Glioma Treatment Guidelines
(2022 Edition)
Gliomas are tumors that originate from glial cells in the brain and are the most common primary intracranial tumors. The 2021 edition of the WHO Classification of Tumors of the Central Nervous System classifies gliomas into grades 1 to 4, with grades 1 and 2 being low-grade gliomas and grades 3 and 4 being high-grade gliomas 1. This guideline focuses on the management of adult high- and low-grade gliomas of astrocytic, oligodendrocytic, and ventricular meningeal cell origin 2, 3.
The annual incidence of glioma in China is 5-8 per 100,000, and the 5-year mortality rate is second only to pancreatic cancer and lung cancer among systemic tumors. The pathogenesis of glioma is unknown, but two risk factors have been identified: exposure to high doses of ionizing radiation and genetic mutations with high epistasis associated with rare syndromes. In addition, carcinogenic factors such as nitrite foods and viral or bacterial infections may also be involved in the development of gliomas.
The clinical manifestations of glioma include increased intracranial pressure, neurological and cognitive deficits, and seizures. At present, clinical diagnosis mainly relies on CT and MRI, diffusion weighted imaging (DWI), diffusion tensor imaging (DTI), perfusion weighted imaging (PWI), magnetic resonance spectroscopy (MRI), and magnetic resonance imaging (MRI). PWI, magnetic resonance spectroscopy (MRS), functional magnetic resonance imaging (FMRI)
(functional magnetic resonance imaging, fMRI), ortho
electron emission tomography (PET) The use of positron emission tomography (PET) is important for the differential diagnosis of glioma and the evaluation of treatment effects.
Diagnosis of glioma requires histopathological and molecular pathological integration of the specimens obtained through tumor resection or biopsy to determine the pathological grade and molecular subtype. The histopathology and molecular pathology are integrated to determine the pathological grade and molecular subtype. Molecular markers are important for the individualized treatment and clinical prognosis of glioma. The treatment of glioma is based on surgical resection, combined with radiotherapy and chemotherapy. Surgery can relieve clinical symptoms, prolong survival, and obtain sufficient tumor specimens for definitive pathological diagnosis and molecular genetic testing. The principle of surgical treatment is to remove the tumor to the maximum extent safely, and new technologies such as conventional neuronavigation, functional neuronavigation, intraoperative neurophysiological monitoring and intraoperative MRI real-time imaging can help to achieve the maximum extent safely. Radiotherapy can kill or suppress tumor cells and prolong patient survival, and conventional fractionated external irradiation is the standard of care for glioma radiation therapy. Postoperative radiotherapy combined with temozolomide synchronized with adjuvant temozolomide chemotherapy for glioblastoma (GBM) has become the standard of care for newly diagnosed GBM in adults.
Treatment of glioblastoma requires a multidisciplinary approach including neurosurgery, neuroimaging, radiation therapy, neuro-oncology, pathology, and neurorehabilitation.
Treatment of glioma requires multidisciplinary collaboration between neurosurgery, neuroimaging
(multi-disciplinary team, MDT), following the principles of evidence-based medicine, individualized and comprehensive treatment, optimization and standardization of treatment protocols. In order to maximize the therapeutic benefit, maximize the progression-free survival time and overall survival time, and improve the quality of survival, the MDT aims to provide patients with the most optimal and comprehensive treatment. In order to achieve optimal comprehensive treatment, physicians need to follow patients closely and manage them throughout the entire process, with regular imaging reviews.
Physicians need to closely follow and manage patients throughout the course of their treatment, taking into account their daily life, social and family activities, nutritional support, pain management, rehabilitation and psychological management.
These are the most important issues in the world.
(A) Conventional imaging features of glioma.
Routine neuroimaging currently consists of CT and MRI, which provide relatively clear and precise views of brain anatomy and morphological features of brain tumor lesions. These two imaging methods can show the anatomical and morphological characteristics of brain tumors, such as location, size, peripheral edema status, tissue uniformity in the lesion area, occupancy effect, degree of blood-brain barrier disruption, and other combined signs caused by the lesion. MRI is superior to CT in terms of image information; CT mainly shows the density difference between glioma lesions and normal brain tissue, characteristic density features such as calcification, hemorrhage and cystic changes, the location of lesion involvement, edema status and occupancy effect, etc. Conventional MRI mainly shows the difference in signal intensity and occupancy effect of glioma hemorrhage, necrosis and edema tissue, and also shows the extent of lesion invasion. The conventional MRI mainly shows the difference in signal intensity and occupational effect of glioma hemorrhage, necrosis, edema, etc., and can show the extent of lesion invasion. Multimodal MRI can not only reflect the morphological characteristics of glioma, but also the functional and metabolic status of tumor tissue. Conventional MRI scans, which mainly acquire T1-weighted images, T2-weighted images, liquid
Fluid attenuated inversion recovery (FLAIR) sequence imaging and MR contrast enhancement scanning. The glioma is poorly defined and presents as a glioma. Gliomas are poorly defined and exhibit long T1 and T2 signal shadows, which can be heterogeneous, with varying degrees of peripheral edema. The magnitude of the surrounding edema varies. Enhancement scans vary depending on the degree of tumor damage to the blood-brain barrier. Gliomas can occur in all parts of the brain. The MRI of low-grade gliomas shows long T1 and T2 signals with unclear borders, mild peripheral edema, and mild localized occupying signs, which can be caused by adjacent ventricles.
Degree of compression, insignificant midline shift, largely normal brain pool, and few signs of hemorrhage, necrosis, and cystic degeneration in the lesion area. The enhancement scan shows that the lesion rarely shows mild abnormal enhancement. The MRI signal of high-grade glioma is clearly heterogeneous, with mixed T1 and T2 signals and peripheral finger-like edema; the occupancy signs are obvious, with the adjacent ventricles distorted by compression, the midline structures displaced, and the cerebral sulci and brain pools compressed; the enhancement scan shows obvious wreath-like and nodular abnormal enhancement.
The PET imaging characteristics of gliomas vary by grade. The widely used tracer is fluorine-18-fluorodeoxyglucose (18F- fluorodeoxyglucose,18F-FDG) and carbon-11 methionine (11C- methionine,11C-MET). The metabolic activity of low-grade gliomas is generally lower than that of normal gray matter, and that of high-grade gliomas can be close to or higher than that of normal gray matter, but the metabolic activity of 18F There is a large overlap in FDG metabolic activity (level 2 evidence)4. Amino acid tumor imaging has good lesion-background contrast and is better than 18F-FDG for grading gliomas, but there is still some overlap.
When a biopsy is proposed for a clinical diagnosis of suspected glioma, PET can be used to identify the areas of highest metabolic activity in the lesion. 18F-FET and 11C-MET has a higher signal-to-noise ratio and lesion contrast than 18F-FDG (level 2 evidence)F-FET has a higher signal-to-noise ratio and lesion contrast than C-MET. span style=”font-size:8pt”>5.PET combined with MRI is more accurate than MRI alone in defining the target area for radiotherapy (level 1 evidence)6. >6. Compared to conventional MRI techniques, amino acid PET can improve the accuracy of outlining tumor biologic volume, detecting potentially tumor cell-infiltrated/invaded brain tissue (which can be found without abnormalities on conventional MRI images), and incorporating it into the patient’s radiotherapy target area (level 2 evidence)7, 8. /span>. 18F-FDG PET due to tumor/cortex
Low contrast and therefore not suitable for adjuvant targeting of radiotherapy (level 2 evidence)9. Neurosurgery clinicians have clear requirements for neuroimaging diagnosis: first
First, localization is required to determine the size and extent of the tumor, its proximity to important surrounding structures (including important arteries, cortical veins, cortical functional areas, and nerve fiber bundles), and morphological features. This is important for the formulation of the surgical plan for glioma; secondly, the diagnostic requirements of the functional status of neuroimaging, such as tumor growth and metabolism, blood supply status and the degree of tumor invasion to the surrounding brain tissues, which is crucial for the comprehensive postoperative efficacy assessment of patients. In addition to conventional MRI sequences such as basal T1, T2, and enhanced T1, multimodal MRI sequences such as DWI, PWI, and MRS can reflect not only the morphological characteristics of glioma, but also the functional and metabolic status of tumor tissues. The elevated choline (Cho) and Cho/N-acetyl-aspartate (NAA) ratios in MRS are positively correlated with tumor grade. fMRI sequences such as DTI and blood oxygenation level dependent (BOLD) can clarify the relationship between tumor and important functional cortical and metabolic areas. The relationship between the tumor and important functional cortical and subcortical structures can provide evidence to support the protection of brain function during surgical resection. Multimodal MRI is important for differential diagnosis of glioma, determination of surgical boundaries, prognosis, monitoring of treatment outcome, and clarification of the presence or absence of recurrence, and is an important complement to morphological imaging diagnosis.
 Table 1 Diagnostic imaging points for glioma
Table 1 Diagnostic imaging points for glioma
Tumor type Characteristic imaging presentation


Low-grade glioma Mainly diffuse astrocytic glioma
3 types of glioma: oligodendroglioma, oligodendroglioma, and oligodendroglioma. Special types also include PXA, third ventricular chordoma-like glioma, and hairy cell astrocytoma.
The MRI signal of diffuse astrocytoma is relatively homogeneous, with long T1, long T2, and FLAIR high signal, mostly without enhancement; oligodendroglioma shows the same pattern as diffuse astrocytoma. PXA is mostly found in the temporal lobe, with superficial location, cystic lesions and wall nodules. Enhanced scans show enhancement of the wall nodules and adjacent meninges. Chordoma-like glioma of the third ventricle is located in the third ventricle. The hairy cell astrocytoma is predominantly solid and commonly found in the suprasellar and cerebellar hemispheres.
Mesenchymal glioma (grade 3)
Majorly including mesenchymal astrocytoma and mesenchymal oligodendroglioma.
When MRI/CT appears to resemble astrocytoma or oligodendroglioma with enhancement, it suggests a high likelihood of mesenchymal glioma.
Grade 4 glioma Glioblastoma tumor; diffuse midline glioma.
Ventricular meningeal tumors Mainly grade 2 and 3 ventricular meningeal tumors. Special types: mucinous papillary ventricular meningioma is grade 1.
Glioblastoma is characterized by irregularly shaped peripheral enhancement and massive central necrosis, with edema visible outside the enhancement. Diffuse midline gliomas often occur in midline structures such as the thalamus and brainstem, and MRI shows long T1 and long T2 signals, with varying degrees of enhancement on enhancement scans.
Ventricular canal tumors are well-defined, mostly located in the ventricles, with mixed signals, and hemorrhage, necrosis, cystic changes, and calcifications can coexist, and tumor enhancement is often evident. Mucinous papillary ventricular tumors are more likely to be found in the spinal cone and cauda equina.


Note:PXA, pleomorphic yellow neoplastic astrocytoma;FLAIR, liquid inhibition inversion recovery sequence.
(B) Differential diagnosis of glioma.
- style=”margin-left: 65pt”>
- Metastatic lesions in the brain
Multiple metastatic lesions are more common in the brain, mostly located in the subcortex, varying in size and degree of edema, with a variety of presentations, most of which are ring-like or node-like enhancing. The 18F-FDG metabolic activity in metastatic lesions in the brain can be lower, nearer, or higher than that in the gray matter; amino acid metabolic activity is generally higher than that in the gray matter. Single metastatic carcinoma needs to be differentiated from high-grade glioma. Imaging can be based on lesion size, lesion involvement, and enhancement performance, combined with medical history, age, and
Related other adjuvant findings can be combined to differentiate. 2. Infectious lesions in the brain
Infectious lesions in the brain, especially brain abscesses, need to be differentiated from high-grade gliomas. Both have edema and occupying signs, and the enhancement is circumferential. Brain abscesses often have smooth walls and no wall nodules, whereas high-grade gliomas tend to have cauliflower-like enhancement with mixed intracapsular signal and may be associated with tumor stroke. The vast majority of high-grade gliomas have significantly higher amino acid metabolic activity than normal brain tissue, whereas brain abscesses are generally hypometabolic.
- style=”margin-left: 65pt”>
- Demyelinating lesions in the brain
A tumor-like demyelinating lesion, which is easily confused with glioma, is seen as a nodular enhancing shadow on enhancement scan and is easily recurring when reviewed after diagnostic treatment. Laboratory tests can help in the differential diagnosis.
- style=”margin-left: 65pt”>
- Lymphoma
In immunocompetent patients, the MRI signal of lymphoma is more homogeneous, intra-tumoral hemorrhage and necrosis are rare, and enhancement is markedly homogeneous. 18F-FDG metabolic activity is generally higher and more uniformly distributed than in high-grade gliomas.
- style=”margin-left: 65pt”>
- Other tumors of neuroepithelial origin
Including central neuroblastoma. The initial differential diagnosis can be made based on the location of the tumor and its enhancement.
(C) Imaging grading of glioma.
- style=”margin-left: 65pt”>
- Conventional MRI examination
With the exception of some grade 2 gliomas (e.g., pleomorphic yellow astrocytoma, third ventricular chordoma-like glioma, and ventricular meningioma), high-grade gliomas
MRI of high-grade gliomas is often enhanced with stroke, necrosis, and cystic changes. The MRI is a very important tool in the development of a patient’s health.
- style=”margin-left: 65pt”>
-
Multimodal MRI examination
Including DWI, PWI and MRS, etc. High signal areas in DWI suggest high cell density and represent high-grade lesions; high perfusion areas in PWI suggest increased blood volume and are mostly high-grade lesions; elevated Cho and The Cho/NAA ratio is elevated, which correlates positively with tumor grade.
- style=”margin-left: 65pt”>
- PET
The tumor-background contrast of metabolic imaging of glioma is low, whereas amino acid tumor imaging has better tissue contrast, therefore, amino acid PET brain imaging is recommended to evaluate Glioma grade (level 2 evidence)10. 11C-MET PET assessment is more accurate than MRI for high-grade glioma 11C-MET metabolic activity is generally higher than that of low-grade gliomas, but there is still some overlap between high-grade and low-grade gliomas (level 2 evidence)11-13 >. The use of 18F-FDG PET dynamic imaging analysis is recommended to improve the imaging grading of gliomas when necessary.
(D) Post-treatment imaging assessment of glioma.
MRI (plain+enhanced) should be reviewed within 24-72 hours after glioma surgery to assess the extent of tumor resection and to use this as a baseline imaging assessment of the brain. This is used as the baseline imaging data for follow-up comparison after glioma surgery. The imaging evaluation of glioma outcome is based on the RANO criteria (Table 2)14.
 Table 2 Glioma treatment outcome assessment RANO criteria
Table 2 Glioma treatment outcome assessment RANO criteria
Complete remission partial remission stable disease disease progression T1 enhancement no shrinkage ≥50  Change in -50 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_20228.png" alt=""/>~+25
Change in -50 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_20228.png" alt=""/>~+25  increase of ≥25
increase of ≥25  T2-FLAIR stable or decreasing stable or decreasing stable or decreasing increasing new lesions no no no no hormone use no stable or decreasing stable or decreasing not applicable* clinical symptoms stable or improving stable or improving stable or improving worsening needed Meet all of the above conditions Any of the above conditions Note: *Disease progression is considered when there is persistent worsening of clinical symptoms, but increased hormone dosage should not be used solely as a basis for disease progression.
T2-FLAIR stable or decreasing stable or decreasing stable or decreasing increasing new lesions no no no no hormone use no stable or decreasing stable or decreasing not applicable* clinical symptoms stable or improving stable or improving stable or improving worsening needed Meet all of the above conditions Any of the above conditions Note: *Disease progression is considered when there is persistent worsening of clinical symptoms, but increased hormone dosage should not be used solely as a basis for disease progression.
Gliomas include in situ recurrence, distant recurrence and spinal cord dissemination according to the site of recurrence and other specific modalities, with in situ recurrence being the most common.15 Histopathological diagnosis remains the gold standard. Pseudoprogression is most often seen within 3 months after radiation/chemotherapy and in a small number of patients within 10 to 18 months. It often presents with circumferential enhancement around the lesion, marked edema, and signs of occupancy, and needs to be judged with clinical caution. For high-grade gliomas, amino acid PET is useful for identifying treatment-related changes
(pseudoprogression, radionecrosis) and tumor recurrence/progression with a high degree of accuracy
(Radiation necrosis is most often seen after 3 months of radiotherapy, and there is no specific test to identify radiation necrosis from tumor progression/recurrence. In high-grade gliomas, 18F-FDG PET is less advantageous than MRI for evaluating postoperative tumor recurrence and radionecrosis, while amino acid PET has higher sensitivity and specificity for identifying tumor progression and treatment-related responses. For low-grade gliomas, 18F-FDGPET is not suitable for evaluating tumor response to therapy, and the evaluation of amino acid PET is limited (level 1 evidence).18 Regular MRI or PET can help identify pseudoprogression.
Regular MRI or PET examinations can help to identify pseudoprogression and tumor progression/recurrence (Table 3). Multimodal MRI examinations such as PWI and MRS are also informative. Table 3 Identification of glioma recurrence, pseudoprogression, and radiation necrosis
Table 3 Identification of glioma recurrence, pseudoprogression, and radiation necrosis
Item tumor recurrence pseudoprogression radionecrosis occurred at any time mostly seen after radiation/chemotherapy 3 months to years after treatment within months, a few patients seen within 10 months clinical symptoms worsened unchanged or worsened unchanged or worsened MRI enhancement scan multiple lesions and corpus callosum subject to large swaths of long T1 and T2 letters MRI enhancement scan visible invasion usually recurrence number, within the irregular reinforcement, late manifestation of reinforcement. Occupancy effect clearly high signal apparent PWI usually Kor perfusion usually low perfusion usually low perfusion MRSCho/NAA , Cho/CrCho/NAA , Cho/CrCho/NAA , Cho/CrCho/NAA , Cho/Cr higher lower lower DWI diffusion restricted than tumor signal lower than tumor signal lower glucose PET usually high metabolism high metabolism or low metabolism low metabolism amino acid PET
18F-FDGPET and high metabolism low metabolism low metabolism good incidence factor radiation therapy + temozolium radiation therapy amine in relation to radiotherapy can be in the radiation therapy field Fan more in the radiation therapy field Fan more in the radiation therapy field range periphery within the periphery incidence almost all total 20 ~30
~30 , in the same dose-related, common in about step radiotherapy, in 2
, in the same dose-related, common in about step radiotherapy, in 2 to 18
to 18  especially for MGMT promoter region methylation occurs at a higher rate in those
especially for MGMT promoter region methylation occurs at a higher rate in those
III.
(a) WHO classification criteria for central nervous system tumors, 2021 edition.
Glioma is a general term for a group of neuroepithelial tumors with a glial cell phenotype. The genetic background and developmental mechanisms of glioma are becoming clearer with the development of pathology and advances in pathology detection techniques, especially second-generation sequencing, DNA methylation profiling and other histological techniques. A growing number of molecular markers have been shown to play an important role in the classification, staging, grading, prognosis, and treatment of gliomas.19-22 The 5th edition of the WHO Classification of Tumors of the Central Nervous System, published in 2021, integrates histologic features and molecular phenotypes of tumors and proposes new tumor classification criteria, focusing on the application of molecular diagnosis in the classification of central nervous system tumors. This classification is now an important basis for the diagnosis and classification of gliomas (Table 4). Table 4 WHO Classification of Gliomas of the Central Nervous System, Version 2021
Table 4 WHO Classification of Gliomas of the Central Nervous System, Version 2021
Adult diffuse glioma Astrocytoma, IDH mutant
Astrocytoma, IDH mutant
oligodendroglioma, IDH mutation with 1p/19q combination deletion glioblastoma, IDH wild type

 Childhood type diffuse low-grade glioma
Childhood type diffuse low-grade glioma
diffuse astrocytoma, MYB or MYBL1 variant
Angiocentric glioma
juvenile pleomorphic low-grade neuroepithelial tumor
 Diffuse low-grade glioma, MAPK signaling pathway variant diffuse high-grade glioma of childhood type
Diffuse low-grade glioma, MAPK signaling pathway variant diffuse high-grade glioma of childhood type
Diffuse midline glioma, H3 K27 variant
Diffuse hemispheric glioma, H3 G34 mutant
Diffuse pediatric high-grade glioma, H3 wild and IDH wild-type infantile hemispheric glioma

 Restricted astrocytic glioma
Restricted astrocytic glioma
hairy cell astrocytoma
high-grade astrocytoma with hairy cell-like features pleomorphic yellow astrocytoma
subventricular giant cell astrocytoma chordoid glioma
 Astroblastoma with MN1 altered ventricular meningeal tumor
Astroblastoma with MN1 altered ventricular meningeal tumor
Supratentorial ventricular meningioma
Supratentorial ventricular meningioma, ZFTA fusion-positive supratentorial ventricular meningioma, YAP1 fusion-positive posterior cranial fossa ventricular meningioma
Posterior cranial fossa ventricular meningioma, posterior cranial fossa ventricular meningioma in PFA group, spinal ventricular meningioma in PFB group
Spinal ventricular meningioma, MYCN-amplified mucinous papillary ventricular meningioma
subventricular ventricular tumor

(B) Classification of gliomas and their molecular variants.
Tumor classification and molecular phenotype
The 5th edition of the WHO Classification of Tumors of the Central Nervous System classifies gliomas into 5 groups based on histologic and molecular pathologic features (Table 5): ①Adult type (1) adult-type diffuse gliomas; (2) pediatric-type diffuse low-grade gliomas; (3) pediatric-type diffuse high-grade gliomas; (4) limited astrogliomas; and (5) ventricular meningeal tumors.
 Table 5 Recommended molecular pathology tests for glioma
Table 5 Recommended molecular pathology tests for glioma
Markers Genetic variants Detection method Diagnostic value Prognostic significance
 IDH1 Mutation
IDH1 Mutation
(R132H/C/L/S/G)
IDH2 mutation
(R172K/M/G/W)
Immunohistochemistry, Sanger
Sequencing, pyrophosphate sequencing, diphase sequencing
Sanger sequencing, pyrophosphate sequencing, diphase sequencing
Key molecular variants for glioma classification; identifiable
Differentiate WHO grade I glioma from gliosis.
Indicates a relatively good prognosis; often used in clinical trials as
important grouping indicator; closely associated with MGMT promoter methylation; relatively sensitive to radiotherapy and alkylating agents; potential therapeutic target (e.g. Ivosidenib).
Dye body 1p/19q
Co-Deficiency FISH , PCR , Meth
Chemical Microarrays/ Expression Profiling Microarrays/ Second Generation Sequencing Related Methods
Key variants in oligodendroglioma. Suggests relatively good prognosis; for radiotherapy and alkylating agents ph
Sensitive to radiotherapy and alkylating agents.
H3 K27 mutation
Immunohistochemistry, Sanger diagnosis of diffuse midline glioma with H3K27 mutation
Relatively poor prognosis; could be a potential therapeutic target (ex.
(K27M)
Sequencing, second generation sequencing
Key reference indicators for variant.
e.g. EZH2 inhibitor).
H3 G34 mutation
(G34R/V)
Immunohistochemistry, Sanger diffuse midline glioma, H3K27 mutation sequencing, second generation sequencing type.
Survival is slightly longer than IDH mutant glioblastoma, but shorter than IDH mutant WHO grade 4 glioma.
ATRX mutation Immunohistochemistry Sanger sequencing, second generation sequencing
TP53 mutation immunohistochemical Sanger sequencing, second-generation sequencing
ATRX nuclear expression deletion and/or positive for p53 mutation can be diagnosed as IDH mutant astrocytoma without detecting 1p19q. ATRX nuclear expression deletion and/or positive p53 mutation can be diagnosed as IDH mutant astrocytoma without detection of 1p19q.
ATRX nuclear expression deletion and/or p53 mutation positive, diagnostic of IDH mutant astrocytoma without detection of 1p19q. ATRX nuclear expression deletion and/or positive p53 mutation can diagnose IDH mutant astrocytoma without detecting 1p19q. It can be used to differentiate diffuse or non-diffuse WHO grade 1 gliomas from gliosis.
The prognosis is better than for IDH-mutant glioblastoma.
|
CDKN2A/B |
purity deletion |
FISH , qPCR , |
Histology Lack of necrosis and microvascular proliferation in stars |
Poor prognosis in IDH mutant gliomas. |
||||||
|
MLPA, methylation chip |
Morphocytoma, IDH mutation, WHO grade 4 Glial |
|||||||||
|
/expression profiling microarray/II |
Diagnostic indicators for tumors One of them. |
|||||||||
|
Sequencing-related methods |
||||||||||
|
TERT |
Promoter mutations |
Sanger sequencing, pyrophosphorus |
Sanger sequencing, pyrophosphorus |
in oligodendroglioma and glioblastoma |
< span style="font-family:Arial; font-size:12pt">Poor prognosis in IDH wild-type gliomas; poor prognosis in IDH |
|||||
|
(C228T/C250T) |
Acid sequencing, second generation sequencing |
is common; in the absence of histological necrosis and microhematology |
Prognosis is better in mutant gliomas. |
|||||||
|
in the case of canal hyperplasia, it is glioblast |
||||||||||
|
tumor, IDH wild type, WHO grade 4 diagnostic indication |
||||||||||
|
one of the criteria. |
||||||||||
|
Dye Body |
+7/-10 |
FISH, second-generation sequencing, |
in the absence of histological necrosis and microvascular proliferation |
Poor prognosis in IDH wild-type gliomas. |
||||||
|
7/10 |
Microarray Chip |
case is glioblastoma, IDH wild |
||||||||
|
Birth type, one of the diagnostic indicators of WHO class 4. |
||||||||||
|
EGFR |
Amplification |
FISH , digital PCR , |
Amplification |
Astrocytoma, IDH mutant, WHO grade 4 |
||||||
|
Astrocytoma, IDH mutant, WHO grade 4 |
||||||||||
| Dio-sequencing, microarray |
One of the diagnostic indicators of glioma; glioblastoma |
|||||||||
|
Chip |
Cytoma, IDH wild type, WHO grade 4 glioma |
|||||||||
|
one of the diagnostic indicators. |
||||||||||
|
EGFRvIII rearrangement |
RT-PCR, digital |
EGFRvIII occurs in about half of the EGFR amplifications |
potential targets for targeted therapies. |
|||||||
|
PCR , immunohistochemistry |
in glioblastoma. |
|||||||||
|
MLPA, second-generation sequencing |
||||||||||
|
BRAF |
Mutation |
Immunohistochemistry Sanger |
appears in a variety of gliomas, including the epidermal type |
targets for targeted therapies (e.g., vemurafenib). |
||||||
|
(BRAFV600E) |
Sequencing, pyrophosphorylation | Sequencing, pyrophosphorylation | Sequencing, pyrophosphorylation span> |
Glioblastoma. |
||||||
|
sequencing, second-generation sequencing |
||||||||||
|
MGMT |
Promoter Region Methylation |
Methylated Specificity |
||||||||
| Methylated Specificity
Better prognosis in glioblastoma; temozolomide treatment |
||||||||||
|
PCR , pyrophosphate measurement |
sequential, methylation microarrays |
Related. |
||||||||
|
FGFR |
Fused genes |
Sanger sequencing, |
In astrocytoma, IDH wild type, WHO 4 |
Can be a potential target for targeted therapies (e.g. FGFR inhibition |
|
MET |
(FGFR-TACC)
Fusion Gene |
qPCR, second generation sequencing
Sanger sequencing, |
grade and glioblastoma, IDH wild type. Occurrence in WHO grade 4. In astrocytoma, IDH wild type, WHO grade 4 |
agent).
In secondary glioblastoma (astrocytoma, |
|||
|
miR-181d |
(PTPRZ1-MET) Mutation (METex14) High Expression |
qPCR, second generation sequencing
microRNA expression profile core |
grade and glioblastoma, IDH wild type, present in WHO grade 4. |
The prognosis is poor in IDH mutant, WHO grade 4); it can be used as a therapeutic target (e.g. MET inhibitor).
Higher expression in glioblastoma in response to temozol |
|||
|
TSC1/2 |
Mutation |
slice, qPCR, in situ hybridization staining Sanger sequencing, NGS |
Diagnosis of subventricular giant cell astrocytoma |
amine chemotherapy is more effective.
mTOR signaling pathway inhibitor (e.g. everolimus) therapy |
|||
|
Specific markers. |
Target. |
||||||
|
ZFTA |
Gene Fusion |
FISH, NGS |
Diagnosis C11orf95 fusion-positive supratentorial ventricular canal |
The prognosis for patients with supratentorial ventricular meningioma who develop this fusion is relatively |
|||
|
YAP1 |
(C11orf95- RELA) Gene Fusion |
Membrane specific markers.
Diagnosis of YAP1 fusion-positive supratentorial ventricular membranes |
poorly.
Patients with supratentorial ventricular meningioma who develop this fusion have a relatively |
||||
|
(YAP1-MAMLD1)< |
Specific markers. |
Better. |
|||||
|
MYCN |
amplification |
FISH, NGS |
Diagnosis of MYCN amplified spinal ventricular tract specific |
The prognosis of patients with this amplification |
|||
|
sexual markers. |
Poor. |
||||||
|
NF1 |
mutation |
Sanger sequencing, NGS |
in optic pathway gliomas and IDH wild-type gliomas |
The prognosis of hairy cell astrocytomas carrying this mutation is comparable |
|||
|
Mutation frequency is higher in cytomas. |
To Better. |
Note:FISH, fluorescence in situ hybridization;PCR, polymerase chain reaction technology;qPCR, quantitative polymerase chain reaction technology;< span style="font-family:Times New Roman">MLPA, multiplex ligation-dependent probe amplification technology.
-
Adult-type diffuse glioma and pediatric-type diffuse glioma. For the first time, the new classification divides diffuse gliomas into two categories: adult-type and pediatric-type diffuse gliomas. It is important to note that this diagnostic classification is not based solely on the age of onset of the tumor, but rather on clinical features such as the major molecular variants and the age-specific distribution of these tumors. Adult-type diffuse gliomas are the main type of adult glioma, but can occur in children, while pediatric-type diffuse gliomas occur primarily in children, but can also occur in adults, especially young adults.
Isocitrate dehydrogenase (IDH) mutations are an important diagnostic marker for adult-type diffuse glioma. The IDH mutation in diffuse gliomas with short arm of chromosome 1/long arm of chromosome 19
(1p/19q) combination deletion is diagnosed as “oligodendroglioma, IDH mutation and 1p/19q combination deletion type”; diffuse glioma without 1p/19q combination deletion but with ATRX mutation is diagnosed as “astrocytoma, IDH The CDKN2A/B pure deletion is a graded marker for this type of tumor. Diffuse gliomas that are IDH wild and histone H3 wild are diagnosed as “glioblastoma, IDH wild” if they show necrosis or microvascular proliferation, or if they have one of three molecular variants: EGFR amplification, chromosome 7 amplification/chromosome 10 deletion (+7/-10), or mutations in the TERT promoter region.
Childhood diffuse low-grade gliomas are characterized by MYB/MYBL1 variants and mitogen-activated protein kinase (MAPK) signaling pathway variants. Among them, MYB/MYBL1 gene copy number variants and gene fusions are important molecular markers for the diagnosis of “diffuse astrocytoma, MYB or MYBL1 variant” and “angiocentric glioma”; MAPK signaling pathway-related gene variants are important molecular markers for the diagnosis of “diffuse astrocytoma, MYB or MYBL1 variant” and “angiocentric glioma”.
including BRAF, FGFR1, etc., are important diagnostic criteria for “juvenile pleomorphic low-grade neuroepithelial tumors” and “diffuse low-grade glioma, MAPK pathway variant”. Diffuse high-grade gliomas in children are characterized by histone H3 mutations, including “diffuse midline glioma, H3 K27 variant”, which occurs in the midline and has a deletion of H3 K27me3 nuclear expression, and “diffuse hemispheric glioma, H3 G34 mutant”, which occurs in the hemisphere and has H3G34R/V mutations. For diffuse gliomas that lack IDH mutations and H3 variants, often occur in infants, children, and young adults, and have high-grade histologic features, the diagnosis is “diffuse childhood high-grade glioma, H3 wild and IDH wild” or “infantile hemispheric glioma” based on their molecular variants and methylation characteristics.
-
Limited astrocytic glioma: The new classification includes hairy cell astrocytoma, hairy cell-like astrocytoma, hairy cell glioma, and hairy cell glioma. The new classification classifies six types of gliomas, including hairy cell astrocytoma, high-grade astrocytoma with hairy cell-like features, pleomorphic yellow astrocytoma, subventricular giant cell astrocytoma, chordoid glioma, and astroblastoma, MN1 variant, as limited astrocytic glioma. The term “limited” refers to their relatively controlled growth pattern, as opposed to “diffuse” tumors, meaning that these gliomas have a more limited growth pattern and are more clearly defined on imaging, but do not represent low grade, and some tumors may be invasive or even disseminated23< span style="font-size:16pt">. Most of these tumors have typical histologic features, such as astrocytic pseudogerminous clusters, biphasic structures and hair-like cells in hairy cell astrocytomas, as well as characteristic molecular variants, such as KIAA1549: BRAF fusion, BRAF V600E mutation, TSC1/TSC2 mutation, and PRKCA D463H mutation.
High-grade astrocytomas with hairy cell-like features are a new class of tumors defined in the WHO CNS5, and the diagnosis of these tumors is dependent on DNA methylation profiles; tumors with a typical astroblastoma morphology that carry the MN1 variant can be diagnosed as “astroblast, MN1 variant.
-
Ventricular vascular tumors: The molecular features of ventricular vascular tumors are closely related to their anatomic location, age, and other factors. Episodic ventricular meningiomas are mainly characterized by fusion genes and can be divided into ZFTA fusion-positive and YAP1 fusion-positive types. The proportion of non-ZFTA non-YAP1 fusion supratentorial ventricular meningiomas is low. Ventricular meningiomas in the posterior cranial fossa exhibit characteristic DNA methylation profile changes and can be divided into PFA and PFB groups; PFA group ventricular meningiomas mainly occur in infants and children, most of them have mesenchymal features and poor prognosis, with deletion of histone H3K27me3 expression, EZHIP overexpression and stable genome; PFB group ventricular meningiomas mainly occur in older children or adults, with relatively good prognosis. H3K27me3 expression was normal. One group of spinal ventricular meningiomas is characterized by MYCN gene amplification, which is highly aggressive and metastatic, and has a poor prognosis.
The new classification is no longer graded across tumor entities, but by tumor type, further emphasizing the biological similarity within tumor types. For example, an IDH mutant astrocytoma with a pure CDKN2A/B deletion will be diagnosed as CNSWHO grade 4 even if there are no high-grade histologic features such as microvascular proliferation or necrosis. It is important to note that the new grading system still retains the
with CNS features and therefore recommends the use of the term “CNSWHO grade” in grading. The term “CNSWHO level” is recommended for grading.
The use of NOS and NEC effectively identifies unclear tumor diagnoses that (1) lack the necessary molecular information or (2) cannot be effectively classified by molecular testing or have negative results. NOS indicates the inability to establish an integrated diagnosis at the histomorphologic and molecular levels, and thus the failure of molecular testing that has not yet been performed by the clinician or for technical reasons. On the other hand, NEC indicates that the necessary diagnostic tests were successfully performed, but the WHO integrated diagnosis could not be made given the mismatch between clinical, histologic, immunohistochemical, and/or genetic features. As with the WHO diagnosis, the NEC and NOS diagnoses should be reported by stratified integration.
Glioma pathology report should be standardized, standardized, and integrated and stratified diagnosis according to the new version of classification. The content should include: (1) integrated diagnosis; (2) histopathological classification; (3) CNSWHO grade; and (4) molecular information, which should indicate details such as specimen type, detection method, and variant type. The pathology report should also include basic clinical information about the patient, tumor site, and notes on special circumstances.
The principle of surgical treatment of gliomas is to maximize safe resection, with the basic goals of relieving occupying The basic objectives include: relieving the signs of occupancy and relieving the symptoms of intracranial hypertension; relieving or alleviating the symptoms associated with glioma, such as secondary epilepsy; obtaining pathologic histology and molecular pathology to clarify the diagnosis; and reducing the tumor load to provide for subsequent comprehensive treatment.
Surgical treatment of glioma can be divided into tumor resection and pathological biopsy.
- style=”margin-left: 78pt”>
- Indications and contraindications for tumor resection.
①Indications: CT or MRI suggesting intracranial occupancy; presence of obvious signs of intracranial hypertension and brain herniation; presence of neurological deficits due to tumor occupancy; clear history of seizures; patient voluntarily undergoes surgery.
②Contraindications: patients with severe cardiac, pulmonary, hepatic, renal dysfunction and recurrence, poor general condition that cannot tolerate surgery; other contraindications that are not suitable for neurosurgical craniotomy.
- style=”margin-left: 78pt”>
- Indications and contraindications for pathologic biopsy.
Indications: Tumor located in the dominant hemisphere, extensive infiltrative growth or invasion of bilateral hemispheres; tumor located in functional cortical, deep white matter or brainstem areas that cannot be satisfactorily resected; need to identify the nature of the lesion.
There are contraindications: severe cardiac, pulmonary, hepatic, and renal dysfunction and recurrence, poor general condition that cannot tolerate surgery, and other contraindications that make the patient unsuitable for neurosurgery.
- Pathologic biopsy procedure: Biopsies can be divided into two categories: stereotactic or guided biopsies and open surgical biopsies. Stereotactic or guided biopsies are suitable for
for lesions that are more deeply located; whereas open biopsy is indicated for lesions that are superficially located or close to the functional cortex. The lesions are more superficial or close to the functional cortex. Cranial biopsy can obtain more tumor tissue than stereotactic biopsy, which is beneficial for the determination of results. The diagnostic accuracy of biopsy is higher than that of imaging, but there is still a misdiagnosis rate due to the heterogeneity of the tumor and target selection.
- style=”margin-left: 78pt”>
- Perioperative management.
Preoperative management: If there are obvious symptoms of intracranial hypertension before surgery, dehydrating drugs should be given to relieve intracranial hypertension; if there is obvious hydrocephalus, ventriculoperitoneal shunt or ventriculostomy can be considered first. If there is significant hydrocephalus, ventriculoperitoneal shunts or ventriculoperitoneal external drainage may be considered.
Post-operative management: dehydration medication should be used to lower the cranial pressure according to the intracranial pressure, and hormones should be used to stabilize the patient. The patient’s neurological status should be stabilized with appropriate hormones. If postoperative fever occurs, lumbar puncture should be performed in a timely manner to collect cerebrospinal fluid for laboratory examination and actively prevent intracranial infection.
-
Use of new surgical adjuncts: The use of new surgical adjuncts helps to determine the extent of surgical resection and tumor boundaries as well as the intraoperative period. The use of new surgical adjuncts helps to determine the extent of surgical resection and tumor borders and to preserve intraoperative function.
Recommendations: neuroimaging navigation, functional neuroimaging navigation (level 2 and 3 evidence) 23, intraoperative neurophysiological monitoring techniques (e.g., functional cortical localization and subcortical nerve conduction bundle localization) (level 3 evidence)24 =”font-size:16pt”>and intraoperative MRI real-time image neuronavigation (level 3 evidence)25. Multimodal neuronavigation combined with intraoperative cortical and subcortical localization can further improve surgical safety and protect neurological function,.
Benefits Maximum range of safe resection (level 3 evidence)26.
Recommendable: fluorescence-guided microsurgery (level 2 evidence)27 and intraoperative ultrasound imaging for real-time localization.
-
Determination of the extent of surgical resection of glioma: review within 24-72 hours after glioma surgery is highly recommended MRI is recommended for high-grade gliomas and T2-FLAIR for low-grade gliomas, and this image is used as a baseline for determining the efficacy of subsequent treatment or tumor progression. The extent of resection is thus classified into 4 levels according to the volume of the resected tumor: total resection, subtotal resection, partial resection, and biopsy, and the specific criteria are not yet uniform.
- style=”margin-left: 48pt”>
- High-grade glioma
Highly recommended for maximum safe resection (level 2 and 3 evidence)28, 29. The goals of surgery include: alleviating symptoms caused by high cranial pressure and compression; reducing steroid drug use and maintaining better survival; reducing tumor cell load and creating conditions for adjuvant radiotherapy/chemotherapy; prolonging survival; and obtaining an accurate pathologic diagnosis. Removing as much of the tumor as possible is an important factor in the prognosis of patients with high-grade glioma compared with biopsy alone30. However, due to the infiltrative nature of high-grade gliomas, it is often difficult to achieve complete pathological resection of the tumor. The use of novel surgical adjuvant techniques can help maximize the extent of safe resection of high-grade gliomas. The extent of tumor resection is an independent prognostic factor for high-grade glioma, and complete tumor resection prolongs postoperative tumor recurrence and patient survival (level 2 and 3 evidence)28, 29, 31. .
- style=”margin-left: 48pt”>
- Low-grade glioma
Low-grade gliomas account for approximately 30 percent of gliomas
 , and the age of onset of patients
, and the age of onset of patients - High-grade glioma
Younger than high-grade gliomas, often located in or near important functional areas such as motor, language, visual-spatial, and memory The tumors are often located in or near important functional areas such as motor, language, visual space, and memory. For diffuse low-grade gliomas, maximum safe resection of the tumor is strongly recommended (level 2 and 3 evidence)32. Novel surgical adjunct techniques can effectively improve the rate of complete tumor resection on patient imaging and reduce the incidence of permanent postoperative neurological deficits (level 2 and 3 evidence)24, 25. Arousal surgery techniques have expanded the indications for surgery in functional areas of the brain (see the section on “Surgical Treatment of Gliomas in Functional Areas” for more details). For low-grade gliomas in nonfunctional or adjacent functional areas, functional localization techniques can identify cortical and subcortical structures associated with critical brain functions, allowing surgical resection to extend to the critical functional structures at the border of the brain to achieve maximum safe resection of low-grade gliomas33. span>.
- style=”margin-left: 54pt”>
- Recurrent glioma
At present, there is a lack of high-level evidence-based evidence for the benefit of surgical treatment of recurrent gliomas. The principle of surgery is to maximize safe resection. The goals of surgery include obtaining histologic and biological information, determining whether the tumor is recurrent or pseudoprogressive, reducing tumor load, relieving symptoms, and allowing for additional postoperative treatment34. Novel surgical adjunct techniques help to achieve maximum safe resection of recurrent gliomas. The surgical treatment of recurrent glioma must be individualized, taking into account the patient’s age, clinical functional status, histologic type, response to initial treatment, type of recurrence (local or diffuse), time interval between first surgery and reoperation, and previous treatment modalities35. span style=”font-size:16pt”>.
Functional-zone glioma is a tumor involving the brain according to preoperative magnetic resonance imaging.
and sensorimotor areas (precentral gyrus, premotor area, supplementary motor area, and sensory area), language areas (including: posterior superior temporal gyrus of the dominant hemisphere, posterior temporal gyrus of the dominant hemisphere, posterior temporal gyrus of the dominant hemisphere, and posterior temporal gyrus of the dominant hemisphere), and language areas. and sensorimotor areas (precentral gyrus, premotor, supplementary motor, and sensory areas), language areas (including: posterior superior temporal gyrus, posterior middle and inferior temporal gyrus, posterior inferior frontal gyrus, posterior middle frontal gyrus, superior limbic gyrus, angular gyrus, etc.), cortical and subcortical structures such as the basal ganglia or internal capsule, thalamus, and talar visual cortex of the dominant hemisphere 36. Modern cognitive neuroscience considers the distribution of functional areas of the brain as a highly complex topological network structure37, and gliomas in functional areas often invade key nodes or connections of the topological network structure, which can The glioma may cause direct or indirect neurological impairment in motor, language, cognition, and memory. The surgical approach and surgical technique for functional glioma surgery is unique.
-
Surgical approach: Currently, intraoperative awakening is recommended for patients with functional glioma. Intraoperative arousal with intraoperative functional brain localization 38-42is recommended to improve the extent of tumor resection and removal while effectively avoiding permanent postoperative sexual dysfunction.
Indications include: patients with glioma involving functional areas of the brain; subjective willingness to cooperate with functional positioning; and voluntary acceptance of wake-up anesthesia.
In addition to contraindications to craniotomy under conventional general anesthesia, contraindications should include 43: patients with severe preoperative intracranial hypertension or existing brain herniation with no improvement in function with conventional preoperative dehydration medications; presence of impaired consciousness or severe cognitive impairment; clear psychiatric history; communication impairment, severe neurological deficits, or difficulty cooperating with intraoperative testing tasks; and The anesthesiologist and surgeon have no experience with wake surgery; the patient refuses to undergo wake anesthesia; the patient is younger than 18 years of age (a relative contraindication) and is mentally retarded; the patient is not able to grow
Tolerance of fixed position for a long time, etc.
-
Preoperative evaluation: The three main components are imaging, neurological assessment, and preoperative education.
①Preoperative imaging assessment: MRI T1, T2, T2-FLAIR, T1 enhancement, task state BOLD-fMRI, DTI, 3D-T1WI are highly recommended. MRS, resting-state functional magnetic resonanceimaging (Rs-fMRI), PWI are recommended.
T1, T2, T2-FLAIR, T1-enhanced MRI sequences: can determine the extent of the lesion, edema and malignancy. The distance between the tumor invasion area and the functional area correlates with the functional status of the patient. BOLD-fMRI technique is commonly used to localize the motor and language functional areas of the extremities (level 3). However, when the tumor is close to the functional area (e.g., when the tumor is close to the hand motor area cortical<4mm), the accuracy of localization is reduced by the tumor (level 3 evidence)45, 46. 47, and it is recommended to use ZOOMit sequence for functional localization, which can effectively improve the localization accuracy.
(Level 3 evidence)48. The preoperative localization of the functional area by fMRI allows the operator to determine the extent of tumor resection intraoperatively, effectively avoiding permanent functional impairment after surgery (level 3 evidence)49. Rs-fMRI is an imaging method that does not require the patient to complete the task during the examination and is recommended as a complementary examination (level 3 evidence)50. It should be used in patients who are unable to cooperate with a completed BOLD-fMRI examination.DTI and fiber bundle tracking: strongly recommended in patients with glioma whose tumors invade functional brain areas to improve the extent of tumor resection while protecting the patient’s neurological function (level 3 evidence)51. span style=”font-size:16pt”>. Meanwhile.
This technique is recommended to be widely used in patients with non-functional gliomas to understand the tumor and surrounding neurofibrillary anatomy.
Preoperative neurological assessment: The objective neuropsychological scale is used to assess the patient’s functional status before surgery to help the surgeon develop a surgical and postoperative treatment plan. The preoperative neuropsychological scales are used to assess the functional status of the patient and to assist the operator in formulating the surgical and postoperative treatment plan. The scale should include normal range reference values and be reproducible.
Highly recommended: Kanofsky performance score (KPS), Edinburgh Leigh hand check.
Recommended (depending on the functional areas of the brain involved in the tumor): Wechsler Adult Intelligence Scale, Western Aphasia Suite Chinese version, Chinese Aphasia Suite The Wechsler Adult Intelligence Scale, the Chinese version of the Western Aphasia Battery, the Chinese Language Aphasia Battery, and neglect assessments (e.g., line segment equating test).
Recommendable: Wada Test, China Rehabilitation Research Center Aphasia Screening Method, Language Task Standard Atlas (2021SR0231666) ), Montreal Cognitive Assessment Scale (MoCA), Depression Self-Rating Inventory, Anxiety Self-Rating Inventory, Symptom Self-Rating Inventory.
③ Preoperative epilepsy assessment: the four aspects of the patient’s epilepsy history, symptoms of seizures, degree of seizures, and medication control are highly recommended Objective assessment. The International League Against Epilepsy (ILAE) Guidelines for the Treatment of Epilepsy 1981, 1990 Revision, and 2013 Edition52,
53, Clinical Guidelines for the Management of Diffuse Glioma-Associated Epilepsy in Adults (English version)
54.
-
Surgical preparation: incision design: the incision should be designed according to the location of the lesion and the functional area, and in principle should include the tumor and the important functions it involves
The brain area (monitoring target area). The following factors are taken into account: (1) Exposure of the lesion and surrounding functional areas for intraoperative monitoring and functional localization protection. The possibility of secondary surgery should be considered for tumors with high recurrence rate (e.g., glioma). (3) Inter-individual variability in the distribution of functional areas. (4) Structural factors such as subcutaneous arteries, venous sinuses, and hairline are often considered.
Positioning: often lateral or supine with a head frame. If supine is used, close attention should be paid to prevent intraoperative aspiration. The position chosen should ensure intraoperative comfort, and the use of a thermal blanket after positioning helps to reduce chills after awakening and the increase in intracranial pressure it causes.
Anesthesia: Current functional area glioma wake surgery includes intraoperative wake anesthesia for cranial functional area tumor resection and supervised anesthesia for the entire procedure. The two types of wake-up surgery include intraoperative wake-up anesthesia for cranial tumor resection and supervised anesthesia for full cranial tumor resection. Sleep-wake-sleep (AAA) anesthesia mode is the most commonly used anesthesia for wake-up surgery, which is a technique of deep anesthesia close to general anesthesia, and requires laryngeal mask, oropharyngeal airway with capsule and other auxiliary airway tools to keep the patient’s airway usual. The advantage of this procedure is that the patient is breathing spontaneously throughout the procedure, without the need for a laryngeal mask or other adjunctive ventilation device, and avoids intracranial pressure increase induced by removal of the mask after intraoperative awakening.
- Intraoperative maneuvers: craniotomy: local infiltrative anesthesia with head frame fixation staples, important scalp nerve blocks (supraorbital and supraglottic nerves, auriculotemporal nerve, lesser occipital nerve, greater occipital nerve, and third occipital nerve) and local infiltration anesthesia for the incision.
The incisional anesthesia covers the skin of the operative field, subcutaneously to the periosteum, including the basal part of the flap. The anesthesiologist is told to awaken the patient and to cover the dura with 2 lidocaine infiltrated cotton pads for 15 to 20 min. After the patient is awakened and in a stable general condition and mood, the dura is cut and suspended around the dura (without excessive traction) and the epidural is completely hemostatic55.
lidocaine infiltrated cotton pads for 15 to 20 min. After the patient is awakened and in a stable general condition and mood, the dura is cut and suspended around the dura (without excessive traction) and the epidural is completely hemostatic55.
Intraoperative imaging techniques: Intraoperative neuronavigation system is highly recommended; intraoperative MRI, intraoperative ultrasound, etc. are recommended. ①Neuronavigation system: intraoperative location of surgical resection and depth of resection can be determined based on the position of the navigation stick probe (level 3 evidence)56. ②Intraoperative MRI technique: can assist the operator to determine the volume of residual tumor after tumor resection and improve the final extent of tumor resection (level 3 evidence)57.
③Intraoperative ultrasound imaging: can assist in intraoperative determination of the extent of tumor and resection, and provide blood flow around and within the lesion.
Intraoperative functional brain localization techniques: direct electrical stimulation to localize functional cortical areas is highly recommended (level 2 and 3 evidence)58, 59; somatosensory evoked potentials to localize the central sulcus, continuous transcranial or transcortical motor evoked potentials to monitor motor pathway integrity, direct electrical stimulation to localize cortical and subcortical functional structures, and neuronavigation combined with preoperative fMRI localization images are recommended.
Motor Zone Monitoring: 1) Positive motor zone is indicated by involuntary muscle movements in the contralateral limb or corresponding part of the face, and electromyographic activity can be recorded. The motor area is positive for involuntary movements of the corresponding muscles of the contralateral limb or face. 60-62.
Sensory area monitoring: Positive sensory areas manifest as abnormal sensations in the contralateral limb or head in the form of pulses, mostly numbness; stimulation of sensory areas can also sometimes induce numbness.
Prompting limb movement.
Language area monitoring: the recommended language tasks are: counting and picture naming. Abnormalities during electrical stimulation (including interruptions, dysarthria, naming errors, unresponsiveness, repetition, etc.) suggest that this area is the language center associated with object naming63. Pictures of objects that have been standardized for Chinese language are recommended for picture materials. The important structures to be monitored and protected in the subcortical language areas are the arcuate fasciculus, superior longitudinal fasciculus, inferior occipitofrontal fasciculus, frontal oblique fasciculus, and inferior longitudinal fasciculus 64, 65.
Resection strategy: Select the appropriate surgical approach to remove the lesion as much as possible while preserving important functional structures. The current internationally accepted safe margin of resection should be at least 5 mm from the positive irritation zone (level 3 evidence)66. At the same time, care is taken to protect the normal arteries and important drainage vessels on the brain surface. The patient’s functional status is monitored continuously during resection, and subcortical electrical stimulation is performed immediately to identify and protect important subcortical functional structures when the presence of important subcortical pathways is suspected. After removal of the lesion, intraoperative MRI, intraoperative ultrasound, or tumor fluorescence imaging can be used to observe whether the lesion remains 67, 68.
-
Postoperative evaluation and prognosis: MRI within 24-72h postoperatively is highly recommended, and high-grade brain MRI enhancement for high-grade glioma and volumetric quantitative analysis of T2-FLAIR for low-grade glioma are recommended to evaluate the extent of tumor resection. It is recommended to evaluate the KPS score, speech function, motor function and quality of life at 1-3 days, 1 month, 3 months and 6 months after surgery. The evaluation process is recommended to use a combination of neuroimaging and behavioral scales.
The use of direct cortical and subcortical electrical stimulation techniques to localize and preserve functional areas during arousal surgery significantly reduces the incidence of permanent postoperative neurological deficits in patients, and temporary postoperative neurological deficits tend to recover within 3 months (level 3 evidence)69 =”font-size:16pt”>.
-
Surgical treatment to control glioma-associated epilepsy. Total glioma resection is superior to subtotal resection for postoperative epilepsy control (level 1 evidence)70, 71. Most patients with glioma-associated epilepsy are seizure-free after total glioma resection, and the largest possible lesion resection for postoperative seizure control is performed when safe and feasible (level 2 evidence)72. size:16pt”>. Patients with preoperative glioma with secondary grand mal seizures and tumor calcification had a better prognosis for postoperative epilepsy (level 3 evidence)73. In patients with temporal lobe glioma-associated epilepsy, tumor resection combined with selective resection of the hook gyrus and amygdala and/or anterior temporal cortical resection may improve postoperative seizure control compared with lesion resection alone (level 2 evidence). However, the decision to preserve hippocampal structures should be considered in the context of the patient’s actual needs for memory and learning.
The risk of seizures due to glioma is related to the area of the brain involved in the tumor
(Level 2 evidence)74. Gliomas in functional areas have a relatively limited scope of surgical resection and a relatively high incidence of postoperative seizures, and the existing techniques should be fully utilized to remove as many tumors as possible to reduce postoperative seizures while preserving brain function (level 3 evidence)75.
For patients with glioma with epilepsy, intraoperative skin is recommended as appropriate
Intraoperative electroencephalography or deep EEG monitoring is recommended for patients with glioma with epilepsy to guide the extent of resection of epileptic foci to improve the patient’s epilepsy prognosis and improve long-term epilepsy cure rates (level 2 evidence)76.
-
Intraoperative seizure control: gliomas involving functional areas of the brain in intraoperative electrical stimulation of functional areas localized with some risk of seizures (level 2 evidence)77, 78, when intraoperative EEG monitoring or symptomatic observation suggests that the patient is experiencing seizures with Local flushing with ice Ringer’s solution or ice saline can control most seizures (level 2 evidence)79. Seizures may be terminated with antiepileptic, sedative, or inotropic medications if persistent seizures remain (Level 4 evidence)
78.
-
Surgical treatment of epilepsy associated with refractory glioma: recurrence or exacerbation of epilepsy during the application of antiepileptic drugs is often indicative of tumor progression (level 2 evidence)80, and recurrence of seizures after a prolonged period without seizures after glioma surgery may indicate tumor recurrence (level 2 evidence)81. In the case of recurrent glioma with frequent drug-refractory seizures, the patient’s condition can be treated surgically. Postoperative glioma without recurrence with frequent seizures may be evaluated comprehensively as refractory epilepsy, and surgery may be considered for drug-refractory glioma-associated epilepsy with significant impact on quality of life (level 3 evidence)82.
Radiotherapy is usually administered with a 6-10 MV linear gas pedal, routinely fractionated and opportunistic, after the tumor pathology has been defined, and stereotactic radiation therapy is not indicated for primary treatment of glioma.
Surgery is the basic treatment and radiotherapy/chemotherapy etc. are essential and important treatment.
Significant survival benefit can be achieved with postoperative radiotherapy for high-grade glioma (level 1 evidence).
-
Timing of radiotherapy: survival time in high-grade glioma is strongly correlated with the timing of initiation of radiotherapy . 83, early postoperative radiotherapy is effective in prolonging patient survival, and starting radiotherapy as early as possible after surgery (2-6 weeks postoperatively) is strongly recommended (level 2 evidence).
-
Radiotherapy techniques: 3D Conformal radiotherapy or conformal modulation techniques, routinely fractionated, are recommended to improve target dose coverage, conformality and protection of normal tissues, reduce unnecessary irradiation volume and complications (level 2 evidence)84. size:16pt”>, pre-radiotherapy image verification is an indispensable part of radiotherapy quality control.
-
Radiotherapy dose: Recommended radiotherapy The total irradiation dose is 54-60 Gy, routinely fractionated, and the total irradiation dose can be appropriately reduced for larger tumors and/or located in critical functional areas and grade 3 gliomas (level 1 evidence)85. Although 3D conformal radiotherapy or conformal intensity modulation techniques have the ability to increase the conformality of the target area, reduce the amount of normal tissue exposed, minimize the irradiation volume, and give a higher dose to the target area, the efficacy of the increased dose has not been proven, and it is prudent to blindly increase the total dose or fractionated dose.
-
Target area determination: The target area of radiotherapy for high-grade glioma is still controversial, focusing mainly on the initial clinical target area (the “clinical target area”). The main focus is whether the initial clinical target volume (CTV) needs to include the peritumoral edema area, and the American Society for Therapeutic Oncology
The Radiation Therapy Oncology Group (RTOG) recommends that the CTV1 should include the 2 cm area outside the periampullary edema zone. CTV2 should be outside the gross tumor target volume (GTV) after field reduction.
2 cm outside the gross tumor target volume (GTV) and a dose of 14 Gy. cm at a dose of 14 Gy. 2021 US National Comprehensive Cancer Network
(National Comprehensive Cancer Network, NCCN) guidelines recommend MRI T1 enhancement or T2-FLAIR abnormal signal as GTV with 1 to 2 cm of outgrowth to form CTV; if edema area is considered, it is recommended to include it in a course of CTV1
(46Gy/23f), second-pass incremental area (14Gy/7f) CTV2 includes only residual tumor and/or postoperative tumor cavity with appropriate external expansion. Phase II clinical trials confirmed that there was no significant difference in tumor control and survival with or without the inclusion of the edema zone in the target area86, 87, European Organisation for the Research and Treatment of Cancer (EORTC) Organisation for the Research and Treatment of Cancer (EORTC) recommended CTV settings that do not emphasize the need to include all areas of peritumoral edema.
The principle of target area mapping is to ensure that the tumor is illuminated at a dose of 60Gy as much as possible with safety in mind, and that target area mapping should refer to pre/post-operative MRI. In clinical practice, physicians should apply the above recommendations on target area setting flexibly, balancing the relationship between irradiation dose, volume and radiation damage, based on a combination of factors such as target area location, volume, patient age and KPS score.
- style=”margin-left: 78pt”>
- Combination radiotherapy: simultaneous application of radiotherapy and temozolomide.
①GBM: radiotherapy combined with temozolomide (75 mg/m2 is strongly recommended for adults with primary treatment “font-size:16pt”>) with concurrent chemotherapy and subsequent 6 cycles of temozolomide (150-200 mg/m2) adjuvant chemotherapy, during and after radiotherapy Temozolomide significantly prolonged patient survival (level 1 evidence)88, and this synergistic effect was most pronounced in patients with methylation of the MGMT promoter region (level 2 evidence)89.
②Grade 3 glioma: For patients with 1p/19q combined deletion on chem/
Radiotherapy is more sensitive (level 1 evidence)90, 91< span style="font-size:16pt">, radiotherapy combined with PCV (methylphenidate + lomustine + vincristine) chemotherapy is the first-line treatment option (level 1 evidence), and temozolomide is now showing preliminary efficacy in grade 3 gliomas (level 2 evidence) with fewer side effects. Two large randomized clinical trials examining the relationship between temozolomide, radiotherapy, and 1p/19q combination deletion are ongoing, with interim results showing that radiotherapy combined with 12 cycles of temozolomide chemotherapy significantly improves patient survival in the absence of 1p/19q combination deletion92 Patients with IDH wild type with or without TERT promoter region mutations have the worst clinical prognosis and should be treated with increased intensity of radiotherapy, also in grade 2 gliomas 93. span style=”font-size:16pt”>.
Radiation therapy for grade 3 glioma should be individualized according to the patient’s specific situation, including general status, molecular pathology, and treatment needs. The treatment options include radiotherapy combined with PCV regimen/temozolomide and participation in clinical trials.
The indications, optimal timing, and dose of postoperative radiotherapy for low-grade gliomas are controversial, and treatment strategies are usually based on the patient’s prognostic risk.
-
Risk factors: age ≥40 years, incomplete tumor resection, large tumor size, preoperative neurological function large volume, preoperative neurological deficits, and IDH wild type are poor prognostic factors 94, 95. Aggressive early treatment is recommended for patients whose tumors are not completely resected or who are ≥40 years of age. Patients aged <40 years with fully resected tumors may be selected for close observation.
96, but the decision should be made carefully after taking into account the patient’s condition and molecular pathology.
- style=”margin-left: 72pt”>
- Radiotherapy dose: The recommended total radiotherapy dose for low-grade glioma is 45 to
- Radiotherapy dose: The recommended total radiotherapy dose for low-grade glioma is 45 to
54 Gy in fractionated doses of 1.8-2.0 Gy (level 1 evidence )97. For IDH wild-type low-grade gliomas (grade 4 astrocytomas as defined by the 2021 WHO classification), a dose increase to 59.4-60 Gy is required. With the widespread use of conformal intensity-modulated radiotherapy and molecular staging in the clinic, a modest increase in radiotherapy dose (54-59.4 Gy) can help prolong patient survival, especially for astrocytomas defined by molecular pathology or MGMT promoter non-methylation. Patients 98, 99. Split doses above 2 Gy increase the risk of distant cognitive impairment (level 2 evidence)100.
-
Target area determination: GTV is mainly based on pre/post-operative MRI T2- FLAIR abnormal signal It is particularly important to correctly distinguish tumor remnants from postoperative changes, and a 1 to 2 cm outgrowth of the GTV is recommended as the CTV for low-grade gliomas.
Surgery is the treatment of choice for ventricular meningeal tumors, and after total tumor resection most patients advocate no adjuvant therapy, while partial resection of ventricular meningioma and mesenchymal ventricular meningioma are indications for radiotherapy (level 3 evidence). Level 3 evidence)101. Chemotherapy may be an adjuvant treatment option for those who have a short-term relapse after radiotherapy or are too young for radiotherapy, but the efficacy is uncertain.
Total brain and spinal cord MRI and cerebrospinal fluid exfoliation cytology are required 3 weeks after ventricular tumor surgery, and local radiation therapy is recommended for those without evidence of brain and spinal cord tumor dissemination, and whole brain and spinal cord radiation therapy is recommended for those without evidence of brain and spinal cord tumor dissemination. Radiotherapy (level 3 evidence)102, 103.
Local radiotherapy: local tumor irradiation was determined based on pre/post-operative MRI, usually using enhanced T1 or T2-FLAIR abnormal signal for GTV, CTV for GTV extrapolation 1 to 2 cm, fractionated dose 1.8 to 2.0 Gy/time, total intracranial tumor dose 54 to 59.4 Gy Dose 54-59.4 Gy, tumor dose 45 Gy in the spinal cord region, if the tumor is located in the spinal cord
The total dose can be increased to 60 Gy if the tumor is located below the cone.
Whole brain and whole spinal cord radiation therapy: whole brain including the area within the dura mater, whole spinal cord from the first cervical medulla down to the caudal dural sac, whole brain and whole spinal cord irradiation The total dose was 36 Gy, 1.8-2.0 Gy each time, with additional doses to 54-59.4 Gy for subsequent intracranial lesions and 45 Gy for spinal lesions.
- style=”margin-left: 54pt”>
- Recurrent glioma
The location and size of the tumor should be fully considered when evaluating the safety of recurrent glioma recourse radiotherapy. For smaller recurrent lesions, most retrospective studies have used stereotactic radiosurgery or hypofractionated stereotactic radiotherapy techniques104, 105, while conventional fractionated radiotherapy studies have traditionally focused on relatively large recurrent lesions. mostly focused on relatively large volume recurrent
The conventional fractionated radiotherapy studies are mostly focused on relatively large recurrent lesions, and the superimposed doses may cause severe brain tissue damage. The risk of brain tissue tolerance and radiation necrosis should be fully considered106. Studies have shown that radiotherapy combined with bevacizumab and temozolomide prolonged progression-free survival and overall survival in some patients 107, 108.
Brain tissue damage from radiotherapy is classified into three different types depending on the time of onset and clinical presentation: acute (during or within 6 weeks after radiotherapy), subacute (within 6 weeks after radiotherapy), and subacute (within 6 weeks after radiotherapy).
(6 weeks to 6 months after radiotherapy) and advanced (months to years after radiotherapy).
-
Acute and subacute radiation injury: Acute and subacute radiation injury may be due to vasodilation, blood-brain barrier acute and subacute radiation injury: acute and subacute radiation injury may be caused by vasodilation, blood-brain barrier damage and edema. Acute injuries are characterized by signs of cranial hypertension, such as nausea, vomiting, headache, and drowsiness. It is usually transient and reversible, and can be relieved by corticosteroids, sometimes on MRI.
The subacute radiation brain injury presents with drowsiness and fatigue and usually resolves spontaneously within a few weeks, with corticosteroids administered as necessary to control symptoms.
-
Late radiation injury: Late radiation reactions are often progressive and irreversible. The radiation response is often progressive and irreversible, including leukoencephalopathy, radionecrosis, and a variety of other lesions (mostly vascular in nature). The total dose of radiation therapy, fractionated dose, etc. is directly related to the development of leukoencephalopathy109, 110. Non-treatment-related factors including concomitant diseases that increase susceptibility to vascular injury, such as diabetes, hypertension, and advanced age, can increase the incidence of white matter encephalopathy. Synchronous chemotherapy is another risk factor 110. The incidence of pseudoprogression is significantly higher after synchronous radiotherapy for glioma temozolomide, which is essentially early radiation necrosis. The most serious late reaction to radiotherapy is radionecrosis, with an incidence of about 3
 to 24
to 24  . The peak occurs 3 years after radiation therapy. The clinical manifestations of radiation necrosis are similar to those of tumor recurrence, such as the reappearance of initial symptoms, worsening of existing neurological deficits and the imaging of progressive and irreversibly enhancing lesions with associated edema. The prevention of radiation damage is fundamental, and rational planning of total dose, fractionation, and appropriate target volume can effectively reduce the incidence of radionecrosis.
. The peak occurs 3 years after radiation therapy. The clinical manifestations of radiation necrosis are similar to those of tumor recurrence, such as the reappearance of initial symptoms, worsening of existing neurological deficits and the imaging of progressive and irreversibly enhancing lesions with associated edema. The prevention of radiation damage is fundamental, and rational planning of total dose, fractionation, and appropriate target volume can effectively reduce the incidence of radionecrosis.Chemotherapy is a treatment that kills tumor cells through the use of chemicals, and chemotherapy can prolong progression-free survival and overall survival in patients with glioma 111, 112. High-grade gliomas grow and recur rapidly, and aggressive and effective individualized chemotherapy is more valuable. Other drug therapies such as molecular targeting and bioimmunotherapy are currently in clinical trials. We encourage those who are qualified and eligible to
eligible patients are encouraged to participate in clinical trials of drugs at different stages of disease. . 1.
- The extent of tumor resection affects the effectiveness of chemotherapy. Chemotherapy is recommended on the basis of maximum safe tumor resection.
- Adequate chemotherapy should be started as soon as possible after surgery. Optimal results can be achieved by completing the established regimen with safety in mind, while paying attention to drug toxicity and monitoring immune function.
- Select drugs with different mechanisms of action and non-overlapping toxicity for combination chemotherapy to reduce the incidence of toxicity and drug resistance.
- Select appropriate chemotherapy regimens based on histopathology and molecular pathology.
-
Some antitumor and antiepileptic drugs can interact with each other and should be used together with discretion.
-
(1) Classical chemotherapy regimens.
①Stupp regimen: Simultaneous oral temozolomide 75mg/ during radiotherapy
(m2-d) for 42 days; 4 weeks after the completion of synchronous radiotherapy, enter the adjuvant chemotherapy phase with oral temozolomide 150-200mg/(m2. size:16pt”>-d) for 5 days and repeated every 28 days for 6 cycles.
②PCV regimen: methylbenzylhydrazine 60mg/(m2< span style="font-size:16pt">-d) day 8-21, lomustine 110mg/(m2-d) day 1, vincristine 1.4mg/m2day 8, 29, 8 weeks for 1 cycle.
-
Other drugs used in glioma treatment are carmustine, irinotecan
(2) Chemotherapy for grade 3 glioma: There is no standard regimen for chemotherapy for grade 3 glioma, and radiotherapy combined with PCV/timozolomide is recommended under molecular pathology guidance. PCV/temozolomide in multiple chemotherapy regimens (level 2 evidence)113, or to participate in clinical trials.
Grade 3 oligodendroglioma with 1p/19q combined deletion, recommended for radiotherapy 102 plus PCV chemotherapy regimen (level 1 evidence)90, 91 size:16pt”>, radiotherapy plus concurrent and/or adjuvant temozolomide chemotherapy (level 2 evidence)90, 91; radiotherapy plus adjuvant temozolomide chemotherapy recommended for those without 1p/19q combination deficiency; radiotherapy plus adjuvant temozolomide chemotherapy recommended for those without 1p/19q combination deficiency Temozolomide chemotherapy 114.
Grade 3 glioma with KPS<60, short course or conventional radiotherapy combined with temozolomide chemotherapy recommended (level 2 evidence) 115.
-
GBM chemotherapy (age ≤70 years): KPS ≥60 Patients with MGMT promoter region methylation, conventional radiotherapy plus synchronous and adjuvant temozolomide chemotherapy with or without electric field therapy (level 1 evidence)85, conventional radiotherapy may also be recommended Add synchronous and adjuvant temozolomide combined with lomustine chemotherapy (level 2 evidence) 116 or clinical trials; for MGMT promoter region non-methylation or unclear methylation, recommend Radiotherapy plus concurrent and adjuvant temozolomide chemotherapy with or without electric field therapy (level 1 evidence)85, or clinical trials.
Patients with KPS<60, short course of radiotherapy with or without synchronous and adjuvant temozolomide chemotherapy is recommended (level 2 evidence)115; temozolomide chemotherapy alone is also recommended in the presence of methylation of the MGMT promoter region (level 2 evidence).
- Chemotherapy for mesenchymal ventricular meningioma: Chemotherapy is usually administered in the setting of tumor recurrence or whole-brain, whole-spinal cord dissemination, with the following agents: platinum, etoposide, and etoposide.
Lomustine, carmustine, and temozolomide, etc., or in clinical trials. 3.
There are many controversies in chemotherapy for low-grade glioma, including the timing of chemotherapy, chemotherapy regimen, and the sequence of chemotherapy and radiotherapy.
According to current evidence-based medicine, radiotherapy combined with chemotherapy should be actively considered for patients with high-risk low-grade glioma . span style=”font-size:8pt”>117, 118. Recommended chemotherapy regimens include: PCV regimen (level 1 evidence)119; temozolomide chemotherapy (level 2 evidence)120; Temozolomide concurrent and/or adjuvant chemotherapy (level 2 evidence)120 size:16pt”>.
Appropriate targeted agents may be recommended for patients with low-grade gliomas with BRAFV600E activating mutations or NTRK fusions.
There is no standard chemotherapy regimen for recurrent glioma after standard treatment. In the case of high-grade recurrent glioma, it is strongly recommended that clinical trials be preferred, and if no appropriate clinical trials are available, the following regimens may be used.
(1) Optional regimens after relapse of low-grade glioma: (1) radiotherapy plus adjuvant PCV chemotherapy; (2) radiotherapy plus adjuvant temozolomide chemotherapy; (3) radiotherapy (2) radiotherapy plus adjuvant temozolomide chemotherapy; (3) radiotherapy with concurrent and adjuvant temozolomide chemotherapy; (4) temozolomide for patients with no prior history of temozolomide treatment 120; (5) lomustine or carmustine; (6) PCV regimen 121; (vii) carboplatin or cisplatin-based chemotherapy regimens 122 ;⑧Targeted agents may be recommended for those with BRAFV600E activating mutations or NTRK fusions.
(2) Optional regimens after relapse of grade 3 glioma: ① Temozolomide 123; ② lomustine or carmustine 124; ③ PCV regimen; ④ bevacizumab 125; ⑤ bevacizumab plus chemotherapy (carmustine/lomustine, temozolomide); ⑥
Etoposide126; (vii) carboplatin- or cisplatin-based chemotherapy regimens; and (viii) appropriate targeted agents can be recommended in the presence of BRAFV600E activating mutations or NTRK fusions.
(3) Options after GBM relapse: ①Bevacizumab 127; (ii) Temozolomide 128; (iii) lomustine or carmustine; ④ PCV regimen; ⑤ regorafenib129; ⑥ bevacizumab plus chemotherapy (carmustine/lomustine, temozolomide); ⑦ etoposide; ⑧ carbostatin or cisplatin-based platinum or cisplatin-based chemotherapy regimens.
9 Targeted agents may be recommended for those with BRAF V600E activating mutations or NTRK fusions.
The principle of electric field for tumor therapy is to continuously influence the arrangement of polar molecules in tumor cells by means of alternating electric field with low field strength at medium frequency, thus interfering with the mitosis of tumor cells and exerting anti-tumor effects. The electric field is used to treat glioma. The electric field therapy system for glioma treatment is a non-invasive, portable device that works by applying an electric field patch to the scalp, which has been shown to be safe and effective130. Recommended for newly diagnosed GBM (level 1 evidence) and recurrent high-grade glioma
(Level 2 evidence). In May 2020, the State Drug Administration approved the marketing application for electric field therapy and approved its use in combination with temozolomide for newly diagnosed GBM (Level 1 evidence). In May 2020, the State Drug Administration approved the marketing application for electric field therapy and approved its use in combination with temozolomide for the treatment of patients with newly diagnosed GBM and as monotherapy for the treatment of patients with relapsed GBM.
(E) Principles of glioma treatment in the elderly.
There is no uniform definition of old age, and this guideline refers to those aged >70 years. The main molecular genetic features of GBM include ATRX
BRAF, IDH, and TP53 mutation rates are significantly decreased and PTEN mutation rate is significantly increased.
131 , TP53 mutations and EGFR amplification may be associated with patient prognosis 132 . Aging
The main treatment options for GBM patients include surgical resection, radiotherapy, and temozolomide chemotherapy. For older GBM patients with KPS ≥60, the US 2021 NCCN guidelines also recommend electric field therapy (Level 1 evidence).
- style=”margin-left: 54pt”>
- Surgical treatment
Surgical resection of tumors provides a definite survival benefit in older GBM patients (level 1 evidence)133, and total tumor resection is more beneficial for postoperative functional recovery (level 2 evidence)134. Surgical resection has a good safety and clinical benefit in those with a good evaluation of the comprehensive geriatric status assessment 135. Therefore, surgery is also recommended as a priority for older patients with glioma, whereas surgery needs to be considered carefully in older patients over 80 years of age and is not recommended for older patients with poor preoperative scores.
- style=”margin-left: 54pt”>
- Radiotherapy and chemotherapy
Radiotherapy and chemotherapy can definitively extend the overall survival time of patients. Short-course or conventional radiotherapy combined with temozolomide chemotherapy (level 1 evidence)136is recommended for elderly GBM patients with KPS ≥60; short-course radiotherapy or temozolomide chemotherapy is recommended for those with KPS<60 radiotherapy or temozolomide chemotherapy.
(F) Principles of treatment for diffuse midline glioma.
Diffuse midline gliomas are gliomas of the midline structures that occur in the thalamus, brainstem, and spinal cord. There is no definitive epidemiological data in China, but overseas reports suggest that the peak incidence is 6-7 years in children and 20-50 years in adults, with no significant gender differences137, with difficult treatment and very poor prognosis. The 2021 WHO classification of central nervous system tumors designates diffuse midline glioma as grade 4. Clinical and imaging
Patients with suspected diffuse midline glioma It is recommended to test for H3K27M mutations, mainly H3.3 K27 mutations, H3.1/2 K27 mutations, H3 wild with EZHIP overexpression, and EGFR mutations, of which H3K27M mutations are the most common alterations in pediatric diffuse endogenous pontine glioma, and patients with worse prognosis 138, 139.
The tumor is in a critical location and is infiltrative in growth, making complete resection difficult and usually not routinely recommended. In most cases, tumor biopsy is possible and recommended to clarify pathology and molecular pathology and to guide comprehensive treatment.
140.
There are no established radiotherapy and chemotherapy regimens. Radiotherapy may improve the objective tumor response rate in some patients (level 3 evidence)141, which can be referred to the GBM treatment protocol . size:8pt”>142, with appropriate adjustment of radiotherapy dose according to the specific situation. Radiotherapy combined with temozolomide chemotherapy or targeted therapy is also a treatment option 142, 143, and appropriate patients are recommended for clinical trials.
(vii) Rehabilitation and palliative care.
Most patients with glioma have varying degrees of postoperative physical and psychosocial impairments that limit their daily activities and social participation. These impairments limit patients’ daily activities and social participation, and reduce their quality of life. Reasonable and appropriate rehabilitation therapy can effectively reduce the disability rate associated with glioma and is an essential part of the clinical management of glioma. In addition, patients with glioma require comprehensive palliative care throughout the disease process, and appropriate palliative care can effectively reduce the symptom burden of patients with glioma and improve patient outcomes, especially for those with glioma.
for patients with end-stage disease) and caregivers. The clinical management of these two types of treatments also requires the attention of the glioma treatment team.
- style=”margin-left: 54pt”>
- For the rehabilitation of glioma patients, a three-level rehabilitation service system is recommended: primary rehabilitation refers to the early rehabilitation of patients in the neurosurgical oncology ward. The early rehabilitation treatment in the neurosurgical oncology ward is the post-operative rehabilitation activities guided by neurosurgical oncologists to address the possible post-operative complications and dysfunction of the patient, and is recommended to be carried out when the patient’s vital signs are stable after surgery or other treatments. If the patient’s function is relatively well recovered, the rehabilitation physician can provide rehabilitation education to the patient and family members, so that the patient can do rehabilitation exercises at home.
The rehabilitation problems caused by glioma can be divided into three levels: disability, activity limitation, and participation restriction. (1) Disabilities: These include muscle weakness, sensory deficits, balance disorders, swallowing disorders, dysarthria, aphasia, cognitive disorders, and psychological disorders. The muscle strength can be assessed by the unassisted muscle strength test, sensory deficits can be assessed by the Fugl-meyer extremity sensory function assessment, balance impairment can be assessed by the Berg Balance Scale, swallowing impairment can be assessed by the Puddlefield drinking test and video pharyngography, dysarthria can be assessed by the modified Frenchay method, aphasia can be assessed by the Boston diagnostic aphasia test, and cognitive impairment can be assessed by the Boston diagnostic aphasia test.
Cognitive impairment can be assessed with the Simple Mental State Examination, the Anxiety and depression can be assessed by the Hamilton Anxiety and Depression Inventory. (2) Activity limitation: The above neurological impairment causes difficulty in mobility and self-care. The Basel Index and the Functional Independence Scale can be used to assess this. (3) Participation limitations: Difficulties in employment, family life, and social integration due to the above neurological impairment. This can be assessed using the Health Survey Scale 36.
The rehabilitation of patients with glioma involves multidisciplinary and interdisciplinary cooperation and requires a collective and collaborative working model.
The rehabilitation of patients with glioma involves a multidisciplinary and interdisciplinary approach, and a wide range of rehabilitation strategies.
-
Motor impairment treatment: Motor impairment in glioma patients is not necessarily caused by the glioma itself, but can also be the result of surgical resection, radiation therapy, and other treatments. It may be a complication of surgical resection, radiotherapy and chemotherapy. The rehabilitation treatment is based on exercise therapy, including proper body positioning, joint mobility exercises, muscle strength training, endurance training, neuromuscular facilitation techniques, balance and coordination training, gait training, and breathing training. For patients with glioma who are physically able to support normal exercise, international expert organizations recommend at least 150 minutes of moderate-intensity or 75 minutes of high-intensity aerobic exercise per week, with strengthening exercises for two major muscle groups
144. In addition, for some patients who develop motor dysfunction after surgery, the
Transcranial magnetic stimulation is used to stimulate important functional network nodes to promote node remodeling and accelerate postoperative motor function recovery 145 >.
- Sensory impairment treatment: In patients with glioma, sensory impairment is usually caused by direct damage to the somatosensory pathways, including the primary sensory cortex
Sensory impairment in patients with glioma is usually caused by direct damage to somatosensory pathways, including primary sensory cortex. After effective treatment of the primary tumor or discontinuation of the chemotherapeutic agent causing the complication, the sensory disorder may resolve or improve significantly. Patients with sensory impairment require appropriate rehabilitation to prevent progressive decline in sensory function. Physical therapy usually targets static posture, transfer and gait, and encourages patients to rely more on visual than sensory perception of their surroundings. In addition, patients can be trained to use assistive devices such as crutches when walking and walking up and down stairs to compensate for reduced proprioceptive acuity in the lower extremities.
-
SpeechSpeech Disorders Treatment: Speechspeech disorders include dysarthria and aphasia, etc., which require separate training to promote speech and language restoration and non-speech therapy based on the results of speechlanguage assessment. The former included phonological training, auditory training, and training in the use of nonverbal communication modalities. The former included speech training, auditory comprehension, and oral expression training, while the latter included sign language, drawing, communication boards, communication manuals, and computerized communication devices.
-
Swallowing Disorder Treatment:63
 of brain tumor patients develop swallowing disorders in early rehabilitation, and swallowing disorders usually improve gradually, with 50
of brain tumor patients develop swallowing disorders in early rehabilitation, and swallowing disorders usually improve gradually, with 50  of patients can return to a normal diet at discharge. Rehabilitation strategies for swallowing disorders include changes in nutritional intake pathways, rehabilitation training to promote swallowing recovery, modification of food properties and eating positions, and rehabilitation care and education related to swallowing rehabilitation.
of patients can return to a normal diet at discharge. Rehabilitation strategies for swallowing disorders include changes in nutritional intake pathways, rehabilitation training to promote swallowing recovery, modification of food properties and eating positions, and rehabilitation care and education related to swallowing rehabilitation. -
Treatment of cognitive impairment: Gliomas and their associated treatments can lead to cross-sectional impairment of cognitive function Gliomas and their associated treatments can lead to cross-sectional impairments in cognitive function, mostly in the form of memory deficits (mainly working memory), executive function, attention, orientation, and visuospatial dysfunction. Previous studies have demonstrated that standardized cognitive rehabilitation helps patients with glioma to recognize
Cognitive The improvement of function. Cognitive rehabilitation includes education to increase awareness and understanding of cognitive deficits, adaptive therapy to reduce the impact of cognitive deficits, and restorative therapy to address cognitive deficits, with the adaptive and restorative therapies being guided by the patient’s lifestyle and work needs.
- Psychotherapy: Anxiety and depression in patients with glioma can be alleviated and eliminated through psychological interventions. For patients with moderate to severe anxiety or depression, anti-anxiety and depression medications can be given as appropriate. Psychological support and education of the patient’s family and caregivers should also be taken into account.
-
Occupational therapy: Occupational therapy refers to the application of various work activities related to daily life, work, or a part of a process as a form of training. The treatment is designed to improve the patient’s independence in self-care, work, and leisure activities by applying a certain motor part of the process. This includes basic occupational therapy necessary to maintain daily living, value-creating occupational therapy, recreational or leisure occupational therapy, educational occupational therapy, and training in the use of assistive devices.
-
Rehabilitation engineering: For glioma patients with limb weakness and balance disorders, rehabilitation For glioma patients with limb weakness and balance disorders, various assistive devices can be made through rehabilitation engineering to improve the patient’s ability to perform daily living. For example, ankle-foot orthoses are used to improve foot drop, and broad-based quadrupeds, standard walkers, or semi-walkers are used to increase the support surface to reduce the risk of falling while walking or standing.
-
Medication: Patients with symptoms such as limb spasm or pain, lung and urinary tract infections, depression or anxiety during rehabilitation. If the patient has symptoms such as spasm or pain, lung and urinary tract infections, depression or anxiety, it is necessary to use symptomatic medications as appropriate. At the same time, symptomatic supportive medications should be used with caution, as they may be the cause of cognitive impairment.
. In addition, medications are not recommended for patients with glioma for reasons of preventing or treating cognitive decline.
-
Traditional Chinese medicine and other rehabilitation therapies: Acupuncture, tui na, and boxing exercises may be chosen for the rehabilitation of patients with glioma.
Palliative care, also known as palliative care, is given to patients with limited survival (including patients with malignancy as well as non-oncology, e.g., when malignancy is diagnosed as advanced, when chronic heart failure is advanced, and when chronic heart failure is advanced). Palliative care, also known as palliative care, is a form of treatment given to patients with limited survival (including malignancy and non-oncology patients, such as those with advanced malignancy diagnosis, advanced congestive heart failure, and end-stage chronic obstructive pulmonary disease) and their families to provide comprehensive and integrated treatment and care to ensure the quality of life of the end-stage patients and to help their families through this difficult period. The primary goal of palliative care is not to prolong life or cure the disease, but to reduce symptoms and maintain or improve function and quality of life. According to the World Health Organization, palliative care “should be used early in the course of the disease, in combination with other therapies designed to prolong life. Since most patients with gliomas are incurable, palliative care is particularly important in this patient population, especially at the end of life. According to the European Neuro-Oncology Society’s 2017 guidelines for palliative care of patients with glioma, end of life is defined as the last 3 months of life before death.
Physicians need to be aware of the following basic principles when performing palliative care.
(1) patient-centeredness; and (2) concern for the patient’s wishes, comfort, and dignity.
(3) Not focused on curing the disease; (4) Accepting the inevitability of death.
(5) Not hastening nor delaying death.
Symptom management is the foundation and core component of palliative care. Symptom reduction and keeping the patient as physically comfortable as possible is the basis for caring for the patient on other levels, including psychological and social.
Patients with glioma have strong individual differences in clinical symptoms depending on the nature, location, and treatment of the disease. Headache, seizures, venous thrombosis, fatigue, mood and behavioral disturbances are common problems. Symptomatic management is the first step in helping patients with end-stage disease, and it needs to be adjusted as the patient’s condition changes until the best outcome is achieved. In the terminal phase of the disease, special attention is given to: (1) delirium control; (2) nutritional and respiratory support; (3) pre-emptive treatment planning; and (4) physician-patient communication and organization.
V. MDT
The MDT for glioma is a collaborative process in which professionals from multiple disciplines discuss and integrate the opinions of different disciplines based on the disease status and various aspects of the actual situation of different glioma patients. The aim is to provide individualized and comprehensive treatment services for glioma patients146 >. The goal of the Glioma MDT is to integrate neuro-oncology-related multidisciplinary strengths to provide patient-centered, one-stop care and achieve optimal sequential treatment.
The MDT is organized in the form of MDT case conferences and MDT joint clinics . “MDTs provide many benefits to patients with glioma: (1) they improve patient compliance with established treatment protocols while facilitating access to care; (2) they increase the likelihood that patients will enter clinical trials; and (3) they improve the likelihood that patients will enter clinical trials. MDTs can improve
Improve patient prognosis; ④MDTs contribute to the development of clinical trials and research. MDTs also bring many benefits to the health care team: (1) improved communication among health care team members and increased learning and education opportunities for team members; (2) shared decision making and better access to best practice and evidence-based advice when MDTs are implemented; (3) shared responsibility for clinical decision making and treatment implementation in MDTs reduces team members’ work stress and medical disputes; and (4) shared responsibility for clinical decision making and treatment implementation in MDTs reduces medical disputes. MDTs also facilitate research and improve the academic standards of medical units.
MDTs are composed of physicians and specialists in related specialties. It is recommended to organize the implementation of the MDT members for glioma with key clinical issues according to the different stages of disease diagnosis and treatment. Core clinical specialties include neurosurgery, medical imaging, neuropathology and molecular pathology, radiation oncology, neuro-oncology, and neurology. Other optional specialties include infection, hematology, endocrinology, neuropsychology, neurorehabilitation, clinical nursing, biospecimen banking, and palliative care. The experts should participate in MDT discussions regularly and be responsible for providing cases and preparing materials, etc.; (3) recorder: record the whole MDT and compile clinical data of MDT cases; (4) secretary (coordinator): assist the convener in organizing the whole MDT; (5) MDT committee: consider setting up an MDT committee to formulate MDT system and supervise MDT implementation. The MDT should set the convener (chief expert) of each case conference according to the key clinical problems to be solved. The convener is usually an authoritative expert from the patient’s primary clinical department, and the chair is
and participate throughout the discussion.
For first-time patients, the MDT implementation pathway includes a discussion of the diagnosis and differential diagnosis, and a decision on whether to operate and how to operate after the proposed diagnosis of glioma. For postoperative patients, tissue specimens are obtained and an accurate integrated pathology report is obtained after histopathologic diagnosis and molecular testing, and the next treatment option is discussed if the diagnosis of glioma is clear. If the pathology is doubtful, the next step is discussed (e.g., transfer to other related departments for treatment or observation). During the course of treatment and follow-up, the MDT can be brought back to discuss the treatment plan if necessary, and for patients with suspected recurrence, the nature of the lesion (e.g., response to treatment, tumor progression) and the next step in treatment should be discussed. The MDT should be supported by the hospital administration, and a system of clinical data management and feedback on outcomes should be established.





 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202244.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202244.png" alt=""/>






 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202253.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202253.png" alt=""/>






 < span style="font-size:10pt">
< span style="font-size:10pt">




 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202268.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202268.png" alt=""/>


 Appendix I Levels of Evidence (Oxford Centre for Evidence-Based Medicine 2011 Edition)
Appendix I Levels of Evidence (Oxford Centre for Evidence-Based Medicine 2011 Edition)(Clinical) Questions
Step 1
Step 2
Step 3
Step 4
Step 5
(level 1*)
(Level 2* )
(Level 3*)
(Grade 4*)
( et al.
5*)
How common is this disease? (Prevalence)
Local, current random sample survey (or census)
Systematic overview of matching surveys to local context**
Local, non-random sample survey**
>
Case Series**
N/A
Is the diagnostic or monitoring test accurate (diagnosis)
A systematic review of cross-sectional studies that consistently applied reference standards and blind methods
consistently applied reference standards and blinded cross-sectional studies
Non-consecutive case studies, or studies that fail to consistently Apply reference standard**
Case-control study, or poor or non-independent reference standard applied**
< td style="border-top: none; border-left: none; border-bottom: solid black 0.5pt; border-right: solid black 0.5pt">
Mechanism-based reasoning
What would have happened if this treatment had not been added? (prognosis)
A systematic review of starting cohort studies
Starting Queue Study
Control group for cohort study or randomized study**
Case series or case-control studies, or low-quality Prognostic cohort studies**
N/A
Does this treatment work? (Treatment benefits)
A systematic review of randomized trials or single-case randomized controlled trials
randomized trials or observational studies with large effects
Non-randomized controlled cohort/follow-up study**
Case series, case-control studies, or historical control studies**
< span style="font-family:Arial; font-size:12pt">Mechanism-based reasoning
What are the common injuries for this treatment ( Healing Injuries
A systematic review of randomized trials, a nested case-control study
a single randomized trial or (specifically) a view with large effects
Non-randomized controlled cohort/follow-up study (post-marketing surveillance) mention
Case series, case-control studies, or historical control studies
Case series, case-control studies, or historical control studies < span style="font-family:Arial; font-size:12pt">Based on the mechanism of pushing







 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202281.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202281.png" alt=""/>





harm)
Overview, n-of-1 trial for patients with the clinical problem you mentioned, observational study with great effect
Prospective research
for, sufficient numbers to rule out common injuries (long enough follow-up required for long-term injuries)**
Inquiry**
Reasoning
What is this healing rare damage? (treatment injury)
A systematic review of randomized trials or N-of-1 trials
Randomized trials or (specifically) observational studies with large effects
 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202289.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202289.png" alt=""/> < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202291.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202291.png" alt=""/> < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202293.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1015_202293.png" alt=""/>Is this test ( early detection) worth it? ( screening)
A systematic review of randomized studies
Randomized trial
Non-randomized controlled cohort/follow-up study**
Case series, case-control studies, or historical control studies**< /span>
Mechanism-based reasoning
Figure 1 Flow chart of integrated pathological diagnosis of glioma
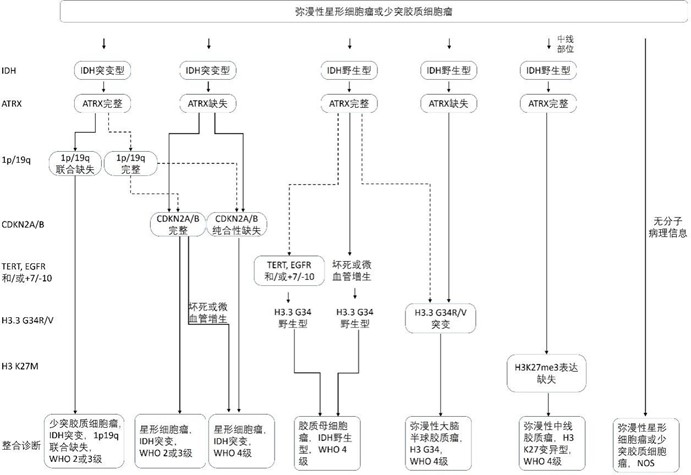
Figure 2 Comprehensive Clinical Process and Recommended Level of Evidence for Glioma
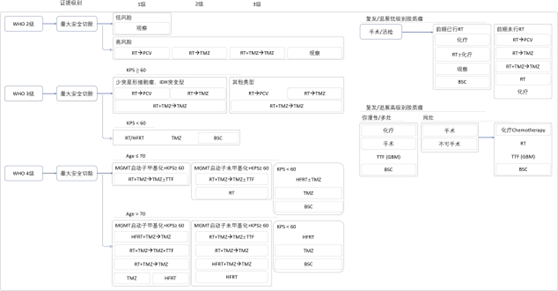
Remarks:RT, radiotherapy; PCV, procarbazine, lomustine and vincristine regimen; TMZ, temozolomide; BSC, best supportive care; HFRT, hypofractionated radiotherapy; KPS, Karnofsky performance status; TTF, tumor-treating fields.
Attachment 3
Glioma Diagnostic and Treatment Guidelines (2022 Edition) Development and Validation Expert Group
Group Leader: Jiang Tao
Deputy Leaders: Wan Jinghai, Qiu Xiaoguang, Mao Ying, Ma Wenbin, Jiang Chuanlu, You Yongping, Kang Dezhi, Li Weiping, Kang Chunsheng, Li Wenbin, and Jiang Zhaoge.
Yunhui Liu, Qing Mao, Yan Qu, Weimin Wang, Lei Wang, Xuejun Yang, Yu Yu, Xinguang Yu, Yongguang Mou, Xinting Wei, Jianning Zhang
Members: Ai Lin, Chen Ling, Chen Qianxue, Chen Ligang, Dou Changwu, Dai Yiwu, Fei Zhou, Feng Hua, Feng Yugong, Hong Tao, Hu Fei, Ji Hongming, and
Ji Nan, Huang Wei, Ji Ying, Li Gang, Li Guilin, Li Liang, Li Shaowu, Li Yunqian, Lin Zhixiong, Liu Xianzhi, Liu Yanhui, Liu Zhixiong, Luo Lin, Lv Zhongqiang, Lv Shengqing, Niu Chaoshi, Pan Yawen, Pang Qi, Chisongtao, Qin Zhiyong, Sheng Xiaofang, Tao Rongjie, Shi Wei, Zhang Junping, Wang Lei, Wang Xiaobian, Wang Maode, Wang Xiaoguang, Wu Jinsong, Wu Anhua, Zhang Jianmin, Zhang Zhiwen, Zhang Zhong, Zhang Wei, Zhao Gang
Co-author: Zhang Wei, Fan Xing, Li Shouwei, Liu Xing, Li Bo, Liu Yanwei, Chen Baoshi, Chai Rui Chao, Chen Xuzhu, Wang Zheng, Li Guanzhang, Wang Yingyan
- style=”margin-left: 42pt”>
- LOUIS D N, PERRY A, WESSELING P, et al. The 2021 WHO Classification of Tumors of the Central Nervous System: a summary [J]. Neuro Oncol, 2021, 23(8): 1231-51.
- JIANG T, MAO Y, MA W, et al. CGCG clinical practice guidelines for the management of adult diffuse gliomas [J]. Cancer Lett, 2016, 375(2): 263-73.
- JIANG T, NAM D H, RAM Z, et al. Clinical practice guidelines for the management of adult diffuse gliomas [J]. Cancer Lett, 2021, 499: 60-72.
-
DUNET V, POMONI A, HOTTINGER A, et al. Performance of 18F-FET versus 18F-FDG- PET for the diagnosis and grading of brain tumors: systematic review and meta-analysis [J]. Neuro Oncol, 2016, 18(3): 426-34.
-
PAFUNDI D H, LAACK N N, YOULAND R S, et al. Biopsy validation of 18F-DOPA PET and biodistribution in gliomas for neurosurgical planning and radiotherapy target delineation: results of a prospective pilot study [J]. Neuro Oncol, 2013, 15(8): 1058-67.
-
WELLER M, VAN DEN BENT M, HOPKINS K, et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma [J]. Lancet Oncol, 2014, 15(9): e395- 403.
-
WEBER D C, CASANOVA N, ZILLI T, et al. Recurrence pattern after [(18)F]fluoroethyltyrosine-positron emission tomography-guided radiotherapy for high-grade glioma: a prospective study [J]. Radiother Oncol, 2009, 93(3): 586-92.
-
MIWA K, MATSUO M, OGAWA S, et al. Re-irradiation of recurrent glioblastoma multiforme using 11C-methionine PET/CT/MRI image fusion for hypofractionated stereotactic radiotherapy by intensity modulated radiation therapy [J]. Radiat Oncol, 2014, 9: 181.
-
TRALINS K S, DOUGLAS J G, STELZER K J, et al. Volumetric analysis of 18F-FDG PET in glioblastoma multiforme: prognostic information and possible role in definition of target volumes in radiation dose escalation [J]. J Nucl Med, 2002, 43(12): 1667-73.
-
MANABE O, HATTORI N, YAMAGUCHI S, et al. Oligodendroglial component complicates the prediction of tumour grading with metabolic imaging [J]. Eur J Nucl Med Mol Imaging, 2015, 42(6): 896-904.
-
JANSEN N L, SCHWARTZ C, GRAUTE V, et al. Prediction of oligodendroglial histology and LOH 1p/19q using dynamic [(18)F]FET-PET imaging in intracranial WHO grade II and III gliomas [J]. Neuro Oncol, 2012, 14(12): 1473-80.
-
HUTTERER M, NOWOSIELSKI M, PUTZER D, et al. [18F]-fluoro-ethyl-L-tyrosine PET: a valuable diagnostic tool in neuro-oncology, but not all that glitters is glioma [J]. Neuro Oncol, 2013, 15(3): 341-51.
-
RAPP M, HEINZEL A, GALLDIKS N, et al. Diagnostic performance of 18F-FET PET in newly diagnosed cerebral lesions suggestive of glioma [J]. J Nucl Med, 2013, 54(2): 229- 35.
-
WEN P Y, MACDONALD D R, REARDON D A, et al. Updated response assessment criteria for high-grade gliomas: response assessment in neuro-oncology working group [J]. J Clin Oncol, 2010, 28(11): 1963-72.
-
BRANDES A A, TOSONI A, FRANCESCHI E, et al. Recurrence pattern after temozolomide concomitant with and adjuvant to radiotherapy in newly diagnosed patients with
glioblastoma: correlation With MGMT promoter methylation status [J]. J Clin Oncol, 2009, 27(8): 1275-9.
- style=”margin-left: 42pt”>
-
WALTER F, CLOUGHESY T, WALTER M A, et al. Impact of 3,4-dihydroxy-6-18F-fluoro- L-phenylalanine PET/CT on managing patients with brain tumors: the referring physician’s perspective [J]. J Nucl Med, 2012, 53(3): 393-8.
-
HERRMANN K, CZERNIN J, CLOUGHESY T, et al. Comparison of visual and semiquantitative analysis of 18F-FDOPA-PET/CT for recurrence detection in glioblastoma patients [J]. Neuro Oncol, 2014, 16(4): 603-9.
-
ALBERT N L, WELLER M, SUCHORSKA B, et al. Response Assessment in Neuro-Oncology working group and European Association for Neuro-Oncology recommendations for the clinical use of PET imaging in gliomas [J]. Neuro Oncol, 2016, 18(9): 1199-208.
-
WELLER M, PFISTER S M, WICK W, et al. Molecular neuro-oncology in clinical practice: a new horizon [J]. Lancet Oncol, 2013, 14(9): e370-9.
-
ECKEL-PASSOW J E, LACHANCE D H, MOLINARO A M, et al. Glioma Groups Based on 1p/19q, IDH, and TERT Promoter Mutations in Tumors [J]. N Engl J Med, 2015, 372(26): 2499-508.
-
CANCER GENOME ATLAS RESEARCH N, BRAT D J, VERHAAK R G, et al. Comprehensive, Integrative Genomic Analysis of Diffuse Lower-Grade Gliomas [J]. N Engl J Med, 2015, 372(26): 2481-98.
-
HU H, MU Q, BAO Z, et al. Mutational Landscape of Secondary Glioblastoma Guides MET-Targeted Trial in Brain Tumor [J]. Cell, 2018, 175(6): 1665-78 e18.
-
Li F, Shi Y, Yao S, et al. Interpretation of the World Health Organization Classification of Tumors of the Central Nervous System (5th edition) for limited astrocytic glioma in 2021 [J]. Chinese Journal of Modern Neurological Diseases, 2021, 21(09): 804-8.
-
DUFFAU H. Is supratotal resection of glioblastoma in noneloquent areas possible? [J]. World Neurosurg, 2014, 82(1-2): e101-3.
-
WU J S, GONG X, SONG Y Y, et al. 3.0-T intraoperative magnetic resonance imaging- guided resection in cerebral glioma surgery: interim analysis of a prospective, randomized, triple-blind, parallel-controlled trial [J]. Neurosurgery, 2014, 61 Suppl 1: 145-54.
-
BELLO L, GAMBINI A, CASTELLANO A, et al. Motor and language DTI Fiber Tracking combined with intraoperative subcortical mapping for surgical removal of gliomas [J]. Neuroimage, 2008, 39(1): 369-82.
-
STUMMER W, PICHLMEIER U, MEINEL T, et al. Fluorescence-guided surgery with 5- aminolevulinic acid for resection of malignant glioma: a randomised controlled multicentre phase III trial [J]. Lancet Oncol, 2006, 7(5): 392-401.
-
ZINN P O, COLEN R R, KASPER E M, et al. Extent of resection and radiotherapy in GBM: A 1973 to 2007 surveillance, epidemiology and end results analysis of 21,783 patients [J]. Int J Oncol, 2013, 42(3): 929-34.
-
KRETH F W, THON N, SIMON M, et al. Gross total but not incomplete resection of glioblastoma prolongs survival in the era of radiochemotherapy [J]. Ann Oncol, 2013, 24(12): 3117-23.
-
LAWS E R, PARNEY I F, HUANG W, et al. Survival following surgery and prognostic factors for recently diagnosed malignant glioma: data from the Glioma Outcomes Project [J]. J Neurosurg, 2003, 99(3): 467-73.
- style=”margin-left: 42pt”>
-
SANAI N, POLLEY M Y, MCDERMOTT M W, et al. An extent of resection threshold for newly diagnosed glioblastomas [J]. J Neurosurg, 2011, 115(1): 3-8.
-
MCGIRT M J, CHAICHANA K L, ATTENELLO F J, et al. Extent of surgical resection is independently associated with survival in patients with hemispheric infiltrating low-grade gliomas [J]. Neurosurgery, 2008, 63(4): Neurosurgery, 2008, 63(4): 700-7; author reply 7-8.
-
Chinese Glioma Collaborative Group (CGCG). Guidelines for the surgical treatment of adult supratentorial low-grade gliomas [J]. Chinese Journal of Neurosurgery, 2016, 32(07): 652-8.
-
MONTEMURRO N, PERRINI P, BLANCO M O, et al. Second surgery for recurrent glioblastoma: A concise overview of the current literature [J]. Clin Neurol Neurosurg, 2016, 142: 60-4.
-
ROBIN A M, LEE I, KALKANIS S N. Reoperation for Recurrent Glioblastoma Multiforme [J]. Neurosurg Clin N Am, 2017, 28(3): 407-28.
-
CHANG E F, CLARK A, SMITH J S, et al. Functional mapping-guided resection of low-grade gliomas in eloquent areas of the brain: improvement of long-term survival. Clinical article [J]. J Neurosurg, 2011, 114(3): 566-73.
-
Jiang T, Wang Y, Fang SN. A comprehensive analysis of the topological properties and protection mechanisms of motor function networks [J]. Chinese Journal of Neurosurgery, 2020, (02): 109-10-11.
-
Zhang Z, Jiang T, Xie J, et al. Arousal anesthesia and intraoperative functional localization for resection of speech area gliomas [J]. Chinese Journal of Neurosurgery, 2007, 23(09): 643-5.
-
Zhang Z, Jiang T, Xie J, et al. Intraoperative functional localization for resection of low-grade gliomas in the supplementary motor area [J]. Chinese Journal of Neurosurgery, 2008, (01): 35-8.
-
Bai H M, Jiang T, Wang W M, et al. Clinical study of category-specific naming area brain localization [J]. Chinese Journal of Neurosurgery, 2010, (12): 1067-70.
-
YORDANOVA Y N, MORITZ-GASSER S, DUFFAU H. Awake surgery for WHO Grade II gliomas within “noneloquent” areas in the left dominant hemisphere: toward a “supratotal” resection. Clinical article [J]. J Neurosurg, 2011, 115(2): J Neurosurg, 2011, 115(2): 232-9.
-
WANG X, WANG Y Y, JIANG T, et al. Direct evidence of the left caudate’s role in bilingual control: an intra-operative electrical stimulation study [J]. Neurocase, 2013, 19(5): 462-9.
-
HERVEY-JUMPER S L, LI J, LAU D, et al. Awake craniotomy to maximize glioma resection: methods and technical nuances over a 27-year period [J]. J Neurosurg, 2015, 123(2): 325-39.
-
JINGSHAN L, SHENGYU F, XING F, et al. Morphometry of the Hand Knob Region and Motor Function Change in Eloquent Area Glioma Patients [J]. Clin Neuroradiol, 2019, 29(2): 243-51.
-
MOLLER M, FREUND M, GREINER C, et al. Real time fMRI: a tool for the routine presurgical localisation of the motor cortex [J]. Eur Radiol, 2005, 15(2): 292-5.
-
XIE J, CHEN X Z, JIANG T, et al. Preoperative blood oxygen level-dependent functional magnetic resonance imaging in patients with gliomas involving the motor cortical areas [J]. Chin Med J (Engl), 2008, 121(7): 631-5.
-
FANG S, LIANG J, QIAN T, et al. Anatomic Location of Tumor Predicts the Accuracy of Motor Function Localization in Diffuse Lower-Grade Gliomas Involving the Hand Knob Area [J]. AJNR Am J Neuroradiol, 2017, 38(10): 1990-7.
-
FANG S, BAI H X, FAN X, et al. A Novel Sequence: ZOOMite-Blood Oxygen Level- Dependent for Motor-Cortex Localization [J]. Neurosurgery, 2020, 86(2): E124-E32.
- style=”margin-left: 42pt”>
-
HALL W A, LIU H, TRUWIT C L. Functional magnetic resonance imaging-guided resection of low-grade gliomas [J]. Surg Neurol, 2005, 64(1): 20-7; discussion 7.
-
QIU T M, YAN C G, TANG W J, et al. Localizing hand motor area using resting-state fMRI: validated with direct cortical stimulation [J]. Acta Neurochir (Wien), 2014, 156(12): 2295- 302.
-
GUNNARSSON T, OLAFSSON E, SIGHVATSSON V, et al. Surgical treatment of patients with low-grade astrocytomas and medically intractable seizures [J]. Acta Neurol Scand, 2002, 105(4): 289-92.
-
FISHER R S, CROSS J H, D’SOUZA C, et al. Instruction manual for the ILAE 2017 operational classification of seizure types [J]. Epilepsia, 2017, 58(4): 531-42.
-
SCHEFFER I E, BERKOVIC S, CAPOVILLA G, et al. ILAE classification of the epilepsies: Position paper of the ILAE Commission for Classification and Terminology [J]. Epilepsia, 2017, 58(4): 512-21.
-
LIANG S, FAN X, ZHAO M, et al. Clinical practice guidelines for the diagnosis and treatment of adult diffuse glioma-related epilepsy [J]. Cancer Med, 2019, 8(10): 4527-35.
-
Technical guidelines for surgical excision of glioma in functional brain areas in the wake state (2018 edition) [J]. Chinese Journal of Microinvasive Neurosurgery, 2018, 23(08): 383-8.
-
DU G, ZHOU L, MAO Y. Neuronavigator-guided glioma surgery [J]. Chin Med J (Engl), 2003, 116(10): 1484-7.
-
Wu Jinsong, Mao Ying, Yao Chengjun, et al. Initial clinical application of intraoperative magnetic resonance imaging neuronavigation for the treatment of glioma (with analysis of 61 cases) [J]. Chinese Journal of Microinvasive Neurosurgery, 2007, (03): 105-9.
-
BELLO L, GALLUCCI M, FAVA M, et al. Intraoperative subcortical language tract mapping guides surgical removal of gliomas involving speech areas [J]. Neurosurgery, 2007, 60(1): 67-80; discussion -2.
-
DUFFAU H. Surgery of low-grade gliomas: towards a ‘functional neurooncology’ [J]. Curr Opin Oncol, 2009, 21(6): 543-9.
-
KIM S S, MCCUTCHEON I E, SUKI D, et al. Awake craniotomy for brain tumors near eloquent cortex: correlation of intraoperative cortical mapping with neurological outcomes in 309 consecutive patients [J]. Neurosurgery, 2009, 64(5): 836-45; discussion 345-6.
-
DE BENEDICTIS A, MORITZ-GASSER S, DUFFAU H. Awake mapping optimizes the extent of resection for low-grade gliomas in eloquent areas [J]. Neurosurgery, 2010, 66(6): 1074-84; discussion 84.
-
TALACCHI A, TURAZZI S, LOCATELLI F, et al. Surgical treatment of high-grade gliomas in motor areas. The impact of different supportive technologies: a 171-patient series [J]. J Neurooncol, 2010, 100(3): 417-26.
-
TATE M C, HERBET G, MORITZ-GASSER S, et al. Probabilistic map of critical functional regions of the human cerebral cortex: Broca’s area revisited [J]. Brain, 2014, 137(Pt 10): 2773-82.
-
DUFFAU H, CAPELLE L, SICHEZ N, et al. Intraoperative mapping of the subcortical language pathways using direct stimulations. An anatomo-functional study [J]. Brain, 2002, 125(Pt 1): 199-214.
-
ROUX F E, DUFOR O, LAUWERS-CANCES V, et al. Electrostimulation mapping of spatial neglect [J]. Neurosurgery, 2011, 69(6): 1218-31.
- style=”margin-left: 42pt”>
-
MAGILL S T, HAN S J, LI J, et al. Resection of primary motor cortex tumors: feasibility and surgical outcomes [J]. J Neurosurg, 2018, 129(4): 961-72.
-
SANAI N, BERGER M S. Glioma extent of resection and its impact on patient outcome [J]. Neurosurgery, 2008, 62(4): 753-64; discussion 264-6.
-
ZHANG Z, JIANG T, XIE J, et al. Surgical strategies for glioma involving language areas [J]. Chin Med J (Engl), 2008, 121(18): 1800-5.
-
LIMA G L O, DEZAMIS E, CORNS R, et al. Surgical resection of incidental diffuse gliomas involving eloquent brain areas. Rationale, functional, epileptological and oncological outcomes [J]. Neurochirurgie, 2017, 63(3): 250-8.
-
JIANG B, CHAICHANA K, VEERAVAGU A, et al. Biopsy versus resection for the management of low-grade gliomas [J]. Cochrane Database Syst Rev, 2017, 4: CD009319.
-
SHAN X, FAN X, LIU X, et al. Clinical characteristics associated with postoperative seizure control in adult low-grade gliomas: a systematic review and meta-analysis [J]. Neuro Oncol, 2018, 20(3): 324-31.
-
ENGLOT D J, HAN S J, BERGER M S, et al. Extent of surgical resection predicts seizure freedom in low-grade temporal lobe brain tumors [J]. Neurosurgery, 2012, 70(4): 921-8; discussion 8.
-
YOU G, SHA Z Y, YAN W, et al. Seizure characteristics and outcomes in 508 Chinese adult patients undergoing primary resection of low-grade gliomas: a clinicopathological study [J]. Neuro Oncol, 2012, 14(2): 230-41.
-
WANG Y Y, ZHANG T, LI S W, et al. Mapping p53 mutations in low-grade glioma: a voxel-based neuroimaging analysis [J]. AJNR Am J Neuroradiol, 2015, 36(1): 70-6.
-
ZAATREH M M, SPENCER D D, THOMPSON J L, et al. Frontal lobe tumoral epilepsy: clinical, neurophysiologic features and predictors of surgical outcome [J]. Epilepsia, 2002, 43(7): 727-33.
-
YAO P S, ZHENG S F, WANG F, et al. Surgery guided with intraoperative electrocorticography in patients with low-grade glioma and refractory seizures [J]. J Neurosurg, 2018, 128(3): 840-5.
-
PEREIRA L C, OLIVEIRA K M, L’ABBATE G L, et al. Outcome of fully awake craniotomy for lesions near the eloquent cortex: analysis of a prospective surgical series of 79 supratentorial primary brain tumors with long follow-up [J]. Acta Neurochir (Wien), 2009, 151(10): 1215-30.
-
LIMA G L, DUFFAU H. Is there a risk of seizures in “preventive” awake surgery for incidental diffuse low-grade gliomas? [J]. J Neurosurg, 2015, 122(6): 1397-405.
-
BOETTO J, BERTRAM L, MOULINIE G, et al. Low Rate of Intraoperative Seizures During Awake Craniotomy in a Prospective Cohort with 374 Supratentorial Brain Lesions: Electrocorticography Is Not Mandatory [J]. World Neurosurg, 2015, 84(6): 1838-44.
-
VECHT C J, KERKHOF M, DURAN-PENA A. Seizure prognosis in brain tumors: new insights and evidence-based management [J]. Oncologist, 2014, 19(7): 751-9.
-
DI BONAVENTURA C, ALBINI M, D’ELIA A, et al. Epileptic seizures heralding a relapse in high grade gliomas [J]. Seizure, 2017, 51: 157-62.
-
KAHLENBERG C A, FADUL C E, ROBERTS D W, et al. Seizure prognosis of patients with low-grade tumors [J]. Seizure, 2012, 21(7): 540-5.
- SUN M Z, OH T, IVAN M E, et al. Survival impact of time to initiation of
chemoradiotherapy after resection of newly diagnosed glioblastoma [J]. J Neurosurg, 2015, 122(5): 1144-50.
- style=”margin-left: 42pt”>
-
MERCHANT T E, KUN L E, WU S, et al. Phase II trial of conformal radiation therapy for pediatric low-grade glioma [J]. J Clin Oncol, 2009, 27(22): 3598-604.
-
CABRERA A R, KIRKPATRICK J P, FIVEASH J B, et al. Radiation therapy for glioblastoma: Executive summary of an American Society for Radiation Oncology Evidence-Based Clinical Practice Guideline [J]. Pract Radiat Oncol, 2016, 6(4): 217-25.
-
CHANG E L, AKYUREK S, AVALOS T, et al. Evaluation of peritumoral edema in the delineation of radiotherapy clinical target volumes for glioblastoma [J]. Int J Radiat Oncol Biol Phys, 2007, 68(1): 144-50.
-
GILBERT M R, WANG M, ALDAPE K D, et al. Dose-dense temozolomide for newly diagnosed glioblastoma: a randomized phase III clinical trial [J]. J Clin Oncol, 2013, 31(32): 4085-91.
-
STUPP R, MASON W P, VAN DEN BENT M J, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma [J]. N Engl J Med, 2005, 352(10): 987-96.
-
HEGI M E, DISERENS A C, GORLIA T, et al. MGMT gene silencing and benefit from temozolomide in glioblastoma [J]. N Engl J Med, 2005, 352(10): 997-1003.
-
VAN DEN BENT M J, BRANDES A A, TAPHOORN M J, et al. Adjuvant procarbazine, lomustine, and vincristine chemotherapy in newly diagnosed anaplastic oligodendroglioma: long-term follow-up of EORTC brain tumor group study 26951 [J]. J Clin Oncol, 2013, 31(3): 344-50.
-
CAIRNCROSS G, WANG M, SHAW E, et al. Phase III trial of chemoradiotherapy for anaplastic oligodendroglioma: long-term results of RTOG 9402 [J]. J Clin Oncol, 2013, 31(3): 337-43.
-
INTERGROUP RADIATION THERAPY ONCOLOGY GROUP T, CAIRNCROSS G, BERKEY B, et al. Phase III trial of chemotherapy plus radiotherapy compared with radiotherapy alone for pure and mixed anaplastic oligodendroglioma: Intergroup Radiation Therapy Oncology Group Trial 9402 [J]. J Clin Oncol, 2006, 24(18): 2707-14.
-
YANG P, CAI J, YAN W, et al. Classification based on mutations of TERT promoter and IDH characterizes subtypes in grade II/III gliomas [J]. Neuro Oncol, 2016, 18(8): 1099- 108.
-
DANIELS T B, BROWN P D, FELTEN S J, et al. Validation of EORTC prognostic factors for adults with low-grade glioma: a report using intergroup 86-72-51 [J]. Int J Radiat Oncol Biol Phys, 2011, 81(1): 218-24.
-
NABORS L B, PORTNOW J, AMMIRATI M, et al. NCCN Guidelines Insights: Central Nervous System Cancers, Version 1.2017 [J]. J Natl Compr Canc Netw, 2017, 15(11): 1331-45.
-
SHAW E G, BERKEY B, COONS S W, et al. Recurrence following neurosurgeon- determined gross-total resection of adult supratentorial low-grade glioma: results of a prospective clinical trial [J]. J Neurosurg, 2008, 109(5): 835-41.
-
SHAW E, ARUSELL R, SCHEITHAUER B, et al. Prospective randomized trial of low- versus high-dose radiation therapy in adults with supratentorial low-grade glioma: initial report of a North Central Cancer Treatment Group/Radiation Therapy Oncology Group/Eastern Cooperative Oncology Group study [J]. J Clin Oncol, 2002, 20(9): 2267-76.
- style=”margin-left: 42pt”>
-
LIU Y, LI Y, WANG P, et al. High-dose radiotherapy in newly diagnosed low-grade gliomas with nonmethylated O(6)-methylguanine-DNA methyltransferase [J]. Radiat Oncol, 2021, 16(1): 157.
-
LIU Y, LIU S, LI G, et al. Association of high-dose radiotherapy with improved survival in patients with newly diagnosed low-grade gliomas [J]. Cancer, 2021.
-
KLEIN M, HEIMANS J J, AARONSON N K, et al. Effect of radiotherapy and other treatment-related factors on mid-term to long-term cognitive sequelae in low-grade gliomas: a comparative study [J]. Lancet, 2002, 360(9343): 1361-8.
-
RODRIGUEZ D, CHEUNG M C, HOUSRI N, et al. Outcomes of malignant CNS ependymomas: an examination of 2408 cases through the Surveillance, Epidemiology, and End Results (SEER) database (1973-2005) [J]. J Surg Res, 2009, 156(2): 340-51.
-
MERCHANT T E, LI C, XIONG X, et al. Conformal radiotherapy after surgery for paediatric ependymoma: a prospective study [J]. Lancet Oncol, 2009, 10(3): 258-66.
-
Zhou Liangfu, Mao Ying, Wang Renzhi. Guidelines for the diagnosis and treatment of glioma of the central nervous system in China (2015) [J]. Chinese Medical Journal, 2016, 96(07): 485-509.
-
FOGH S E, ANDREWS D W, GLASS J, et al. Hypofractionated stereotactic radiation therapy: an effective therapy for recurrent high-grade gliomas [J]. J Clin Oncol, 2010, 28(18): 3048-53.
-
CABRERA A R, CUNEO K C, DESJARDINS A, et al. Concurrent stereotactic radiosurgery and bevacizumab in recurrent malignant gliomas: a prospective trial [J]. Int J Radiat Oncol Biol Phys, 2013, 86(5): 873-9.
-
LAWRENCE Y R, LI X A, EL NAQA I, et al. Radiation dose-volume effects in the brain [J]. Int J Radiat Oncol Biol Phys, 2010, 76(3 Suppl): S20-7.
-
BOOTHE D, YOUNG R, YAMADA Y, et al. Bevacizumab as a treatment for radiation necrosis of brain metastases post stereotactic radiosurgery [J]. Neuro Oncol, 2013, 15(9): 1257-63.
-
MINNITI G, AGOLLI L, FALCO T, et al. Hypofractionated stereotactic radiotherapy in combination with bevacizumab or fotemustine for patients with progressive malignant gliomas [J]. J Neurooncol, 2015, 122(3): 559-66.
-
DOUW L, KLEIN M, FAGEL S S, et al. Cognitive and radiological effects of radiotherapy in patients with low-grade glioma: long-term follow-up [J]. Lancet Neurol, 2009, 8(9): 810- 8.
-
POSTMA T J, KLEIN M, VERSTAPPEN C C, et al. Radiotherapy-induced cerebral abnormalities in patients with low-grade glioma [J]. Neurology, 2002, 59(1): Neurology, 2002, 59(1): 121-3.
-
STUPP R, HEGI M E, MASON W P, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial [J]. Lancet Oncol, 2009, 10(5): 459-66.
-
WOLFF J E, BERRAK S, KOONTZ WEBB S E, et al. Nitrosourea efficacy in high-grade glioma: a survival gain analysis summarizing 504 cohorts with 24193 patients [J]. J Neurooncol, 2008, 88(1): 57-63.
-
VAN DEN BENT M J, BAUMERT B, ERRIDGE S C, et al. Interim results from the CATNON trial (EORTC study 26053-22054) of treatment with concurrent and adjuvant temozolomide for 1p/19q non-co-deleted anaplastic glioma: a phase 3, randomised,
open-label intergroup study [J]. Lancet, 2017, 390(10103): 1645-53.
- style=”margin-left: 42pt”>
-
VAN DEN BENT M J, TESILEANU C M S, WICK W, et al. Adjuvant and concurrent temozolomide for 1p/19q non-co-deleted anaplastic glioma (CATNON; EORTC study 26053-22054): second interim analysis of a randomised, open-label, phase 3 study [J]. Lancet Oncol, 2021, 22(6): 813-23.
-
MALMSTROM A, GRONBERG B H, MAROSI C, et al. Temozolomide versus standard 6-week radiotherapy versus hypofractionated radiotherapy in patients older than 60 years with glioblastoma: the Nordic randomised, phase 3 trial [J]. Lancet Oncol, 2012, 13(9): 916-26.
-
HERRLINGER U, TZARIDIS T, MACK F, et al. Lomustine-temozolomide combination therapy versus standard temozolomide therapy in patients with newly diagnosed glioblastoma with methylated MGMT promoter (CeTeG/NOA-09): a randomised, open- label, phase 3 trial [J]. Lancet, 2019, 393(10172): 678-88.
-
BELL E H, ZHANG P, SHAW E G, et al. Comprehensive Genomic Analysis in NRG Oncology/RTOG 9802: A Phase III Trial of Radiation Versus Radiation Plus Procarbazine, Lomustine (CCNU), and Vincristine in High-Risk Low-Grade Glioma [J]. J Clin Oncol, 2020, 38(29): 3407-17.
-
FISHER B J, PUGH S L, MACDONALD D R, et al. Phase 2 Study of a Temozolomide- Based Chemoradiation Therapy Regimen for High-Risk, Low-Grade Gliomas: Long-Term Results of Radiation Therapy Oncology Group 0424 [J]. Int J Radiat Oncol Biol Phys, 2020, 107(4): 720-5.
-
SHAW E G, WANG M, COONS S W, et al. Randomized trial of radiation therapy plus procarbazine, lomustine, and vincristine chemotherapy for supratentorial adult low-grade glioma: initial results of RTOG 9802 [J]. J Clin Oncol, 2012, 30(25): 3065-70.
-
KESARI S, SCHIFF D, DRAPPATZ J, et al. Phase II study of protracted daily temozolomide for low-grade gliomas in adults [J]. Clin Cancer Res, 2009, 15(1): 330-7.
-
TRIEBELS V H, TAPHOORN M J, BRANDES A A, et al. Salvage PCV chemotherapy for temozolomide-resistant oligodendrogliomas [J]. Neurology, 2004, 63(5): 904-6.
-
MASSIMINO M, SPREAFICO F, RIVA D, et al. A lower-dose, lower-toxicity cisplatin- etoposide regimen for childhood progressive low-grade glioma [J]. J Neurooncol, 2010, 100(1): 65-71.
-
PERRY J R, BELANGER K, MASON W P, et al. Phase II trial of continuous dose-intense temozolomide in recurrent malignant glioma: RESCUE study [J]. J Clin Oncol, 2010, 28(12): 2051-7.
-
WICK W, PUDUVALLI V K, CHAMBERLAIN M C, et al. Phase III study of enzastaurin compared with lomustine in the treatment of recurrent intracranial glioblastoma [J]. J Clin Oncol, 2010, 28(7): 1168-74.
-
NORDEN A D, YOUNG G S, SETAYESH K, et al. Bevacizumab for recurrent malignant gliomas: efficacy, toxicity, and patterns of recurrence [J]. Neurology, 2008, 70(10): 779- 87.
-
FULTON D, URTASUN R, FORSYTH P. Phase II study of prolonged oral therapy with etoposide (VP16) for patients with recurrent malignant glioma [J]. J Neurooncol, 1996, 27(2): 149-55.
- FRIEDMAN H S, PRADOS M D, WEN P Y, et al. Bevacizumab alone and in combination
with irinotecan in recurrent glioblastoma [J]. J Clin Oncol, 2009, 27(28): 4733-40.
- style=”margin-left: 42pt”>
-
YUNG W K, ALBRIGHT R E, OLSON J, et al. A phase II study of temozolomide vs. procarbazine in patients with glioblastoma multiforme at first relapse [J]. Br J Cancer, 2000, 83(5): 588-93.
-
LOMBARDI G, DE SALVO G L, BRANDES A A, et al. Regorafenib compared with lomustine in patients with relapsed glioblastoma (REGOMA): a multicentre, open-label, randomised, controlled, phase 2 trial [J]. Lancet Oncol, 2019, 20(1): 110-9.
-
STUPP R, TAILLIBERT S, KANNER A A, et al. Maintenance Therapy With Tumor-Treating Fields Plus Temozolomide vs Temozolomide Alone for Glioblastoma: A Randomized Clinical Trial [J]. JAMA, 2015, 314(23): 2535-43.
-
FERGUSON S D, XIU J, WEATHERS S P, et al. GBM-associated mutations and altered protein expression are more common in young patients [J]. Oncotarget, 2016, 7(43): 69466-78.
-
SRIVIDYA M R, THOTA B, ARIVAZHAGAN A, et al. Age-dependent prognostic effects of EGFR/p53 alterations in glioblastoma: study on a prospective cohort of 140 uniformly treated adult patients [J]. J Clin Pathol, 2010, 63(8): 687-91.
-
VUORINEN V, HINKKA S, FARKKILA M, et al. Debulking or biopsy of malignant glioma in elderly people – a randomised study [J]. Acta Neurochir (Wien), 2003, 145(1): 5-10.
-
ALMENAWER S A, BADHIWALA J H, ALHAZZANI W, et al. Biopsy versus partial versus gross total resection in older patients with high-grade glioma: a systematic review and meta-analysis [J]. Neuro Oncol, 2015, 17(6): 868-81.
-
EXTERMANN M, HURRIA A. Comprehensive geriatric assessment for older patients with cancer [J]. J Clin Oncol, 2007, 25(14): 1824-31.
-
PERRY J R, LAPERRIERE N, O’CALLAGHAN C J, et al. Short-Course Radiation plus Temozolomide in Elderly Patients with Glioblastoma [J]. N Engl J Med, 2017, 376(11): 1027-37.
-
RINEER J, SCHREIBER D, CHOI K, et al. Characterization and outcomes of infratentorial malignant glioma: a population-based study using the Surveillance Epidemiology and End-Results database [J]. Radiother Oncol, 2010, 95(3): 321-6.
-
SCHWARTZENTRUBER J, KORSHUNOV A, LIU X Y, et al. Driver mutations in histone H3.3 and chromatin remodelling genes in paediatric glioblastoma [J]. Nature, 2012, 482(7384): 226-31.
-
BECHET D, GIELEN G G, KORSHUNOV A, et al. Specific detection of methionine 27 mutation in histone 3 variants (H3K27M) in fixed tissue from high-grade astrocytomas [J]. Acta Neuropathol, 2014, 128(5): 733-41.
-
CARAI A, MASTRONUZZI A, DE BENEDICTIS A, et al. Robot-Assisted Stereotactic Biopsy of Diffuse Intrinsic Pontine Glioma: A Single-Center Experience [J]. World Neurosurg, 2017, 101: 584-8.
-
HAMISCH C, KICKINGEREDER P, FISCHER M, et al. Update on the diagnostic value and safety of stereotactic biopsy for pediatric brainstem tumors: a systematic review and meta-analysis of 735 cases [J]. J Neurosurg Pediatr, 2017, 20(3): 261-8.
-
COHEN K J, HEIDEMAN R L, ZHOU T, et al. Temozolomide in the treatment of children with newly diagnosed diffuse intrinsic pontine gliomas: a report from the Children’s Oncology Group [J]. Neuro Oncol, 2011, 13(4): 410-6.
- style=”margin-left: 42pt”>
-
FLEISCHHACK G, MASSIMINO M, WARMUTH-METZ M, et al. Nimotuzumab and radiotherapy for treatment of newly diagnosed diffuse intrinsic pontine glioma (DIPG): a phase III clinical study [J]. J Neurooncol, 2019, 143(1): 107-13.
-
PACE A, DIRVEN L, KOEKKOEK J A F, et al. European Association for Neuro-Oncology (EANO) guidelines for palliative care in adults with glioma [J]. Lancet Oncol, 2017, 18(6): e330-e40.
-
Wang Citation, Fang Shengyu, Li Lianwang, et al. Clinical analysis of repetitive transcranial magnetic stimulation for postoperative motor dysfunction in glioma (with five case reports) [J]. Chinese Journal of Neurosurgery, 2020, 36(05): 458-62.
- style=”margin-left: 41pt”>
-
Chinese Expert Consensus on Multidisciplinary Diagnosis and Treatment (MDT) of Glioma [J]. Chinese Journal of Neurosurgery, 2018, 34(02): 113-8.
-