
- style=”margin-left: 110pt”>
- Perioperative management
- style=”margin-left: 62pt”>
-
Preoperative preparation: Preoperative Assess the patient’s general condition and exclude contraindications to anesthesia and endoscopic treatment. After obtaining informed consent from the patient and family, sign the preoperative informed consent form.
- style=”margin-left: 72pt”>
-
Postoperative management: Day 1 postoperative Fasting; close observation of vital signs.
No abnormalities on the 2nd postoperative day with liquid or soft food. It is controversial whether to repeat the endoscopy at 1 week postoperatively.
-
-
Postoperative medication: ulcer treatment: proton pump inhibitor for ulcers after endoscopic resection of early gastric cancer. The treatment of ulcers after endoscopic resection of early gastric cancer can be done with proton pump inhibitor (PPI) or H2receptor antagonist (H2receptor antagonist, H2RA) for treatment. Antimicrobial drug use: Prophylactic use of antimicrobial drugs may be considered for preoperative evaluation of large resections, long operation times and potential for perforation of the GI tract.
- style=”margin-left: 48pt”>
- Postoperative complications and management
Common post-ESD complications include bleeding, perforation, stenosis, abdominal pain, and infection.
- Postoperative complications and management
-
Hemorrhage: Intraoperative hemorrhage is recommended to be stopped by direct electrocoagulation, and delayed hemorrhage can be stopped by hemostatic clips or electric hemostatic forceps.
- style=”margin-left: 72pt”>
- Perforation: intraoperative perforation can be closed by metal clamping of the fissure in most cases.
- Perforation: intraoperative perforation can be closed by metal clamping of the fissure in most cases.
Repair is possible in most cases through metal clamping of the fissure. When the perforation is large, it is often difficult to perform endoscopic treatment and requires emergency surgery.
- style=”margin-left: 62pt”>
-
Stenosis: Stenosis or distortion of the gastric lumen occurs less frequently and is mainly seen in the post-operative ESD with a large area of the cardia, pylorus, or gastric sinus region. Endoscopic columnar balloon dilation is an effective treatment modality.
- style=”margin-left: 48pt”>
- Prognostic evaluation and follow-up
In the evaluation of curative endoscopic resection, there is confusion between the current endoscopic curative resection and R0 resection, which implies a negative margin, but a negative endoscopic margin does not imply curative resection. To standardize the prognostic evaluation criteria, this guideline recommends the eCura evaluation system (Table 2). See Table 3 for follow-up methods.
- Prognostic evaluation and follow-up
Table 2 eCura evaluation system
|
Staging |
Ulcers/depth |
Divergent |
Undifferentiated |
||
pT1a(M) |
UL(–) |
≤2cm |
≤2cm |
>2cm |
|
UL(+) |
≤3cm |
>3cm |
|||
|
pT1b(SM) |
SM1 |
≤3cm |
>3cm |
||
|
SM2 |
|||||


 eCura A* eCura B* eCura C-2
eCura A* eCura B* eCura C-2
* need to meet the en bloc whole block removal, HM0, VM0, ly (–), v (< span style="font-family:Times New Roman">–)
Table 3 different eCura Evaluation results of follow-up methods
|
eCura A |
Every 6 to 12 monthly endoscopic follow-up |
|
eCura B |
Every 6 to 12 monthly endoscopic follow-up+. family:仿宋”>abdominal ultrasound or CT follow-up |
eCura C1 |
Supplementary treatment (surgical or non-surgical) or close follow-up is recommended |
eCura C2 |
Surgical treatment or fully informed follow-up is recommended |
>
eCura C1: In differentiated carcinoma, cases that meet the other criteria for eCura A or B, but do not achieve en bloc resection or complete local excision of HM0, i.e. eCura C1. Local treatment can be used, such as re-ESD, endoscopic ablation, etc., and again an aggressive follow-up approach can be taken, taking into account the thermal effects of ESD.
eCura C2: Pathology suggests a high risk of lymph node metastasis. Although there is a high risk of lymph node metastasis, treatment with ESD may be indicated on a case-by-case basis after adequate information about the risk of lymph node metastasis.
It is of interest that the choice of additional surgery and the control of the timing of surgery in patients with eCura C is controversial, focusing on the following 3 areas.
(1)80  More than 80 eCura C patients did not develop local recurrence or lymph node metastasis.
More than 80 eCura C patients did not develop local recurrence or lymph node metastasis.
- style=”margin-left: 62pt”>
-
For vascular infiltration, nerve invasion, lymph node invasion, and horizontal The role and impact of risk factors such as vascular infiltration, nerve invasion, lymph node invasion, and horizontal / vertical margins for evaluation in lesion recurrence need to be further refined.
-
The prognosis of eCura C patients who underwent additional surgery immediately after ESD versus those who underwent local recurrence after ESD. There was no significant difference in prognosis between patients who underwent additional surgery immediately after ESD and those who underwent local recurrence after ESD and then surgery.
In summary, the need for immediate additional surgery in eCura C patients needs to be supported by more detailed clinical data. The need for immediate additional surgery in eCura C patients needs to be supported by data from more detailed clinical studies.
(iii) Surgical treatment.
- style=”margin-left: 110pt”>
- Principles of surgical treatment
Surgical resection is the main treatment for gastric cancer and is currently the only way to cure it. Gastric cancer surgery is divided into radical surgery and non-radical surgery. Radical surgery involves complete removal of the primary lesion and complete clearance of the regional lymph nodes and includes standard, modified, and expanded surgery; non-radical surgery includes palliative and tumor-reducing surgery.
- style=”margin-left: 62pt”>
-
Radical surgery: 1) Standard surgery is aimed at radical treatment. It requires that more than 2/3 of the stomach must be removed and D2 lymph node dissection is performed. (2) Modified surgery is mainly for early-stage tumors, requiring partial or total gastric resection and D1 or D1+ lymph node dissection. (iii) Extended surgery includes combined organ resection or (and) extended surgery with D2+ lymph node dissection.
-
Non-radical surgery: 1) Palliative surgery is mainly performed for patients with tumor complications (bleeding, obstruction, etc.). The main surgical procedures include palliative gastric resection, short-circuit gastrojejunostomy and jejunal nutrition tube placement. Gastric resection is not recommended for patients with unresectable liver metastases or peritoneal metastases without tumor complications.
- style=”margin-left: 48pt”>
- Treatment flow
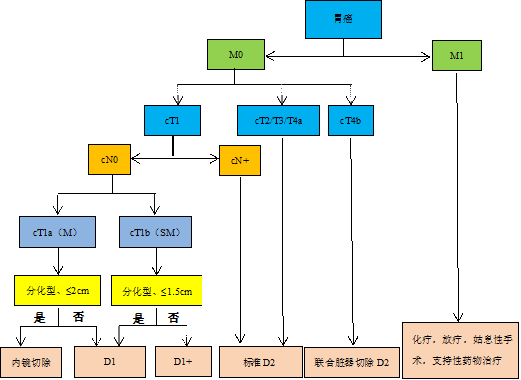
The surgical-based treatment flow according to cTNM staging is shown in Figure 4, and the postoperative treatment flow is shown in Figure 5.
- Treatment flow
 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0941_202237.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0941_202237.png" alt=""/>
Figure 4 Treatment flow
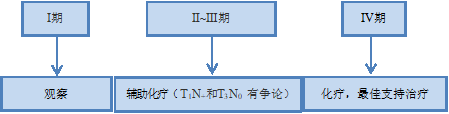
Figure 5 Postoperative treatment (according to postoperative pTNM staging)
- style=”margin-left: 110pt”>
- Requirements for safe margin cutting
- style=”margin-left: 62pt”>
- For T1 tumors, a 2 cm margin should be sought, and endoscopic localization should be performed when the tumor border is unclear.
- For tumors above T2, a minimum of 3 cm proximal margin is recommended for Borrmann types I and II, and a minimum of 5 cm proximal margin is recommended for Borrmann types III and IV.
Margins.
- style=”margin-left: 134pt”>
- When the above principles cannot be achieved, it is recommended to check the proximal edge by frozen section
The margin.
- style=”margin-left: 134pt”>
- For tumors with esophageal invasion, a margin cut of 3-5 cm or a frozen section is recommended.
Slice examination for R0 resection.4. Selection of the extent of gastrectomy
The extent of gastrectomy is different for different sites of gastric cancer. In the lower part of the stomach, a distal gastrectomy or total gastrectomy is performed, in the body of the stomach, a total gastrectomy is performed, and in the gastroesophageal junction, a proximal gastrectomy or total gastrectomy is performed.
According to clinical staging.
- style=”margin-left: 62pt”>
-
Gastric cancer with cT2-4 or cN(+) is usually chosen Standard partial gastrectomy or total gastrectomy.
-
cT1N0M0 gastric cancer, depending on the location of the tumor, in addition to the above surgical options proximal gastrectomy, pylorus-preserving gastrectomy, and partial gastrectomy can be chosen.
-
For combined organ resection, radical combined organ resection is feasible if the tumor directly invades the surrounding organs. If the tumor directly invades the surrounding organs, radical combined organ resection is feasible. In cases where the tumor is located in the greater curvature of the stomach with No.4sb lymph node metastasis, total gastrectomy in combination with splenectomy is considered. In other cases, prophylactic splenectomy is not recommended except for direct tumor invasion.
- style=”margin-left: 48pt”>
- Lymph node dissection
According to current evidence-based medical evidence and domestic and international guidelines, lymph node dissection ranges from
- Lymph node dissection
The circumference is determined based on the extent of gastrectomy (Table 3).
D1 resection includes removal of the greater and lesser omentum and its inclusion in the right and left cardia, the greater and lesser curvatures of the stomach, and the suprapyloric and subpyloric lymph nodes adjacent to the right gastric artery, as well as the lymph nodes adjacent to the left gastric artery. For cT1aN0 and cT1bN0, differentiated gastric cancers with a diameter of <1.5 cm, D1 is performed; for cT1N0 gastric cancers other than those mentioned above, D1+ is performed. D2 resection is based on D1, followed by clearance of the abdominal trunk, common hepatic artery, and
Lymph nodes of the splenic artery and hepatoduodenal ligament (see Appendix for grouping of perigastric lymph nodes). A minimum of 16 or more lymph nodes should be cleared to ensure accurate staging and prognosis. D2 clearance should be performed for cT2-4 or cN(+) tumors. When the extent of lymph node dissection does not fully meet the appropriate D criteria, the lymph nodes can be dissected as
Actually recorded as D1 (+ No. 8a), D2 (-No 10), etc.
Table 3 Lymph node dissection extent
|
D0 |
D1 |
D1 + |
D2 |
||
Total Gastrectomy |
<D1 |
No.1~7 |
D1 + No.8a,9,11p *No.110 |
D1 + No.8a,9,11p,11d,,12a *No.19,20,110,,111 |
|
Distal gastrectomy |
<D1 |
No.1,3,4sb,4d,5,6,7 |
D1 + No.8a,9 |
D1 + No.8a,9,11p,12a |
|
|
Proximal gastrectomy |
<D1 |
No.1,2,3a,4sa,4sb,7 |
D1 + No.8a,9,11p *No.110 |
||
Pyloric Gastrectomy Preserved |
No.1,3,,4sb, |
D1+: |
|
Excluding surgery |
4d,6,7 |
D1+No.8a,9 |
Note: *Tumor invaded esophagus
Expanded lymph node dissection: Expanded lymph node dissection beyond D2 should be considered for the following cases. ①Progressive upper gastric cancer infiltrating the greater curvature of the stomach is recommended for D2+No.10 debulking. (2) D2+No.14v lymph node dissection is recommended for the presence of lymph node metastasis of group No.6 in the lower gastric cancer. (3) D2+No.13 lymph node dissection is recommended in the presence of duodenal infiltration in subgastric cancer.
The need for and how to perform lymph node dissection of the splenic hilum is more controversial. The rate of metastasis to the splenic hilar lymph nodes varies widely between the literature, and patients with stage T1 and T2 gastric cancer do not require splenic hilar lymph node dissection. Therefore, splenorenal lymph node dissection is recommended in the following cases: primary tumor >6 cm, located in the greater curvature, and preoperative stage T3 or T4 upper middle gastric cancer.
- style=”margin-left: 115pt”>
- Carcinoma of the combined gastroesophagus
There is no consensus on the extent of gastrectomy and lymph node dissection for combined gastroesophageal cancer. Based on the current evidence-based medical evidence, the following recommendations are available
- style=”margin-left: 62pt”>
-
Tumor centered within 2 cm above and below the gastroesophageal junction and <4 cm in length. The tumor center is located within 2 cm above and below the gastroesophageal junction, and the length diameter is <4 cm. proximal gastrectomy (+ lower esophageal resection) or total gastrectomy (+ lower esophageal resection) can be chosen for esophagogastric junction cancer. cT1 tumor recommended lymph node dissection range No.1, 2, 3, 7, 9, 19, 20. cT2-4 tumor recommended lymph node dissection range No.1, 2, 3, 7, 8a, 9, 11p, 11d, 19, 20. Additional sweeping of the lower mediastinal lymph nodes if the center is located above the esophagogastric junction.
- style=”margin-left: 61pt”>
-
When the tumor invades the esophagus <3 cm The transabdominal transdiaphragmatic surgery is recommended; invasion
-
If the length of the esophagus is >3 cm and the procedure is potentially curative, open thoracotomy should be considered.7 7. laparoscopic surgery
Indications: Gastric cancer invasion depth within T2, or laparoscopic exploration for staging. There are a growing number of clinical findings confirming the safety and long-term efficacy of laparoscopy performed for progressive gastric cancer, but centers should carefully select their indications based on their own team’s experience and conduct further randomized controlled studies for exploration.
- style=”margin-left: 107pt”>
- Gastrointestinal Tract Reconstruction
There are different GI reconstruction modalities for different gastrectomy modalities. Reconstruction is recommended using a variety of anastomoses to increase the safety of the anastomosis and reduce complications. Based on current evidence-based medical evidence, the following recommendations are made for different gastrectomy modalities.
- style=”margin-left: 62pt”>
-
Reconstruction modalities after total gastrectomy: Roux-en-Y anastomosis, jejunal interposition method.
-
Reconstruction after distal gastrectomy: Billroth I, Billroth II Combined Braun anastomosis, Roux-en-Y anastomosis, and interjejunal placement method.
- style=”margin-left: 61pt”>
- Reconstruction after pylorus preserving gastrectomy: Gastric anastomosis.
- Reconstruction after pylorus preserving gastrectomy: Gastric anastomosis.
-
Reconstruction after proximal gastrectomy: esophageal remnant gastric anastomosis, interjejunal placement.
- style=”margin-left: 48pt”>
- Other
- Other
- Splenectomy: primary T2-T4 tumor directly invading the spleen or located in the superior greater curvature of the stomach. Splenectomy for the purpose of lymph node dissection is not recommended.
- For T1 / T2 tumors, the greater omentum can be preserved more than 3 cm from the vascular arch of the gastric omentum.
- style=”margin-left: 62pt”>
-
Tumors with direct invasion of the primary or metastatic lesions into adjacent organs can be treated with combined resection of the involved organs.
- style=”margin-left: 56pt”>
-
- Antimicrobial drugs.
- Antimicrobial drugs.
Preventive use: the incision of gastric cancer surgery is a class II incision, and the bacteria that may be contaminated are gram-negative bacilli, streptococci, and oropharyngeal anaerobes (e.g., Streptococcus alginolyticus). Cephalosporins, or cephalosporins; for those allergic to β-lactams, clindamycin + aminoglycosides, or aminoglycosides + metronidazole. The route of administration is intravenous; the drug should be given within 0.5 to 1 hour before skin or mucous membrane incision or at the beginning of anesthesia, and the surgery should be started after the infusion is completed to ensure that the concentration of antimicrobial drugs in the local tissues at the time of surgical site exposure is sufficient to kill bacteria contaminated during the surgery. The effective duration of antimicrobial drug coverage should include the entire surgical procedure. If the duration of surgery exceeds 3 hours or more than twice the half-life of the drug used, or if the adult bleeding volume exceeds 1500 ml, an additional dose should be administered intraoperatively. Prophylactic medication for Class II incisions should be administered for 24 hours, but may be extended to 48 hours if necessary. Excessively prolonged dosing
Does not further improve prophylaxis and increases the chance of infection with drug-resistant organisms when prophylaxis is administered beyond 48 hours.
Therapeutic use: Develop an antibacterial regimen based on the pathogen, site of infection, severity of infection, and the patient’s physiology and pathology, as well as pharmacodynamic and pharmacokinetic evidence of antibacterial drugs, including the choice of antibacterial drug species, dose, frequency of administration, route of administration, duration of therapy, and combination of drugs. The general course of treatment should be used until 72-96 hours after the body temperature is normal and the symptoms have subsided.
-
- style=”margin-left: 62pt”>
-
Nutrition Supportive therapy: Patient-generated subjective global assessment (PG-SGA) combined with nutritional risk screening (NRS) 2002 is recommended for nutritional risk screening and assessment.
Patients with an NRS2002 score of ≥3 or a PG-SGA score of 2 to 8 should be given preoperative nutritional support; patients with an NRS2002 score of ≥3 and a PG-SGA score of ≥9 who undergo elective surgery may still benefit from surgery after 10 to 14 days of nutritional support. Immunonutrition is recommended for 5 to 7 days before surgery in patients undergoing major open surgery, regardless of their nutritional status, and continues until 7 days after surgery or until the patient consumes >60
 needed. Immune-enhanced enteral nutrition should contain all three substrates: omega-3 polyunsaturated fatty acids, arginine, and nucleotides. Adding these 3 nutrients alone
needed. Immune-enhanced enteral nutrition should contain all three substrates: omega-3 polyunsaturated fatty acids, arginine, and nucleotides. Adding these 3 nutrients aloneeither 1 or 2 of these nutrients alone need to be studied further. Oral enteral nutrition support is preferred.
Patients with moderate malnutrition planning major surgery or those with severe malnutrition are recommended to receive nutrition therapy for 1 to 2 weeks before surgery, even if surgery is delayed. It is expected that nutrition will not be met by normal diet more than 7 days after surgery.
patients whose nutritional needs cannot be met by a normal diet more than 7 days after surgery, and patients whose nutritional needs cannot be met by oral feeding for 60
 Patients with more than 1 week of need should be given postoperative nutritional therapy.
Patients with more than 1 week of need should be given postoperative nutritional therapy.Enteral nutrition is recommended for postoperative patients; patients are encouraged to resume oral feeding as soon as possible, and oral nutritional support is recommended for those who can eat by mouth; for those who cannot have early oral nutritional support, tube feeding is used, and enteral nutrition using a nasojejunal tube is recommended for patients with gastric cancer.
Timing of supplemental parenteral nutrition: NRS2002 score ≤3 or NUTRIC rating
Patients at low nutritional risk with an NRS2002 score ≤ 5 should initiate parenteral nutrition support only if enteral nutrition fails to meet 60% of target energy and protein requirements for more than 7 days. For patients at high nutritional risk with NRS2002 ≥ 5 or NUTRIC score ≥ 6, early implementation of parenteral nutrition is recommended if enteral nutrition fails to achieve 60% of the target energy and protein requirements within 48-72 hours. Discontinue parenteral nutrition when the enteral nutrition supply reaches the target requirement of 60 .
.
- style=”margin-left: 134pt”>
- Pain management: opioids are not recommended to be given to patients preoperatively
or non-selective NSAIDs because of the lack of benefit.
Postoperative pain is a response of the body to surgical stimulation (tissue damage). Effective postoperative pain management can reduce patient suffering and also facilitate recovery. Multimodal analgesic regimens are recommended, and NSAIDs are recommended as the basis for postoperative analgesia in several guidelines in the United States and Europe. Multimodal analgesia also includes oral acetaminophen, local infiltration of ropivacaine in the incision or combined with epidural analgesia in the mid-thoracic segment. Opioid analgesia should be avoided or minimized because of the large adverse effects of opioids, including impairment of gastrointestinal recovery, respiratory depression, dizziness, nausea, and vomiting.
- style=”margin-left: 62pt”>
-
Management of postoperative nausea and vomiting: All inpatients with postoperative nausea and vomiting (PONV) in all hospitalized patients 20
 to 30
to 30, mainly within 24 to 48 hours postoperatively, but rarely for up to 3 to 5 days. Associated risk factors: female, postoperative use of opioid analgesics, nonsmoking, history of PONV, or history of motion sickness.
PONV prophylaxis: Determine the patient’s risk for PONV; patients without risk factors for PONV do not require prophylaxis. For low- and intermediate-risk patients, Table 4 in 1
or 2 types of prophylaxis. For high-risk patients, 2 to 3 drugs are available for prophylaxis.
A combination of drugs with different mechanisms of action is better than a single drug. 5-hydroxytryptamine 3 receptor inhibitors, dexamethasone and haloperidol or haloperidol are the most effective drugs for PONV prevention with few side effects. The gold standard for clinical control of PONV is 24-hour effectiveness and complete absence of nausea and vomiting.
 Table 4 Commonly Used PONV Prevention PONV Dose and duration of drug use
Table 4 Commonly Used PONV Prevention PONV Dose and duration of drug use
Drug Dosing Schedule Adult Dose Pediatric Dose

Ondansetron before the end of surgery 4mg IV 0.05 0.1mg/kg IV (maximum dose 4mg)
8mg ODT
Dolasetron before the end of surgery 12.5mg IV 0.35mg/kg IV(maximum dose 12.5mg) Granisetron before the end of surgery 0.35 to 3mg IV 0.04mg/kg IV (maximum dose 6mg) Toltestrone before the end of surgery 2mg IV 0.1mg/kg IV (maximum dose 2mg)
Palonosetron before induction 0.075mg IV
Arepitant before induction 40mg PO
Dexamethasone after surgery 4 to 5mg IV 0.15mg/kg IV (maximum dose 5mg)
Flupredol before the end of surgery 0.625 to 0.625 =”font-family:Times New Roman”>1.25mg IV 0.01 to 0.015mg/kg IV (maximum dose 1.25mg)
Haloperidol
Before the end of surgery or after induction
0.5 to 2mg IM or IV
Benadryl at induction 1mg/ kg IV 0.5mg/kg IV (maximum dose 25mg)
East Used Danganine
The night before surgery or
Paste
Before surgery 2 to 4 hours
 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0941_202247.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0941_202247.png" alt=""/>
Note: IV, intravenous; ODT, orally disintegrating tablets; PO, oral; IM, intramuscular injection.
Treatment of PONV: For patients leaving recovery from anesthesia with persistent nausea and vomiting, antiemetic management should be performed first after bedside examination to exclude drug stimulation or mechanical factors.
If the patient has no prophylactic medication, the first presentation of PONV should be initiated with a small dose of 5-hydroxytryptamine 3 receptor inhibitor therapy, usually 1/4 of the prophylactic dose. dexamethasone 2 to 4 mg, haloperidol 0.625 mg or If the patient develops PONV in the recovery room after anesthesia, consider sedation of propofol 20 mg.
If prophylaxis has been administered, the treatment should be switched to another type of medication. If PONV occurs in a patient despite triple therapy prophylaxis, it should not be repeated within 6 hours and should be switched to another drug; if it occurs at 6 hours, consider giving a repeat 5-
hydroxytryptamine 3 receptor inhibitor and haloperidol or haloperidol at the same dose as before. Repeated applications of dexamethasone are not recommended.
- style=”margin-left: 62pt”>
-
Perioperative fluid management: Perioperative fluid balance can improve the prognosis of patients undergoing gastrectomy, both in terms of avoiding tissue perfusion deficit and organ function impairment due to hypovolemia and in terms of tissue edema and increased cardiac load due to volume overload. An intraoperative goal-directed-based treatment strategy can maintain appropriate circulatory volume and tissue oxygen supply in patients.
-
Prevention of stress ulcers: Stress ulcers are caused by the body in various types of stressful conditions such as severe trauma, critical illness or severe psychological illness. The most important thing is that the body has to be able to take care of its own health.
and even perforation, which can aggravate and worsen the degree of pre-existing disease and increase morbidity and mortality. In critically ill patients, PPI is superior to H2RA, and the recommended standard dose of PPI is administered intravenously once every 12 hours for at least 3 days, and can be switched to oral administration or gradually discontinued when the patient is stable enough to tolerate enteral nutrition or has eaten, or when clinical symptoms begin to improve or is transferred to a general ward. In non-critical patients, PPI and H2RA are comparable in efficacy. Because of the low incidence of severe clinical bleeding, studies have shown that the use of drugs for bleeding prevention in this group of patients is not effective, and therefore no consensus recommendation can be made for the prevention of postoperative stress ulcers in non-critical patients.
- style=”margin-left: 62pt”>
-
Perioperative Airway Management: Perioperative airway management can effectively reduce complications, shorten hospital stay, reduce readmission rates and risk of death, improve patient prognosis, and reduce healthcare costs. Commonly used therapeutic agents for perioperative airway management include antimicrobials, glucocorticoids, bronchodilators (β2 receptor agonists and anticholinergics), and mucolytics. For patients with postoperative respiratory tract infections, antibacterial drugs can be used to treat them according to the Guidelines for Clinical Use of Antibacterial Drugs (2015 edition); glucocorticoids and bronchodilators are mostly used in combination, via nebulized inhalation, 2 to 3 times a day for 7 to 14 days; mucolytic agents commonly used in the perioperative period are amiloride hydrochloride, which can reduce the decline of pulmonary surface active substances caused by mechanical injury during surgery, and reduce pulmonary complications such as atelectasis. It can reduce the decrease of pulmonary surface active substance caused by mechanical injury during surgery and reduce the occurrence of pulmonary complications such as atelectasis. For patients with poor respiratory function or chronic underlying lung diseases such as chronic obstructive pulmonary disease, preoperative prophylaxis is recommended until the postoperative period. It should be noted that amiloride hydrochloride is an intravenous formulation and is not recommended for nebulized inhalation use.
-
Other: Other relevant medication management and adjustments in the perioperative period for patients with underlying disease For more information, see the UpToDate Perioperative Medication Management topic.
For patients with more complex conditions, it is recommended to consult with the relevant specialty.
(iv) Chemotherapy.
Categorized into palliative chemotherapy, adjuvant chemotherapy, and neoadjuvant chemotherapy and translational therapy, it should be administered under the guidance of a medical oncologist with strict clinical indications and exclusion of contraindications. Chemotherapy should be administered with full consideration of the patient’s disease stage, age, physical condition, treatment risk, quality of life and patient’s will to avoid over-treatment or under-treatment. Timely assessment of chemotherapy efficacy, close monitoring and prevention of adverse reactions, and adjustment of drugs and/or doses as appropriate. Evaluate the efficacy of chemotherapy according to the RECIST efficacy evaluation criteria (see Appendix). Adverse effects were evaluated according to the NCI-CTC criteria.
- style=”margin-left: 110pt”>
- Palliative chemotherapy
The aim is to relieve clinical symptoms caused by tumor, improve quality of life and prolong survival. It is indicated for unresectable, postoperative recurrent metastases or after palliative resection in patients with good general condition and essentially normal major organ function. Contraindicated in patients with severe organ dysfunction, uncontrollable co-morbidities and expected survival of less than 3 months. Commonly used systemic chemotherapeutic agents include: 5-fluorouracil, capecitabine, tegeo, cisplatin, oxaliplatin, paclitaxel, docetaxel, albumin paclitaxel, irinotecan, epothilone, etc. Targeted therapeutic agents include: trastuzumab, apatinib. Chemotherapy regimens include 2-drug combination or 3-drug combination regimens.
2-drug regimens include: 5-fluorouracil/calcium folinate + cisplatin (5-FU/LV+FP), capecitabine + cisplatin (XP), tegeo + cisplatin (SP), 5-fluorouracil + oxaliplatin (FOLFOX), capecitabine + oxaliplatin (XELOX), tegeo + oxaliplatin (SOX), capecitabine + paclitaxel, capecitabine + docetaxel, 5-fluorouracil/calcium folinic acid + irinotecan (FOLFIRI), etc.3 Drug formulary
Cases are indicated for patients with advanced gastric cancer in good physical condition, and commonly used include: epothilone + cisplatin + 5-fluorouracil (ECF) and its derivatives (EOX, ECX, EOF), docetaxel + cisplatin + 5-fluorouracil (DCF) and its modifications (FLOT , DOX, DOS), etc. Albumin-bound paclitaxel as second-line treatment is comparable to regular paclitaxel in efficacy, and allergic reactions rarely occur, and is now also an optional chemotherapeutic agent. For patients with poor physical status and advanced age, single-agent chemotherapy with oral fluorouracil-based drugs or paclitaxel-based drugs is considered. For patients with advanced gastric cancer with positive HER2 expression (++++ immunohistochemical staining or +++ immunohistochemical staining and positive FISH test), the combination of molecularly targeted therapy trastuzumab in addition to chemotherapy may be considered. Patients with advanced gastric cancer who have failed 2 previous chemotherapy regimens and are in good health may be considered for single-agent apatinib therapy.
Cautions for palliative chemotherapy are as follows.
- style=”margin-left: 62pt”>
- Gastric cancer is a highly heterogeneous malignancy that is difficult to treat, and patients are actively encouraged to participate in clinical studies as much as possible.
-
For patients with recurrent metastatic gastric cancer, the 3-drug regimen is appropriate for those with a high tumor load and good physical status. In contrast, single-agent chemotherapy is indicated for patients with advanced age, poor physical status, or mild organ dysfunction.
-
For patients whose disease has been controlled with systemic chemotherapy, regular review is still needed, and according to retrospective and observational studies In patients with disease control after systemic chemotherapy, periodic review is still required, and sequential single-agent maintenance therapy after standard chemotherapy may improve quality of life and reduce adverse effects compared with standard chemotherapy, generally after 4 to 6 cycles of standard chemotherapy, according to retrospective and observational studies.
- Peritoneal metastasis is a specific metastatic pattern in patients with advanced gastric cancer, often accompanied by cancerous ascites and cancerous intestinal obstruction, which affects patients’ eating and quality of life. Treatment
Absorptive drainage and peritoneal perfusion chemotherapy are needed to improve general condition according to abdominal distension, etc., combined with systemic chemotherapy at an elective stage.
- style=”margin-left: 110pt”>
- Adjuvant chemotherapy
Adjuvant chemotherapy is indicated for those with stage II and stage III pathology after D2 radical surgery. Adjuvant chemotherapy is not recommended for stage Ia, and there is no sufficient evidence-based medical evidence on whether postoperative adjuvant chemotherapy is needed for stage Ib gastric cancer, but adjuvant chemotherapy can be considered for patients with positive lymph nodes (pTIN1M0), and adjuvant chemotherapy for patients with pT2N0M0 who are young (<40 years old), histologically hypodifferentiated, with neural tract or vascular or lymphatic infiltrative factors, mostly as single agents, with potential to reduce recurrence. Combination chemotherapy should be completed within 6 months, and single-agent chemotherapy should not exceed 1 year. Adjuvant chemotherapy
The recommended regimen is a 2-drug combination of fluorouracil and platinum. For the body
People with poor physical status, advanced age, and intolerance to 2-drug combination regimens should be considered for single-agent chemotherapy with oral fluorouracil.
Cautions for adjuvant chemotherapy are as follows.
- style=”margin-left: 62pt”>
- Adjuvant chemotherapy begins when the patient’s postoperative physical status has largely returned to normal, usually 4 weeks after surgery. Special attention is given to the need for patients to resume postoperative feeding and for perioperative complications to resolve.
-
Other 2-drug combinations of fluorouracil and platinum may also be considered in adjuvant chemotherapy. Recent studies suggest an improved prognosis with docetaxel in combination with tegeo capsules compared with tegeo capsules alone after stage III gastric cancer, and docetaxel in combination with tegeo could potentially be another option for adjuvant chemotherapy.
- Observational studies suggest that stage II patients have similar survival benefit with single-agent versus combination chemotherapy, but stage III patients benefit more significantly from the combination. Also needed
The choice of single-agent oral or combination chemotherapy needs to be considered in the context of the patient’s physical condition, age, underlying disease, and type of pathology.
- style=”margin-left: 62pt”>
-
Dose adjustment during adjuvant chemotherapy should be standardized and reasonable. The patient’s nutritional and physical status should be closely monitored to ensure weight maintenance and to maintain the body’s immune function. If the combination chemotherapy is not tolerated, the dose can be reduced or adjusted to a single agent, and the treatment cycle can be maintained while maintaining the overall condition.
- style=”margin-left: 48pt”>
- Neoadjuvant chemotherapy
For locally progressive gastric cancer without distant metastases (T3/4, N+), neoadjuvant chemotherapy is recommended and should be a 2-drug regimen of platinum in combination with fluorouracil, or
A 3-drug combination chemotherapy regimen with paclitaxel on top of a 2-drug regimen, not
single-agent regimens are appropriate. The time frame for neoadjuvant chemotherapy generally does not exceed 3 months, and the efficacy should be evaluated in a timely manner, and attention should be paid to determining adverse effects and avoiding additional surgical complications. Postoperative adjuvant therapy should be based on preoperative staging and neoadjuvant chemotherapy efficacy, with effective continuation of the original regimen or adjustment of the treatment regimen as appropriate based on patient tolerance, and ineffective replacement of the regimen or addition of targeted agents such as apatinib.
Neoadjuvant chemotherapy considerations are as follows.
(1) Whether the 3-drug regimen is appropriate for the entire neoadjuvant chemotherapy population, particularly in the Eastern population, is controversial. Small sample prospective randomized controlled studies have not shown 3
The efficacy of the 3-drug regimen is superior to the 2-drug regimen, and the survival benefit is more pronounced. We conducted
Multiple prospective clinical studies of 2-drug regimens have been conducted, initially showing good efficacy and perioperative safety. It is recommended to fully communicate with patients and families on the basis of multidisciplinary collaboration based on clinical practice.
- style=”margin-left: 72pt”>
- For patients who achieve pathologic complete remission, consideration for treatment with
- Neoadjuvant chemotherapy
Effective patients, combined with preoperative staging, are recommended in principle to continue the preoperative chemotherapy regimen.
- style=”margin-left: 62pt”>
-
Patients with suboptimal neoadjuvant chemotherapy should be evaluated by the MDT team
- style=”margin-left: 48pt”>
- Translational therapy
For patients with locally progressive gastric cancer that is initially unresectable but not associated with distant metastases, chemotherapy or concurrent radiotherapy can be considered for conversion to resectable tumor after shrinkage. For chemotherapy alone, refer to the neoadjuvant chemotherapy protocol; for concurrent radiotherapy, refer to the radiotherapy section.
Cautions are as follows.
- Translational therapy
-
Unresectable oncologic causes are the population addressed in this section, including severe invasion of the primary tumor, or fixed, fused regional lymph node metastases The primary tumor is severely invasive, or the regional lymph node metastases are fixed, fused, and massed, cannot be separated from the surrounding normal tissue or have encircled large blood vessels; those who cannot be resected due to the patient’s physical condition and other underlying diseases, and for which translational therapy is not applicable, refer to palliative chemotherapy and radiotherapy.
-
The resectability of the tumor should be evaluated mainly by surgical oncology with the help of imaging, endoscopy and other means. PET-CT and/or laparoscopic exploration, if necessary, for precise clinical staging and overall treatment strategy.
-
Unlike neoadjuvant chemotherapy, evidence-based evidence for translational therapy comes more from experience in the treatment of advanced gastric cancer. The evidence for translational therapy is derived more from the experience of treatment of advanced gastric cancer, where R0 resection is possible only after tumor regression, so there is a greater emphasis on efficient tumor reduction, and 3-drug chemotherapy regimens can be considered relatively aggressively if tolerated by the patient.
- style=”margin-left: 72pt”>
- Preliminary studies suggest that concurrent radiotherapy is more effective than radiotherapy alone or chemotherapy alone.
- Preliminary studies suggest that concurrent radiotherapy is more effective than radiotherapy alone or chemotherapy alone.
may achieve greater tumor regression, but the current indications and timing of its introduction need to be further explored and are recommended to be carried out in clinical studies; in clinical practice In clinical practice, a multidisciplinary team is recommended to evaluate and determine the best treatment modality.
- style=”margin-left: 62pt”>
- Gastric cancer with only a single distant metastasis at initial diagnosis without other non-curative factors and technically resectable is a special group, such as those with only liver metastases, ovarian metastases, 16 metastases, ovarian metastases, group 16 lymph node metastases, positive peritoneal exfoliation cytology, or limited peritoneal metastases. R0 resection has been shown in cohort studies to be achieved in some patients after tumor shrinkage by translational therapy, but is currently only recommended for active consideration in clinical studies. In clinical practice, the benefits and risks of surgery must be carefully judged by a comprehensive assessment by a multidisciplinary team, taking into account the patient’s age, underlying disease, physical status, compliance, social support, metastatic site, type of pathology, efficacy and adverse effects of translational therapy, and other options beyond surgery.
-
Local recurrence of gastric cancer after radical surgery should be evaluated first for the possibility of re-excision; in the case of a single distant metastasis that occurred after radical surgery. In the case of a single distant metastasis after radical surgery, in addition to the above (5), the first surgical staging, adjuvant treatment options, disease-free survival time, and risk factors for recurrence should be considered.
-
After translational therapy, a multidisciplinary team is recommended to re-evaluate the feasibility and likelihood of radical surgery, and the risks of treatment need to be fully communicated with the patient and family. The risks and benefits of treatment need to be fully communicated with the patient and family. The remaining perioperative efficacy assessment and safety management are equivalent to neoadjuvant chemotherapy.
(v) Radiotherapy.
Radiotherapy is one of the important treatments for malignant tumors. According to the clinical follow-up study
Research data and autopsy data suggest that the risk of local recurrence and distant metastasis is high after gastric cancer surgery, and radiotherapy can reduce the risk of local recurrence by irradiating the primary tumor location and lymphatic drainage area Radiotherapy can reduce the risk of local recurrence by irradiating the primary tumor location and lymphatic drainage area. Under the guidance of multidisciplinary treatment, radiotherapy can be combined with surgery, chemotherapy, molecular targeted therapy and other therapies to develop a reasonable treatment plan for the benefit of patients. Currently, the NCCN guidelines in the United States and the ESMO guidelines in Europe recommend radiotherapy before or after surgery for locally advanced gastric cancer under certain circumstances. With the development and widespread use of D2 surgery, the indications for postoperative radiotherapy and the scope of radiotherapy have become a hot topic of discussion. For preoperative radiotherapy of locally advanced gastric cancer, especially for combined gastroesophageal cancer, several studies have shown that preoperative simultaneous radiotherapy can significantly reduce tumor load and provide help to improve tumor cure rate.
- style=”margin-left: 110pt”>
-
Indications for radiotherapy
- Good general condition with KPS ≥ 70 or ECOG score 0-2.
- Good general condition with KPS ≥ 70 or ECOG score 0-2.
- style=”margin-left: 62pt”>
-
Preoperative radiotherapy: For surgically resectable or potentially resectable locally advanced gastric cancer, preoperative concurrent radiotherapy can improve long-term prognosis by achieving a higher R0 surgical resection rate and significantly reducing the tumor stage. For non-surgically resectable locally advanced gastric cancer, preoperative concurrent radiotherapy can improve the prognosis by significantly shrinking the tumor and converting part of the tumor into a resectable lesion, increasing the R0 surgical resection rate. The combination of preoperative synchronized radiotherapy and chemotherapy can be tried if the patient tolerates it well.
-
Postoperative radiotherapy: ①Postoperative radiotherapy is recommended for those with positive surgical margins; ②R0 resection and lymph node clearance
Postoperative concurrent radiotherapy is recommended for those with lymph node metastases; (3) R0 resection and D2 lymph node clearance range: postoperative concurrent radiotherapy can be considered for those with pathological lymph node metastases. The postoperative synchronous radiotherapy is recommended for those with R0 resection and D2 lymph node clearance.
- style=”margin-left: 62pt”>
- Patients with gastric cancer who refuse to undergo surgery or cannot tolerate surgery due to medical conditions.
-
Decompensated radiotherapy for advanced gastric cancer: For patients with distant metastases, irradiation of the primary or metastatic foci, depending on the situation, can achieve relief of The purpose is to relieve obstruction, compression, bleeding or pain, and to improve the patient’s survival quality. Irradiation of only the primary lesion and metastatic lesions causing symptoms, with the irradiation dose determined by the size, location and tolerance of the lesion.
- style=”margin-left: 48pt”>
- Radiotherapy techniques
Intensity modulated radiotherapy techniques, including volumetric rotational intensity modulated radiotherapy and spiral tomography intensity modulated radiotherapy, have better dose distribution conformality and uniformity than 3D conformal radiotherapy, and can be combined with simultaneous target-in-target or intra-target dose addition modes to increase the dose to normal tissue without increasing the dose to normal tissue. The dose to the gastric tumor can be increased without increasing the dose to normal tissue.
- Radiotherapy techniques
-
Radiotherapy target area: For non-surgically resected lesions, conventional split-dose radiotherapy covers the primary tumor and metastatic lymph nodes, as well as prophylactic irradiation of lymph nodes in high-risk areas. For non-surgically resected lesions, conventional split-dose radiotherapy included primary tumor and metastatic lymph nodes, as well as prophylactic irradiation of high-risk regional lymph nodes (Table 5).
Table 5 High-risk selective irradiation of lymphatic drainage areas
Primary site
Lymphatic drainage area to be irradiated
Proximal 1/3
Middle 1/3
Distal 1/3
7, 8, 9, 11p, 16a2, 16b1*
7, 8, 9, 11p, 12a, 13, 14#, 16a2,
16b1*
7, 8, 9, 11p, 12a, 13, 14#, 16a2.
16b1*
#: If zone 6 lymph node metastasis, zone 14 must be included.
*: If zone 7 to 12 lymph node metastases or N2/3 lesions, they must be included up to 16b1.
The scope of radiotherapy for postoperative treatment includes selective irradiation of the tumor bed and anastomosis, as well as prophylactic irradiation of high-risk lymph node areas. For anastomosis and tumor bed irradiation, the following indications are recommended: incision margin <3 cm from the tumor including the corresponding anastomosis and postoperative radiotherapy including the tumor bed for T4b, especially for posterior gastric wall lesions (Table 6). Table 6 Postoperative target area Selective irradiation range
Table 6 Postoperative target area Selective irradiation range
Staging Anastomosis Tumor bed and organ involvement area Lymphatic drainage area

T4bNany Yes Yes
T1~4aN+ T4aN0
Cutting edge ≤ 3cm No Yes
then must include No Yes T3N0 No Yes
T3N0 No Yes
Palliative cases may irradiate only the primary lesion and the metastatic lesion causing symptoms
Yes
Radiotherapy dose: 3D conformal radiotherapy and intensity-modulated radiotherapy with volume dose
Volume definition mode, isocentric dose definition mode for conventional irradiation. The total amount of conventional radiotherapy in synchronous radiotherapy is 45-50 Gy, with a single dose of 1.8-2.0 Gy; the recommended dose for radical radiotherapy is 56-60 Gy in synchronous or sequential dosing.
- style=”margin-left: 118pt”>
- Postoperative radiotherapy dose: recommended for clinical target area DT45 to 50.4 Gy per
1.8 Gy for 25 to 28 times; for those with tumors and/or residuals, large-field irradiation followed by localized field reduction for additional DT 5 to 10 Gy.
- style=”margin-left: 62pt”>
- Preoperative radiotherapy dose: recommended DT 41.4 to 45 Gy, 1.8 Gy each time, 23 to 25 times.
- Radical radiotherapy dose: recommended DT 54 to 60 Gy, 2 Gy each time, 27 to 30 times in total.
- Radiotherapy dose for metastases, brain metastases: 30 Gy/10f or 40 Gy/20f or stereotactic radiotherapy.
-
Irradiation techniques: choose different radiotherapy techniques according to the hospital’s radiotherapy equipment, such as conventional radiotherapy, 3D conformal radiotherapy, image guided radiotherapy, and image guided radiotherapy. The radiation technology: according to the hospital’s radiotherapy equipment, different radiotherapy techniques are selected, such as conventional radiotherapy, 3D conformal radiotherapy, intensity modulated radiotherapy, image guided radiotherapy, etc. It is recommended to use advanced technologies such as 3D conformal radiotherapy or intensity modulated radiotherapy to better protect surrounding normal tissues such as liver, spinal cord, kidney and intestine, reduce toxic side effects of normal tissues and improve the tolerance of radiotherapy.
-
Simulated localization: CT simulation is recommended. If CT simulation is not available, conventional simulation positioning must be performed. The position should be fixed, supine. Avoid eating much food 3 hours prior to localization, and oral contrast or intravenous application of contrast will help with CT localization and target area delineation.
- style=”margin-left: 56pt”>
- Multiple field irradiation of 3 fields and more is recommended.
- If intensity-modulated radiotherapy is given, plan validation must be performed.
- Multiple field irradiation of 3 fields and more is recommended.
- style=”margin-left: 118pt”>
- Local dosing can be done using intraoperative radiotherapy or external irradiation techniques.
- Radiation particle implantation therapy is not recommended for routine use.
- style=”margin-left: 62pt”>
-
Synchronous chemotherapy: Tegeo or Capecitabine is preferred as a single agent in synchronous chemotherapy regimens. Clinical studies of combination intravenous chemotherapy can be conducted in hospitals where available.
Tegeo dose (in terms of tegafur): ①body surface area<1.25m2 at 40mg each time; ②body surface area 1.25-1.5m2, 50mg each time; (iii) body surface area ≥
-
m2, 60mg each time.
Capecitabine dose: 800 mg/m2 orally twice daily on day of radiation therapy. Normal tissue limits: lung, V20<25
 ; Heart, V30<30
; Heart, V30<30  ; Spinal cord, Dmax
; Spinal cord, Dmax
≤45Gy; kidney, V20<25
 ; small intestine, V45<195ml; liver, V 30<30
; small intestine, V45<195ml; liver, V 30<30  , Dmean<25Gy.
, Dmean<25Gy.(vi) Targeted therapy.
- style=”margin-left: 48pt”>
- Trastuzumab
-
-
Indications: For HER2 overexpression (immunohistochemical staining of +++, or immunohistochemical staining of +++ with FISH). In patients with advanced gastric or gastroesophageal junction adenocarcinoma with HER2 overexpression (++ immunohistochemical staining or ++ immunohistochemical staining and positive FISH test), trastuzumab is recommended in combination with chemotherapy. The indication population is patients who have not received prior first-line therapy for metastatic disease or patients who have not received prior second-line therapy against HER2 or higher.
-
Contraindications: Prior history of congestive heart failure, high-risk uncontrolled arrhythmias, angina requiring drug therapy, clinically significant valve disease, transmural myocardial infarction on ECG, and poorly controlled hypertension.
- style=”margin-left: 73pt”>
- Pre-treatment evaluation and on-treatment monitoring: trastuzumab adverse reactions
- Pre-treatment evaluation and on-treatment monitoring: trastuzumab adverse reactions
The main effects include cardiotoxicity, infusion reactions, hematologic toxicity, and pulmonary toxicity. Therefore, a thorough assessment of medical history, physical status, baseline tumor status, HER2 status, and cardiac function is required prior to application. The LVEF is absolutely reduced by ≥1% relative to pre-treatment.
16  or LVEF below the local provider’s normal range for this parameter and with an absolute reduction ≥10 relative to pre-treatment
or LVEF below the local provider’s normal range for this parameter and with an absolute reduction ≥10 relative to pre-treatment  Trastuzumab therapy should be discontinued.
Trastuzumab therapy should be discontinued.
- style=”margin-left: 134pt”>
- Caution.
- style=”margin-left: 118pt”>
- According to the ToGA study, for HER2-positive gastric cancer, it is recommended to
5-fluorouracil/capecitabine in combination with cisplatin in combination with trastuzumab. In addition, several phase II clinical studies have evaluated trastuzumab in combination with other chemotherapy regimens, which also have better efficacy and safety, such as paclitaxel, capecitabine in combination with oxaliplatin, tegeo in combination with oxaliplatin, and tegeo in combination with cisplatin. However, the combination with anthracyclines is not recommended.
- style=”margin-left: 62pt”>
-
Patients with HER2-positive advanced gastric cancer after progression of first-line chemotherapy, such as (3) Other HER2-targeted agents include the anti-HER2 monoclonal antibody Paraquel. antibody Pa
Tutuzumab, the small-molecule tyrosine kinase inhibitor lapatinib, and the drug-coupled anti-HER2 monoclonal antibody TDM-1, none of which have yielded positive results in clinical studies and none of which are recommended for clinical use.
- style=”margin-left: 110pt”>
- Apatinib
- style=”margin-left: 62pt”>
-
Apatinib mesylate is a highly selective VEGFR-2 inhibitor that is indicated for the third-line treatment of patients with advanced adenocarcinoma of the stomach or gastroesophageal junction who are in good general condition at the time of treatment with apatinib.
- Contraindications: Same as palliative chemotherapy, but with special attention to patient bleeding tendency, cardio-vascular system underlying disease and renal function.
-
Pre-treatment evaluation and in-treatment monitoring: Adverse effects of apatinib include elevated blood pressure, proteinuria, hand-foot syndrome, bleeding, cardiotoxicity, and hepatotoxicity. The adverse effects of apatinib include elevated blood pressure, proteinuria, hand-foot syndrome, bleeding, cardiotoxicity and hepatotoxicity. The risk of bleeding, ECG and cardiac function, and liver function need to be monitored closely during treatment.
- style=”margin-left: 72pt”>
- Caution.
- Caution.
- Apatinib in combination or alone is not currently recommended for first- and second-line therapy outside of clinical studies.
-
Prospective studies have found prolonged disease control, relapse-free survival, and overall survival in people with early-onset hypertension, proteinuria, or hand-foot syndrome. Therefore, it is important to pay active attention to adverse reactions, manage them throughout, adjust the dose appropriately, and try reapplication with caution.
-
Emphasis on patient education for patients with ECOG ≥ 2, post fourth-line chemotherapy, primary gastric lesions, poor bone marrow reserve, and poorly treated patients. For female patients with ECOG ≥2, after fourth-line chemotherapy, unresected primary gastric lesions, poor bone marrow reserve, old and frail, or thin, a low dose such as 500 mg once daily can be started orally to ensure patient safety and improve compliance.
(vii) Immunotherapy.
With the widespread use of immune checkpoint inhibitors, first-line chemotherapy combined with PD-1 monoclonal antibody in advanced gastric cancer (Checkmate 649 study), and third-line single-agent PD-1 monoclonal antibody therapy have yielded positive results in randomized phase III clinical studies (Attraction
- style=”margin-left: 62pt”>
-
studies), and in the area of second-line, perioperative therapy Several studies related to immune checkpoint inhibitors have also been conducted. Patients are now advised to actively participate in clinical studies.
(viii) Interventional therapy.
Interventional treatment of gastric cancer includes minimally invasive interventions for gastric cancer, liver metastases from gastric cancer, bleeding associated with gastric cancer, and gastric outlet obstruction.
- style=”margin-left: 48pt”>
- Interventional treatment of gastric cancer
Transcatheter arterial embolization (TAE), transcatheter arterial embolization chemotherapy (Transcatheter arterial chemoembolization (TACE), or transcatheter arterial infusion (TACE)
(transcatheter arterial infusion (TAI) chemotherapy can be used for palliative or adjuvant treatment of progressive and nonradiable gastric cancer, but its efficacy is not yet certain and needs to be further confirmed in large, prospective studies.
- style=”margin-left: 48pt”>
- Interventional treatment of liver metastases from gastric cancer
Interventional therapy can be used as a local minimally invasive treatment option for liver metastases from gastric cancer in addition to surgical resection. These include ablation therapy, TAE, TACE, and TAI chemotherapy.
- style=”margin-left: 48pt”>
- Interventional treatment of bleeding associated with gastric cancer
Interventional treatment (e.g., TAE) has unique advantages for gastric cancer-related bleeding, including gastric cancer rupture bleeding, gastric cancer metastasis bleeding, and gastric cancer postoperative bleeding, etc.
- Interventional treatment of gastric cancer
The hemostasis can be accomplished rapidly and efficiently by identifying the location of the bleeding through selective or super-selective arteriography and using the appropriate embolic material to seal it, while relieving the symptoms associated with the bleeding.
- style=”margin-left: 110pt”>
- Interventional treatment of gastric outlet obstruction
Patients with advanced gastric cancer may present with symptoms related to malignant gastric outlet obstruction, and X-ray guided stent implantation is used to relieve symptoms related to the obstruction and improve the patient’s quality of life.
(ix) Chinese medicine treatment.
TCM treatment can help improve post-surgical complications, reduce the adverse effects of radiotherapy and chemotherapy, and improve the quality of life of patients, and can be an important adjunct to gastric cancer treatment. For patients who are too old, too weak, or too sick to tolerate Western medicine, Chinese medicine can be used as an adjunctive treatment.
In addition to traditional herbal medicine, Chinese herbal medicine can also be used to benefit qi, detoxify the body, remove blood stasis, and soften and disperse nodules.
For precancerous lesions detected early (e.g., chronic atrophic gastritis, gastric adenomatous polyps, residual gastritis, gastric ulcers, etc.), Chinese medicine treatment is an option and requires dietary and lifestyle modifications that may delay the onset of tumor.
(x) Supportive therapy.
Supportive/palliative care for gastric cancer aims to relieve symptoms, reduce pain, improve quality of life, manage treatment-related adverse effects, and improve compliance with antitumor therapy. All patients with gastric cancer should be screened, evaluated and treated for symptoms throughout the course of supportive/palliative care. This includes both bleeding, obstruction, pain, nausea/vomiting, etc.
Common physical symptoms should be included, as well as psychological issues such as sleep disturbances, anxiety and depression. At the same time, cancer survivors should be given enhanced guidance and follow-up on relevant rehabilitation.
- style=”margin-left: 110pt”>
- Basic principles of supportive/palliative care for patients with gastric cancer
Providers should integrate supportive/palliative care for gastric cancer throughout the oncology continuum, and all patients with gastric cancer should be screened for the need for supportive/palliative care early in their treatment, at the appropriate time, or based on clinical indications. Supportive/palliative specialists and interdisciplinary multidisciplinary collaborative care teams, including oncologists, supportive/palliative care physicians, nurses, dieticians, social workers, pharmacists, mental health professionals, and other professionals, give patients and families relevant treatment in real time.
- style=”margin-left: 110pt”>
- Management of supportive/palliative care for patients with gastric cancer
- style=”margin-left: 62pt”>
-
Bleeding: Patients with gastric cancer Bleeding includes acute and chronic bleeding. Acute bleeding is a common symptom in patients with gastric cancer and may be caused by direct bleeding from the tumor or from treatment.
-
Acute bleeding should be monitored for vital signs and circulatory status, early fluid resuscitation (blood volume supplementation, vasoactive drugs, etc.), and administration of The patient should be monitored for vital signs and circulatory status, and fluid resuscitation (blood volume supplementation, vasoactive drugs, etc.) should be performed early. Patients with acute severe bleeding (vomiting blood or black stool) should be evaluated immediately with endoscopy.
- While endoscopic therapy may be initially effective, the probability of rebleeding is very high.
-
Popularly available treatment options include injection therapy, mechanical therapy (e.g., endoscopic clips), ablation therapy (e.g., argon plasma coagulation), or a combination of these. coagulation), or a combination of these approaches.
- style=”margin-left: 117pt”>
- Angiographic embolization techniques may be indicated in cases where endoscopic treatment is ineffective.
- style=”margin-left: 62pt”>
- External radiation radiotherapy is effective in controlling acute and chronic gastrointestinal bleeding from multiple small vessels.
-
Chronic blood loss due to gastric cancer can be treated with PPI, hemostatic drugs, and external radiotherapy. For patients with anemia, erythropoietic drugs, iron, folic acid, vitamin B12 and other drugs can be given as appropriate according to the condition.
-
Obstruction: In patients with combined malignant gastric obstruction, the primary goal of supportive/palliative therapy is to reduce nausea/vomiting. The goal is to reduce nausea/vomiting and allow resumption of oral feeding when possible.
- Endoscopy: Placement of an enteral stent to relieve outlet obstruction or an esophageal stent to relieve esophagogastric junction/gastric cardia obstruction.
-
Surgery: either gastrojejunostomy or, in some elective patients, gastrectomy.
- style=”margin-left: 56pt”>
- Some patients may opt for external radiotherapy and chemotherapy.
- Some patients may opt for external radiotherapy and chemotherapy.
-
Gastrostomy may be performed to reduce the symptoms of obstruction when the obstruction is irreversible (not suitable for endoscopic intraluminal dilation or when dilation is ineffective). If the location of the tumor permits, gastrointestinal decompression by percutaneous, endoscopic, surgical or interventional radiological placement of a gastrostomy tube is indicated. In patients with central or distal gastric obstruction and inability to eat, a jejunal nutrition tube may be placed if the tumor location permits.
-
If ascites is present, drain the ascites before placing a gastrostomy tube to reduce the risk of infection-related complications.
- style=”margin-left: 72pt”>
- Pain
- style=”margin-left: 56pt”>
- Patient complaints are the gold standard for pain assessment, and analgesic treatment must be preceded by
- Pain
Assess the intensity of the patient’s pain. The preferred method of pain assessment is numerical pain grading, which includes the etiology, characteristics, nature, aggravating or relieving factors, the impact of pain on the patient’s daily life, and the efficacy and side effects of analgesic treatment.
- style=”margin-left: 62pt”>
-
The WHO three-step analgesic principle remains the most basic principle for clinical analgesic treatment. The opioids are the cornerstone of cancer pain treatment, with the addition of glucocorticoids and anticonvulsants as adjuvant drugs when necessary, and attention to the adverse effects of analgesic drugs. 3) More than 80
 cases of cancer pain can be relieved by pharmacological treatment, with a few patients
cases of cancer pain can be relieved by pharmacological treatment, with a few patientsNon-pharmacologic analgesia, including surgery, radiation analgesia, and minimally invasive interventions, is needed, and the effectiveness of analgesia should be dynamically assessed and interdisciplinary collaboration should be actively pursued.
- style=”margin-left: 72pt”>
- Nausea/vomiting.
- Nausea/vomiting.
-
Drug selection for chemotherapy-induced nausea/vomiting should be based on the risk of emetics in the treatment regimen, prior The choice of medication for chemotherapy-induced nausea/vomiting should be based on the risk of emesis with the treatment regimen, previous experience with antiemesis, and the patient’s own factors, with adequate dynamic assessment for appropriate management.
- Nausea/vomiting may be associated with GI obstruction and should be evaluated with endoscopy or fluoroscopy to determine if obstruction is present.
- Consider other potential emesis-causing factors: e.g., vestibular dysfunction, brain metastases, electrolyte imbalance, adjuvant medications (including opioids), gastric muscle bradycardia: tumor itself, chemotherapy-induced or caused by other causes (e.g., diabetes mellitus), malignant ascites. diabetes mellitus), malignant ascites, psychophysiology (including anxiety, anticipatory nausea/vomiting).
- Lifestyle management may help to reduce nausea/vomiting, such as eating smaller, more frequent meals, making healthy food choices, controlling food intake, and avoiding cold and heat. Diet sessions may also
Helpful.
- style=”margin-left: 62pt”>
-
Nutrition: First, the nutritional status of each tumor patient needs to be correctly assessed. In order to objectively evaluate the efficacy of nutritional therapy, it is necessary to continuously re-evaluate during the treatment process in order to timely adjust the treatment plan.
- style=”margin-left: 56pt”>
- Patients with malignant tumors should be screened for nutritional risk as soon as they are clearly diagnosed.
- Patients with malignant tumors should be screened for nutritional risk as soon as they are clearly diagnosed.
Screening.
- style=”margin-left: 118pt”>
- The most widely used nutritional risk screening tools for malignancy at this stage are
NRS2002 and PG-SGA.
- style=”margin-left: 62pt”>
-
Those with NRS <3, although not at nutritional risk, should be screened once a week during their Those with an NRS ≥3 are at nutritional risk and require individualized nutrition-based planning and nutritional interventions based on the patient's clinical condition.
-
No intervention is needed for PG-SGA scores 0 to 1, and routine follow-up and evaluation is maintained during treatment. A PG-SGA score of 2 to 3 requires patient or patient family education by a dietitian, nurse practitioner, or physician and may include pharmacologic interventions based on the presence of symptoms and laboratory findings. a PG-SGA score of 4 to 8 requires intervention by a dietitian and may include nutritional interventions in conjunction with a physician and nurse practitioner, depending on the severity of symptoms. a PG-SGA score of 9 requires urgent symptom improvement and/or concurrent nutritional interventions. or concurrent nutritional interventions.
-
History, physical examination and some laboratory tests are useful to understand the causes and severity of malnutrition in patients with malignancy. The reason and severity of malnutrition in patients with malignant neoplasm can be assessed by comprehensive nutrition assessment.
- style=”margin-left: 56pt”>
- Nutritional risk screening and comprehensive nutritional assessment should be combined with the impact of antitumor therapy.
- Nutritional risk screening and comprehensive nutritional assessment should be combined with the impact of antitumor therapy.
Imaging efficacy evaluation should be performed simultaneously to fully assess the benefit of antitumor therapy.
- style=”margin-left: 134pt”>
- Psychological distress.
- style=”margin-left: 62pt”>
-
Psychological distress is the result of psychological (i.e., cognitive, behavioral, emotional), social, mental, and/or somatic experiences that may affect the patient’s ability to cope with tumors, somatic symptoms, and treatment. Psychological distress includes such things as depression, anxiety, panic, social isolation, and existential crisis.
- Psychological distress should be recognized, monitored documented, and addressed in a timely manner at all stages of the disease and in all settings.
-
Psychological distress should be assessed and managed according to clinical practice guidelines. The interdisciplinary, collaborative, multidisciplinary treatment team should be formed to manage and treat the psychological distress of patients and families.
- style=”margin-left: 72pt”>
- Anorexia/hyperalgesia.
- Anorexia/hyperalgesia.
-
Assess the cause and severity of weight loss and recommend early treatment of reversible causes of anorexia ( Oral infections, psychological causes, pain, constipation, nausea/vomiting, etc.), evaluation of medications that affect eating, etc.
-
Consider appropriate exercise program and active nutritional support (enteral or parenteral nutrition).
- style=”margin-left: 72pt”>
- Other symptoms.
- Other symptoms.
-
Constipation: When constipation occurs, evaluate the cause and severity of constipation, expel obstruction, fecal If constipation occurs, assess the cause and severity of constipation, remove obstruction, fecal blockage, and treat other causes of constipation. If other causes are ruled out, laxatives, gastrointestinal motility drugs, enemas, etc. may be given. Active prophylaxis, such as drinking more water, exercising, and prophylactic medication.
- style=”margin-left: 56pt”>
- Sleep/wake disorders: assess the type and severity of sleep/wake disorders.
- Sleep/wake disorders: assess the type and severity of sleep/wake disorders.
Extent, patient fear and anxiety of death/illness, and treatment-related influences. Provide sleep hygiene education; provide cognitive behavioral therapy treatment. Medication should be given under professional supervision for refractory sleep/wake disorders.
- style=”margin-left: 110pt”>
- Counseling on health behaviors for gastric cancer survivors
- style=”margin-left: 62pt”>
-
Maintaining a lifelong The patient should be monitored regularly, encouraged to eat less and more often, referred to a dietitian or nutrition unit for individualized counseling if necessary, and attended to and actively evaluated for medical and/or psychosocial factors contributing to weight loss, especially after gastric cancer surgery.
- Focus on a healthy diet of plant-based origin, adjusted as needed for treatment sequelae (e.g., dumping syndrome, bowel dysfunction).
-
Adopt a healthy lifestyle and engage in appropriate physical activity. Goal: Try to get at least 30 minutes of moderate intensity activity daily.
- style=”margin-left: 72pt”>
- Limit alcohol consumption.
- Smoking cessation is recommended.
(xi) Follow up.
The primary purpose of follow-up/surveillance is to detect metastatic recurrence that is still amenable to potentially curative aimed therapy, to detect tumor recurrence or second primary gastric cancer earlier, and to intervene in a timely manner to manage it in order to improve overall patient survival and improve quality of life. There is no high-level evidence-based medical evidence to support which follow-up/surveillance strategy is optimal. Follow-up should be based on the principles of patient individualization and tumor staging, and routine oncologic follow-up/surveillance is not advocated for patients whose medical condition does not allow for the anticancer therapy needed once recurrence occurs.
The main purpose of gastroscopic follow-up after gastric cancer surgery is to detect neoplastic tumors under gastroscopy
- Limit alcohol consumption.
Tumor or recurrence of the primary tumor, rarely local recurrence of the gastric anastomosis, can be observed under gastroscopy and a local tissue biopsy of the stomach can be taken to determine tumor recurrence. Gastroscopy strategy: Gastroscopy is recommended within 1 year after surgery, and each gastroscopy biopsy should be repeated within 1 year if there is evidence of high-grade atypical hyperplasia or recurrence of gastric cancer. It is recommended that patients undergo gastroscopy once a year. For those who develop macrocytic anemia after total gastrectomy, vitamin B12 and folic acid should be supplemented.
PET-CT, MRI are recommended only for clinically suspected recurrence in combination with negative conventional imaging, e.g., persistent elevated CEA and negative abdominal CT or ultrasound. PET-CT is not currently recommended as a routine follow-up/monitoring tool. The specific method and frequency of follow-up is detailed in Table 7.
Table 7 Post-treatment follow-up requirements and guidelines for gastric cancer
|
purpose |
Basic strategy |
Follow-up after radical surgery for early gastric cancer |
Frequency of follow-up visits Every 6 months for the first 3 years, then every 1 year until 5 years after surgery |
|
Content of follow-up visit: (no specific reference means each time) a) Clinical history
|
|
|
Radical surgery for progressive gastric cancer |
Frequency of follow-up/monitoring |
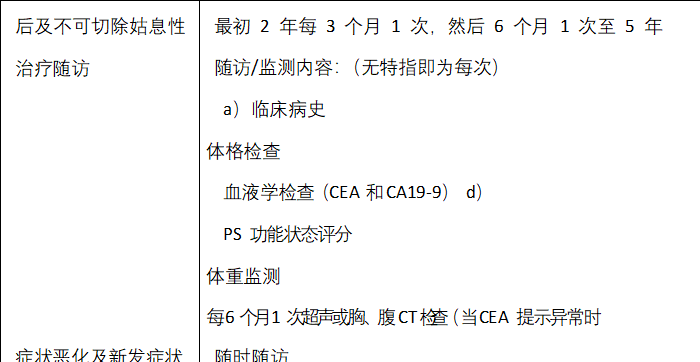 < span style="font-size:14pt">)
< span style="font-size:14pt">)
Appendix I: AJCC/UICC TNM Staging of Gastric Cancer (8th Edition) Appendix II: Histologic Types and Grading of Gastric Cancer
Appendix III: Gross staging of gastric cancer
Appendix IV: Standard template for reporting pathology of gastric cancer Appendix V: Guidelines for reporting imaging of gastric cancer
Appendix VI: Diagnostic imaging process for gastric cancer Appendix VII: Criteria for grouping lymph nodes in gastric cancer
Appendix VIII: Criteria for grouping lymph nodes in different sites of gastric cancer Appendix IX: Anatomical site coding of gastric tumors
Appendix X: Schematic diagram of the gastroesophageal junction
Appendix XI: Siewert staging of tumors of the gastroesophageal junction Appendix XII: CT staging signs of gastric cancer and report reference Appendix XIII: Ultrasound endoscopic (EUS) staging signs of gastric cancer Appendix XIV: Common systemic treatment options for gastric cancer
Appendix XV: Commonly used targeted therapeutic agents for gastric cancer
Appendix XVI: Basic criteria for determining the efficacy of radiation and chemotherapy for gastric cancer
Appendix XVII: Assessment of the efficacy of preoperative adjuvant therapy for tumor (tumor regression grading TRG)
Appendix I: AJCC/UICC TNM staging of gastric cancer (8th edition)


Primary Tumor (T)
Tx Primary tumor could not be evaluated
T0 No evidence of primary tumor
Tis carcinoma in situ: intraepithelial tumor without invasion of the lamina propria, highly atypical hyperplasia T1 Tumor invading the lamina propria, myxomucosa or submucosa
T1a Tumor invading lamina propria or myxomucosa T1b Tumor invading submucosa
T2 Tumor invades the lamina propria*
T3 Tumor penetrates the subplasmic connective tissue without yet invading the visceral peritoneum or adjacent structures** , **** T4 Tumor invades the plasma membrane (visceral peritoneum) or adjacent structures**, ***
 T4a Tumor invasion of the plasma membrane (visceral peritoneum) T4b Tumor invasion of adjacent structures
T4a Tumor invasion of the plasma membrane (visceral peritoneum) T4b Tumor invasion of adjacent structures
Regional lymph nodes (N)
Nx regional lymph nodes could not be evaluated
N0 regional lymph nodes without metastasis
N1 1 to 2 regional lymph nodes with metastasis
N2 3 to 6 regional lymph nodes with metastasis
N3 7 or more regional lymph nodes with metastasisN3a 7 to 15 regional lymph nodes with metastasis
 N3b 16 or more regional lymph nodes with metastases distant metastases (M)
N3b 16 or more regional lymph nodes with metastases distant metastases (M)
M0 No distant metastases
 M1 Histologic grading with distant metastases (G)
M1 Histologic grading with distant metastases (G)
Gx grading cannot be assessed
G1 Highly differentiated
G2 Moderately Divergent
G3 hypofractionated, undifferentiated


*Tumors can penetrate the lamina propria to reach the gastrocolic ligament or hepatogastric ligament or greater and lesser omentum, but does not penetrate the overlying
the visceral peritoneum covering these structures. In this case, the primary tumor is staged as T3, and if it penetrates the visceral peritoneum covering the gastric ligament or omentum, it should be classified as stage T4.
**Adjacent structures of the stomach include the spleen, transverse colon, liver, diaphragm, pancreas, abdominal wall adrenal glands, kidneys, small
intestine, and the retroperitoneum.
***Tumors that extend into the duodenum or esophagus through the stomach wall are not considered for invasion of adjacent structures, but rather apply any
maximal depth of infiltration at these sites for staging.
|
Clinical staging (cTNM) |
|||||
|
0 period |
Tis |
N0 |
M0 |
||
|
Phase I |
T1 |
N0 |
M0 > |
||
|
T2 |
N0 |
< span style="font-family:imitation-song; font-size:12pt">M0 |
|||
|
Phase IIA |
T1 |
N1 to 3 |
N1 to 3 |
M0 | |
|
T2 |
N1 to 3 |
M0 |
|||
|
IIB period |
T3 |
N0 |
|||
|
N0 |
N0 |
M0 |
|||
|
III |
T3 |
T3 |
N1~3 |
M0< |
|
|
T4a< |
N1 to 3 |
M0 |
|||
|
IVA period |
T4b |
Any N |
M0 |
||
|
< span style="font-family:imitation-song; font-size:12pt">ⅣB period |
< span style="font-family:imitation-song; font-size:12pt">any T |
< span style="font-family:imitation-song; font-size:12pt">any N |
< span style="font-family:imitation-song; font-size:12pt">M1 |
||
|
Pathological staging (pTNM) |
|||||
|
0 period |
Tis |
N0 |
M0 |
||
|
Phase IA |
Phase IA |
T1 |
N0 |
M0 |
|
|
Ib Phase |
T1 |
N1 |
|||
|
N0 |
M0 |
||||
|
Phase IIA |
T1 |
T1 |
N2 |
M0 > |
|
|
T2 |
N1 |
< span style="font-family:imitation-song; font-size:12pt">M0 |
|||
|
< span style="font-family:imitation-song; font-size:12pt">T3 |
N0 |
M0 |
|||
|
IIB period |
T1 |
N3a |
N3a< |
M0 |
|
|
T2 |
N2 |
M0 |
|||
|
T3 |
N1 |
M0 |
|||
|
T4a |
T4a |
N0 |
M0 > |
||
|
IIIA period |
T2 |
T2 | N3a |
M0 |
|
|
T3 |
N2 |
M0 |
|||
|
T4a |
N1 |
M0 |
|||
|
T4a |
T4a |
N2 |
M0 |
||
|
T4b |
N0 |
M0 |
|||
|
IIIB period |
T1 |
N3b |
M0 |
||
|
T2 |
T2 |
N3b |
M0 |
||
T3N3aM0T4aN3aM0T4bN1M0T4bN2M0 Stage IIIC T3N3bM0T4aN3bM0T4bN3aM0T4bN3bM0 Stage IV Any T any NM1
Post neoadjuvant therapy staging (ypTNM) Phase I T1N0M0T2N0M0T1N1M0 Phase II T3N0M0T2N1M0T1N2M0T4aN0M0T3N1M0T2N2M0T1N3M0 Phase III T4aN1M0T3N2M0T2N3M0T4bN0M0T4bN1M0T4aN2M0T3N3M0T4bN2M0T4bN3M0T4aN3M0 Stage IV any T NM1 notes
To achieve accurate staging, the number of regional lymph nodes should be ≥16, preferably ≥30.
- style=”margin-left: 62pt”>
-
If the tumor involves the esophagogastric junction If the center of the tumor is on the esophageal side of the esophagogastric junction or within 2 cm of the gastric side (Siewert’s type I and II), it is staged as esophageal cancer; if the center of the tumor is outside 2 cm of the proximal stomach (Siewert’s type III), it is staged as gastric cancer. If the center of the tumor is within 2 cm of the proximal stomach but does not involve the esophagogastric junction, it is staged as gastric cancer.
- Staging of neuroendocrine tumor (NET) of the stomach is based on the TNM staging of gastric neuroendocrine tumor.
- This staging does not apply to non-epithelial tumors such as lymphoma, sarcoma, and gastrointestinal mesenchymal tumors.
- Staging of neuroendocrine tumor (NET) of the stomach is based on the TNM staging of gastric neuroendocrine tumor.
Appendix II: Histologic Types and Grading of Gastric Cancer
Histologic Types of Gastric Cancer WHO (refer to 2010 edition of WHO Classification of Tumors of the Digestive System)
|
Histological type |
ICD-O code |
|
Cancer |
|
|
Cancer |
8140/3 |
|
8140/3 |
|
|
papillary adenocarcinoma |
8260/3 |
|
Tubular adenocarcinoma |
8211/3 |
|
Mucinous Adenocarcinoma |
8480/ 3 |
|
Low-adherent carcinoma (including indolent cell carcinoma and other variants) |
8490/3 |
| < p>Mixed Adenocarcinoma |
8255/3 |
|
Adenosquamous carcinoma |
8560/3 |
|
Carcinoma with lymphoid interstitium (medullary carcinoma) |
8512/3 |
|
Hepatocellular adenocarcinoma |
8576/3 |
|
Squamous cell carcinoma |
8070/3 |
|
Undifferentiated carcinoma |
8020/3 |
|
Neuroendocrine Tumors |
|
|
Neuroendocrine Tumor (NET) |
|
|
NET G1 |
8240/3 |
|
NET G2 |
8249/3 |
|
Neuroendocrine Carcinoma (NEC) |
8246/3 |
|
Small cell carcinoma |
8041/3 |
|
Large cell neuroendocrine carcinoma |
8013/3 |
|
Mixed glandular-neuroendocrine carcinoma < |
8244/3 |
|
8241/3 |
|
|
Gastrin-secreting NET (gastrinoma) |
8153/3 |
Appendix III: Broad Staging of Gastric Cancer
Recommended Paris Staging for Early Stage Gastric Cancer
Ruminal type (0-Ⅰ): subdivided into tipped augmentation (0-Ⅰp) and non-tipped augmentation (0-Ⅰs); superficial type (0-Ⅱ): subdivided into superficial augmentation (0-Ⅱa), superficial flat type (0-IIb) and
Superficial depressed type (0-IIc). Lesions with both superficial elevation and superficial depression are classified into superficial depression + superficial elevation type (type 0-IIc+IIa) and superficial elevation + superficial depression type according to the ratio of superficial elevation/superficial depression
(0-IIa+IIc type).
Depressed (ulcerated) type (0-III): lesions with a combination of depression and superficial depression are divided into superficial depression + depression type (0-IIc+III) and depression + superficial depression type (0-III) according to the ratio of depression/ superficial depression. type (0-III+IIc type).
The common Borrmann staging of progressive gastric cancer: type I (nodular bulge), type II (limited ulcer), type III (infiltrative ulcer), type IV (diffuse infiltrative)
Appendix IV: Standard template for pathology report of gastric cancer
Record of routine description of gross examination of specimens of gastric and esophagogastric union cancer
Excised specimen (whole stomach, large stomach or remnant stomach): length of greater curvature cm, length of lesser curvature cm, with pyloric ring/duodenum/lower esophagus, length cm; in (esophagogastric junction/fundus/body/sinus) (including visual description): cm from superior margin, cm from inferior margin, size — x– x– cm, cross-sectional features; depth of infiltration to; involvement/non-involvement of the pyloric ring/esophagogastric junction. (In case of carcinoma of the esophagogastric junction, the center of the tumor should be described as cm from the esophagogastric junction line). What is seen in the esophageal mucosa/muscular wall next to or around the mass (erosion/roughness/granularity/depression/plaque//negative if necessary). Lymph nodes found in the greater curvature (several/many/dozen/odd), diameter to cm; lymph nodes found in the lesser curvature (several/many/dozen/odd), diameter to cm. greater omentum, size –
×—×—cm, with or without tumor and lymph nodes. Contents of pathological diagnosis report of gastric cancer
1. Tumor
- style=”margin-left: 94pt”>
- Tissue typing
- Tissue grading
- Depth of infiltration
- Esophageal or duodenal infiltration (if excised)
- Vascular infiltrate
- style=”margin-left: 62pt”>
-
Perineural infiltrate 2. Cut margin
- Proximal
- Distant end
-
Other pathology seen
- Chronic gastritis
- Enterization
- Atypical hyperplasia
- atrophy
- Adenoma
- Polyp
- Helicobacter pylori
- Other
- Chronic gastritis
- Regional lymph nodes (including small bend, large bend, large omentum and separately sent lymph nodes)
- Proximal
- style=”margin-left: 94pt”>
- Total
- style=”margin-left: 62pt”>
-
Number of involved 5. Distant metastases
- Other tissues/organ
- Special auxiliary findings (histochemical staining, immunohistochemical staining, etc.)
Difficult pathology is referred to a higher level hospital for consultation (provide information such as the original pathology report and tissue block site to verify the correctness of the submitted sections to reduce errors, provide adequate lesion sections or wax blocks, and intraoperative views, etc.).
- Other tissues/organ
Appendix V: Guidelines for imaging reports of gastric cancer
Principle: To report comprehensive information related to clinical diagnosis and treatment around cTNM staging of gastric cancer, and to leverage the value of MDT in image interpretation.
Primary Foci
Site (esophagogastric junction, fundus, gastric body, sinus, pyloric duct, greater curvature, lesser curvature, anterior wall, posterior wall), morphology (mass, limited ulcer, infiltrating ulcer, diffuse thickening), thickness.
density (specific signs such as mucinous adenocarcinoma), enhancement features, depth of invasion, mucosal and plasma surface conditions, location of proximal/distal involvement borders, junction with normal gastric wall, relationship to adjacent organs.
Lymph nodes
Referring to the report of the subgroup of the statute for the management of gastric cancer of the Japanese Society of Gastric Cancer.
Report the number of lymph nodes with clear signs of metastasis (or the range of numbers with reference to N-stage), maximum lymph node length and diameter, morphology, border, and enhancement.
Distant metastases
Location, distribution, morphology, size, density and enhancement characteristics of metastases, peritoneal morphology and ascites. In case of controversy, it was submitted to the MDT for joint discussion.
Appendix VI: Diagnostic imaging process for gastric cancer
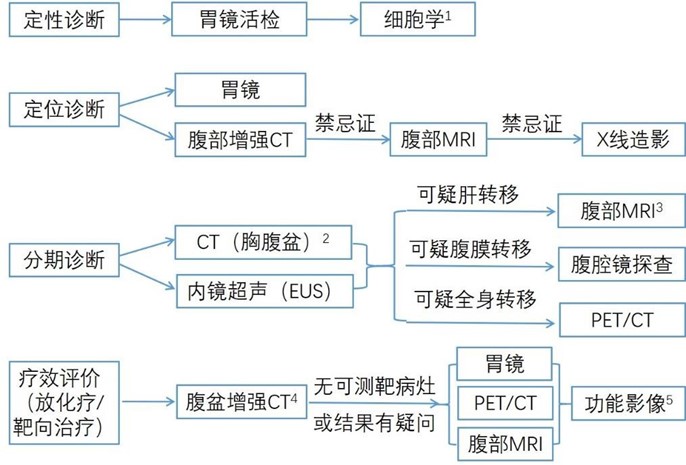
- style=”margin-left: 62pt”>
- When repeated biopsies by gastroscopy do not confirm the pathological diagnosis, cytology of peritoneal/pleural fluid or pathology of metastases can be used as a qualitative diagnostic aid .
- Abdominopelvic CT should be enhanced, and chest CT should be performed as a routine plain scan with additional enhancement if mediastinal lymph node metastasis is suspected.
- As a means of further examination when liver metastases are suspected on CT, the use of hepatocyte-specific contrast is recommended when available and may improve the sensitivity of the diagnosis of liver metastases.
- Long diameter of hepatopulmonary or peritoneal metastatic nodes>1cm or short diameter of lymph nodes>1.5cm as target lesions according to RECIST 1.1 criteria. The thickness of the primary site can be used as a reference for evaluation, but is not considered as a target lesion.
- Small sample studies have shown that imaging functional imaging parameters such as magnetic resonance diffusion imaging ADC values and dual-energy CT iodine concentration values can assist in evaluating the efficacy of gastric cancer.
Appendix VII: Criteria for lymph node grouping in gastric cancer
|
Group 1 |
(No. 1) |
Right lymph node of cardia |
||
|
< span style="font-family:imitation-song; font-size:12pt">(No. 1) |
(No. 2) |
Left lymph node of cardia |
Group 3 |
(No. 3) |
Little curved lymph nodes |
|
Group 4sa |
(No. 4sa) |
left group of greater curvilinear lymph nodes (along the short gastric artery) |
||
|
Group 4sb |
(No. 4sb) < /td> |
Left group of greater curvilinear lymph nodes (along the left artery of the gastric omentum) |
||
|
Group 4d |
(No. 4d) |
Right group of large curved lymph nodes ( along the right artery of the gastric omentum) |
||
|
Group 5 |
(No. 5) |
(No. 5) |
Suprapyloric lymph nodes | |
|
Group 6 |
(No. 6) |
Subpyloric lymph nodes |
||
|
Group 7 |
(No. 7) |
Lymph node of the left gastric artery |
||
|
Group 8a |
Group 8a |
(No. 8a) |
Lymph nodes in the anterior superior aspect of the common artery |
hepatic anterior superior common artery lymph node |
|
Group 8b |
(No.8b) |
(No.8b) |
Posterior common hepatic artery lymph node | |
|
Group 9 |
(No. 9) |
peri-abdominal artery lymph nodes |
||
|
< span style="font-family:imitation-song; font-size:12pt">(No. 9) | Group 10 |
(No. 10) |
Splenic hilar lymph node |
Group 11p |
(No. 11p) |
Proximal splenic artery lymph nodes |
|
Group 11d |
< span style="font-family:imitation-song; font-size:12pt">Lymph nodes distal to splenic artery |
|||
|
Group 12a |
(No. 12a) |
(No. 12a) < /td> |
Lymph nodes of the hepatoduodenal ligament (along the hepatic artery) |
|
|
Group 12b |
(No. 12b) |
Hepatoduodenal ligamentous lymph nodes (along the bile duct) |
||
|
Group 12p |
(No. 12p) |
Lymph nodes of the hepatoduodenal ligament (along the portal vein) |
||
|
Group 13 |
(No. 13) |
Pancreatic head posterior lymph node |
||
|
(No. 14v) |
Lymph nodes along the superior mesenteric vein > |
|||
|
Group 14a |
(No. 14a) |
(No. 14a) |
Lymph nodes along the superior mesenteric artery |
|
|
Group 15 |
(No. 15) |
peri-colonic middle artery lymph nodes |
||
|
Group 16a1 |
(No. 16a1) |
Periaortic lymph node a1 | ||
|
Group 16a2 |
(No. 16a2) |
Group 16a2 |
periaortic lymph nodes a2 |
|
|
Group 16b1 Group 16b1 |
(No. 16b1) |
(No. 16b1) |
periaortic lymph node b1 |
|
|
Group 16b2 |
(No. 16b2) |
Periaortic lymph node b2 | ||
|
Group 17 |
(No. 17) |
Group 17 |
size:12pt”>Anterior pancreatic head lymph node |
|
|
Group 18 |
(No. 18) |
< span style="font-family:imitation-song; font-size:12pt">Subpancreatic lymph nodes |
||
|
Group 19 |
(No. 19) |
Subphrenic lymph nodes |
||
|
< span style="font-family:imitation-song; font-size:12pt">Subphrenic lymph nodes |
||||
| Group 20 |
(No. 20) |
Esophageal fissure lymph node |
||
|
Group 110 |
(No. 110) |
Paraesophageal lymph nodes in the lower chest |
||
|
Group 111 |
(No. 111) |
< span style="font-family:imitation-song; font-size:12pt">Supradiaphragmatic lymph nodes |
||
|
Group 112 |
(No. 112) |
Posterior mediastinal lymph nodes |
p>
 Appendix VIII: Criteria for the staging of various groups of lymph nodes in different sites of gastric cancer
Appendix VIII: Criteria for the staging of various groups of lymph nodes in different sites of gastric cancer
|
Stomach cancer sites
Lymph node group |
< span style="font-family:imitation-song; font-size:12pt">LMU MUL MLU UML |
LD L |
LM M ML |
MU UM |
U |
E+ |
||
|
No.1 |
1 |
< span style="font-family:imitation-song; font-size:12pt">2 |
1 |
1 |
1 |
|||
|
No.2 |
1 |
M |
3 |
1 |
1 |
|||
|
No.3 |
1 |
1 |
1 |
1 |
1 |
|||
|
No.4sa |
1 |
M |
3 |
1 |
||||
|
No.4sb |
No.4sb | No.4sb |
1 |
3 |
1 |
1 |
1 |
|
|
No.4d |
1 |
1 |
1 |
1 |
2 |
|||
|
No.5 |
1 |
1 |
1 > |
1 |
3 < /td> | |||
|
No.6 |
1 |
1 |
1 |
1 |
3 |
|||
|
No.7 |
2 |
2 |
2 |
2 |
2 > |
|||
|
No.8a |
2 < /td> |
2 |
2 |
2 |
||||
|
No.8b |
3 |
3 |
3 |
3 |
3 |
|||
|
No.9 |
2 |
2 |
2 |
2 |
2 |
|||
|
No.10< /p> |
2 |
M < /td> |
3 |
2 |
2 | |||
|
No.11p |
No.11p |
2 |
2 |
2 |
2 |
|||
|
No.11d |
2 |
M |
3 |
2 |
2 |
|||
|
No.12a |
2 |
“border-top: none; border-left: none; border-bottom: solid black 0.5pt; border-right: solid black 0.5pt”>
2 |
2 |
3 |
||||
|
No.12b |
3 |
3 |
3 |
3 |
3 |
|||
|
No.12p |
3 |
3 |
3 |
3 |
3 > |
|||
|
No.13 |
3 < /td> |
3 |
3 |
M |
||||
|
No.14v |
2 |
2 |
3 |
3 |
M |
|||
|
No.14a |
M |
M |
M |
M |
M |
|||
|
No.15< /p> |
M |
M < /td> |
M |
M |
M |
< span style="font-family:imitation-song; font-size:12pt">M |
||
|
No.16a1 |
No.16a1 | M |
M |
M |
M |
|||
|
No.16a2 |
3 |
3 |
3 |
3 |
3 |
|||
|
No.16b1 > |
3 |
3 |
3 |
3 |
|
No.16b2 |
M < /td> |
M |
M |
M |
M |
||
|
No.17 |
M |
M |
M |
M |
M |
||
|
No.18 |
M |
M |
M |
M |
M > |
||
|
No.19 |
3 < /td> |
M |
M |
3 |
2 |
||
|
No.20< /p> |
3 |
M < /td> | M |
3 |
3 |
1 |
|
|
M |
M |
M |
M |
M |
3 |
||
|
No.111 |
M |
M |
M |
M |
M |
< span style="font-family:imitation-song; font-size:12pt">M |
3 |
|
No.112 |
M < /td> |
M |
M |
M |
3 |
Appendix IX: Anatomical site coding of gastric tumors
Coding |
Description |
|
C16.0 |
Cardia, Gastroesophageal Junction* |
C16.1 |
Stomach base |
C16.2 |
胃体 |
|
C16.3 |
Gastric sinus |
|
C16.4 |
Pylons |
C16.5 |
Small curvature of the stomach, unspecified |
|
C16.6 |
Great Curvature of the Stomach, Unspecified |
|
C16.8 |
Partial overlapping lesions of the stomach |
|
C16.9 |
Stomach, unspecified |
Appendix X: Schematic diagram of the gastroesophageal junction
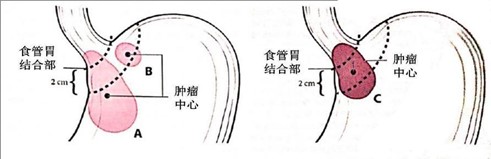
- style=”margin-left: 127pt”>
- The center of the tumor is >2 cm from the EGJ into the proximal stomach, and TNM staging should be performed according to the stomach.
- style=”margin-left: 127pt”>
- Cardia carcinoma without EGJ involvement (tumor center <2cm from EGJ) should be staged by TNM according to the stomach.
- style=”margin-left: 127pt”>
- Proximal gastric cancer involving EGJ with tumor center <2cm from EGJ is staged by TNM as esophageal cancer
Appendix XI: Siewert typing
Siewert typing: a typing proposed by Siewert et al. based on the anatomical features of the esophagogastric junction, also known as the Munich typing. Siewert’s typing is based on the anatomical features of the esophagogastric junction. They believe that adenocarcinoma of the distal esophagus and adenocarcinoma of the cardia should belong to the same disease, that is, adenocarcinoma of the esophagogastric junction. Adenocarcinoma of the esophagogastric junction is an adenocarcinoma with the center of the tumor located within 5 cm above and below the anatomical esophagogastric junction (the anatomical esophagogastric junction is the site where the tubular esophagus becomes the cystic stomach, i.e., the end of the esophagus and the beginning of the stomach, which corresponds to the level of the Hitchcock’s angle or the peritoneal reflex or the lower edge of the esophageal sphincter, and does not necessarily correspond to the histological squamocolumnar junction). It can be divided into 3 types.
Type I: equivalent to distal esophageal adenocarcinoma, with the center of the tumor located 1-5 cm above the esophagogastric junction. Type II: equivalent to pancreatic adenocarcinoma, with the center of the tumor located 1cm above to 2cm below the esophagogastric junction. Type III: equivalent to subcardia adenocarcinoma, with the center of the tumor located 2 to 5 cm below the esophagogastric junction.
Appendix XII: CT staging signs and report reference for gastric cancer
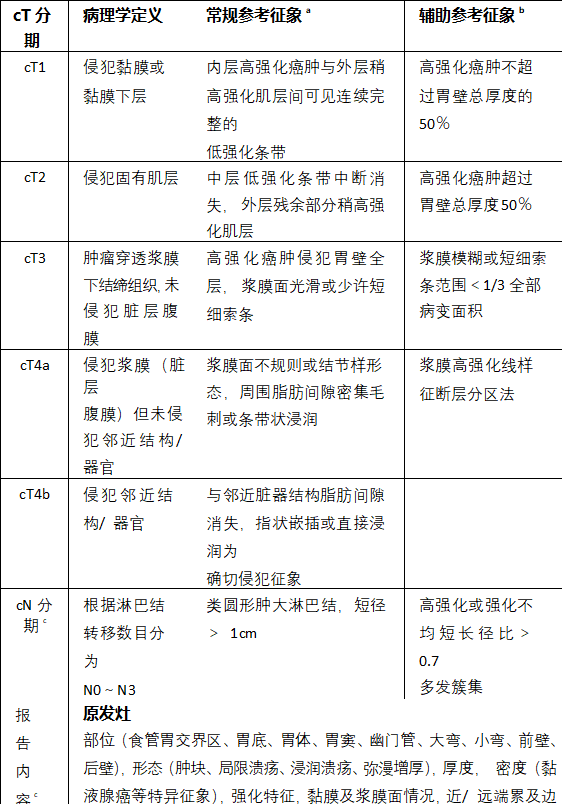 1. Gastric Cancer CT Staging Signs and Report Reference
1. Gastric Cancer CT Staging Signs and Report Reference
Appendix XIII: Ultrasound endoscopic (EUS) staging signs of gastric cancer
|
uT staging |
Definition of pathology |
Major reference signs |
Remarks |
|
uT1a |
violating the intrinsic layer or mucosal muscle layer |
Thickening of the second layer (mucosal layer) in the dark area |
Using high frequency ( 12MHz+) EUS probe theoretically helps to distinguish uT1a from uT1b |
|
uT1b |
invasion of the submucosa |
The thickened dark area extends from the second layer (mucosal layer) to the third layer (submucosal layer) but has not yet reached the fourth layer (solid layer). with muscle layer) |
|
|
invasion of intrinsic muscle layer |
Thickened dark areas reached but not yet penetrated the fourth layer and the outer layer retains a smooth echo boundary |
||
|
uT3 |
The tumor penetrated the subplasma connective tissue without invading the visceral abdominal layer. Membrane |
The structure of each layer is completely lost, but the outermost part retains a smooth hyperechoic band (plasma membrane layer) |
|
|
uT4a |
invasion of the plasma membrane (dirty peritoneum) but not adjacent structures /organs |
Disappearance of structures in all layers, along with disappearance of the hyperechoic band in the plasma layer, or visible burr with clear breakthrough of strong echogenic lines in the plasma layer sign or crabfoot sign |
|
|
violation of neighboring structures /organ |
Whole layer involvement and junction with adjacent organs The echogenic boundaries between structures (aorta, pancreas, liver, etc.) are absent |
||
|
uN Staging |
According to the number of lymph node metastases, they are classified as N0 to N3 |
Circular, well-defined hypoechoic structures >10mm in diameter are usually suggestive of malignant lymph nodes |
< span style="font-family:imitation-song; font-size:12pt">If puncture can be performed without going through the tumor, EUS-FNA is highly recommended for clear gonorrhea. Bar node metastasis |
|
uM Staging |
Divided into M0 and M1 based on whether they are distantly transferred |
EUS can sometimes detect partial intrahepatic metastases or find perigastric ascites, which may be a possible manifestation of M1 |
< span style="font-family:imitation-song; font-size:12pt">Intrahepatic metastases can be clearly identified by EUS-FNA, but diagnosed by the presence of ascites signs M1 is sometimes unreliable |
>
Appendix XIV: Common systemic treatment options for gastric cancer
Cisplatin + fluorouracil-based
|
PF |
Cisplatin 75-100mg/m >2, IV, Day 1 5-Fluorouracil 750-1000mg/(m< span style="font-size:6pt">2-d), continuous intravenous injection for 24 hours, days 1 to 4 Repeat every 28 days |
|
Cisplatin 50mg/m2, IV, Day 1 Calcium folinic acid 200mg/m2, IV, Day 1 5-Fluorouracil 2000mg/m2, continuous intravenous infusion for 24 hours, day 1 Repeat every 14 days |
|
|
XP < span style="font-size:12pt">Cisplatin 80mg/m2, IV, Day 1 Capecitabine 1000mg/m2 Orally, twice daily, days 1 to 14 Repeat every 21 days |
|
|
SP Cisplatin 60mg/m2, IV, Day 1 Tegeo 40-60mg orally twice daily on days 1-14 Repeat every 21 days |
|
>
Oxaliplatin + Fluorouracil-based
|
Oxaliplatin + |
Oxaliplatin 85mg/m2, IV, Day 1 |
|
Calcium folinic acid 400mg/m 2, IV, Day 1 |
|
|
Calcium folic acid |
5-Fluorouracil 400mg /m2, IV, Day 1 |
|
5-fluorouracil 2400-3600mg/(m2– d), continuous intravenous infusion for 48 hours |
|
|
when |
|
|
Repeat every 14 days |
|
|
XELOX |
Oxaliplatin 130mg/m2, IV, Day 1 Capecitabine 1000mg/m “font-size:6pt”>2, orally, twice daily, repeated every 21 days on days 1-14 |
|
SOX |
Oxaliplatin 130mg/m2< span style="font-size:12pt">, IV, Day 1 Tegeo 80mg/m2, orally, twice daily, repeated every 21 days from days 1 to 14 |
- style=”margin-left:12pt”> =”margin-left: 71pt”>
- Drug combination regimen
|
ECF |
Table Adriamycin 50mg/m2, IV, day 1 |
|
Cisplatin 60mg/m2, intravenously on day 1. IV, Day 1 |
|
|
5-Fluorouracil 200mg/(m2-d ) administered intravenously for 24 hours on the first |
|
|
1 to 21 days |
|
|
Repeat every 21 days |
|
|
EOX |
Table Adriamycin 50mg/m2, IV, day 1 |
|
Oxaliplatin 130mg/m2, IV, Day 1 |
|
|
Carbetabine 625 mg/m2, orally, twice daily, days 1-21 |
|
|
Repeat every 21 days |
|
|
DCF > |
Docetaxel 75mg/m2, IV, Day 1 |
|
Cisplatin 75mg/m2, IV, Day 1 |
|
|
5-Fluorouracil FU 1000mg/(m) 2-d), continuous intravenous for 24 hours, |
|
|
Day 1 to 5 |
|
|
< span style="font-family:imitation-song; font-size:12pt">Repeat every 28 days |
|
|
mDCF |
Docetaxel 60mg/m 2, IV, Day 1 |
|
Cisplatin 60mg/m2, intravenous, day 1 span> |
|
|
5-Fluorouracil 600mg/(m2-d), continuous IV for 24 hours, 1st to |
|
|
5 days |
|
|
Repeat every 14 days |
|
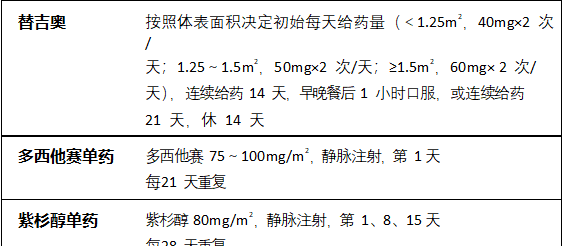 < span style="font-family:Microsoft elegant black; font-size:12pt">Single-drug regimen
< span style="font-family:Microsoft elegant black; font-size:12pt">Single-drug regimen
|
Paclitaxel 135-250mg/m2, intravenous, repeated every 21 days on day 1 |
|
Iritecan monotherapy< span style="font-family:imitation-song">Iritecan 150-180mg/m2, IV, repeat every 14 days on day 1 |
|
Iritecan 125mg/m2, IV, repeated every 21 days on days 1 and 8 |
Appendix XV: Commonly used targeted therapeutic agents for gastric cancer
|
< strong>Trastuzumab (+ chemotherapy)Load dose 8mg/kg (IV over 90 minutes); maintenance dose 6mg/kg (IV over 30-90 minutes) Repeat every 3 weeks If there is a delay or interruption in the course of treatment, a delay of ≤1 week may be made directly Maintenance dose; delay >1 week, reintroduce loading dose |
|
Apatinib mesylate 850mg orally once daily with lukewarm water half an hour after a meal, 28 days for 1 cycle If adverse reactions occur during dosing, maintain the dose level for NCI class 1 to 2; for NCI class 3 to 4, suspend the dose. ~If adverse reactions occur during dosing, NCI class 1 to 2, maintain the original dose level; NCI class 3 to 4, suspend dosing and wait until adverse reactions return to ≤1, then adjust the dose downward by 1 dose (1st dose adjustment to 750 mg once daily, 2nd dose adjustment to 500 mg once daily) and continue dosing. For physical status score ECOG ≥ 2, after fourth-line chemotherapy, primary cancer in the stomach For female patients with ECOG ≥2, after fourth-line chemotherapy, without resection, poor bone marrow reserve, old and frail, or thin, the starting dose can be reduced by starting with 500 mg once daily and taking |
|
Remolimumab (+ Paclitaxel < span style="font-family:仿宋">Remolimumab 8 mg/kg intravenously on day 1, repeated every 2 weeks ol)Remolimumab 8 mg/kg intravenously on days 1 and 15 + paclitaxel 80 mg/m2 IV on days 1, 8, 15, repeated every 4 weeks |
Appendix XVI: Basic criteria for determining the efficacy of radiation and chemotherapy for gastric cancer
I. Criteria for evaluating the efficacy of solid tumors
Complete remission, complete disappearance of tumor for more than 1 month.
Partial remission, where the product of the largest diameter of the tumor and the largest vertical diameter shrinks by up to 50 , with no increase in other lesions
, with no increase in other lesions
Large, lasting more than 1 month.
Stable lesion with a reduction in the product of the two diameters of the lesion of no more than 50 , increase by no more than 25
, increase by no more than 25 for more than 1 month.
for more than 1 month.
Progression of the lesion, with the product of the two diameters of the lesion increasing by more than 25 . II.RECIST1.1 Efficacy evaluation criteria
. II.RECIST1.1 Efficacy evaluation criteria
(i) Evaluation of target lesions
- style=”margin-left: 62pt”>
-
Complete remission: all target lesions disappeared, all pathological lymph nodes (including target nodes and non-target nodes)Partial remission: sum of target lesion diameters reduced by at least 30
 .
.
Progression of lesion: at least 20in diameter and relative increase from baseline level, using the minimum of the sum of all measured target lesion diameters as reference src=”https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0941_202277.png” alt=””/>(baseline values are used as reference if baseline measurements are minimal); otherwise, straight >
An absolute increase in the sum of the diameters of at least 5 mm (the presence of 1 or more new lesions is also considered disease progression).
Stable lesion: The target lesion has not decreased to the level of partial remission, nor has it increased to the level of lesion progression, but in between, the minimum value of the sum of the diameters can be used as a reference. The smallest value of the sum is used as a reference.(ii) Evaluation of non-target lesions
- style=”margin-left: 36pt”>
- Complete remission: disappearance of all non-target lesions and normalization of tumor markers.
Not in complete remission/stable: Presence of 1 or more non-target lesions and/or tumor markers persistently above normal values.- style=”margin-left: 36pt”>
- Progression of lesions. The presence of one or more new lesions and/or definite progression of an existing non-target lesion(s).
(iii) Evaluation of best overall outcome
The evaluation of best overall outcome is the smallest value measured between the start of treatment and disease progression or relapse. The classification of a patient’s best outcome usually consists of lesion measurement and confirmation.
Appendix XVII: Evaluation of Efficacy of Preoperative Adjuvant Therapy for Oncology (Tumor Regression Grading TRG)
Tumor regression grading (TRG)
as seen under the light microscope
0 (fully retracted)
None Tumor cell residual (including lymph nodes)
1 (medium receding)
Only single or small focal cancer cell remnants are seen
2 (slightly receding)
Tumor remnants but less than fibrotic interstitium
3 (no retraction)
extensive tumor remnants with no or little tumor cell necrosis
Remarks
- style=”margin-left: 112pt”>
- TGR score limited to primary tumor lesions
- Tumor cells refer to surviving tumor cells, excluding degenerated and necrotic cells
- The cell-free mucus lake that may appear after radiation/chemotherapy cannot be considered as tumor remnants.
Attachments
Gastric Cancer Guidelines (2022 Edition) Development and Validation Expert Group
(in order of last name stroke)
Team leader: Ji Jiafu
Members: Wang Renben, Shi Susheng, Liu Yunpeng, Liu Hongjun, Li Peng, Shen Lin, Wu Aiwen, Zhou Zhiwei, Zhou Aiping, Fang Xuedong, Zhao Dongbing.
Dao-Yu Hu, Quan Xu, Zhen Zhang, Jun Liang, Han Liang