Guidelines for the diagnosis and treatment of melanoma
(2022 Edition)
I. Overview
Although melanoma is a rare malignancy in China, the death rate is high and the incidence is increasing year by year. Melanoma in China differs greatly from Caucasians in Europe and the United States in terms of pathogenesis, biological behavior, histological morphology, treatment methods, and prognosis. Among Asians and other people of color, primary melanoma in the extremities accounts for about 50%, with common primary sites mostly in the extremities such as the soles of the feet, toes, finger ends, and under the nails, and primary melanoma in the mucous membranes such as the rectum, anus, vulva, eyes, and oropharynx Melanoma in the mucosa, such as the rectum, anus, vulva, eyes, and oropharynx, accounts for 20% to 30%; and for Caucasians, melanoma originating in the skin accounts for about 30%. span style=”font-family:Times New Roman”>90% of melanomas with primary sites on the back, chest and abdomen, and skin of the lower extremities; melanomas on the extremities and mucous membranes accounted for only 5%, 1%.
II. Screening and diagnosis
(I) Surveillance screening of high-risk groups.
Screening of people at high risk for melanoma helps with early detection, early diagnosis, and early treatment, and is also key to improving the outcome of melanoma. In China, people at high risk for cutaneous melanoma include those with a history of severe sunburn, a history of skin cancer, pigmented nevi, chronic inflammation of the skin at the extremities, and inappropriate treatments such as salt pickling, cutting, needle picking, and string strangulation. The risk factors for mucosal melanoma are unclear. Recommendations
Recommend that people at high risk should regularly self-examine and, if necessary, visit a specialist hospital, rather than treating themselves.
(ii) Diagnosis of melanoma.
Melanoma is most likely to occur in the skin, so visual diagnosis is the easiest means of early diagnosis. Visual inspection and palpation of the primary lesion, affected areas, and regional lymph nodes are commonly used in the initial diagnosis of melanoma.
- style=”margin-left: 55pt”>
- Clinical symptoms
Dermal melanoma mostly develops from moles, and the early malignant symptoms of moles can be summarized as the following ABCDE law.
-
Asymmetric (asymmetry): one half of the pigmented spot looks asymmetrical to the other half.
-
Irregular margins () border irregularity): The edges are irregular or have cut marks, jagged teeth, etc., unlike normal pigmented nevi that have smooth round or oval contours. Ccolor variationcolor variation): normal pigmented nevi are usually monochromatic.
Melanoma, on the other hand, mainly appears as a smudgy black color, but can also be brown, tan, brown-black, blue, pink, black, or even white in many different colors.
-
diameter (diameter): pigmented nevus diameter >5 ~6mm or when the pigmented nevus is significantly larger to Note that melanomas are usually larger than normal moles and a biopsy evaluation is advisable for pigmented moles >1cm in diameter.
-
augmentation (< span style="font-family:Times New Roman">elevation): In some early melanomas, there is a slight elevation of the entire tumor body.
Likewise, the general clinical features of subxiphoid melanoma are ABCDEF Method
then the meanings are:A represents older adults or seniors (age), Asian and African-American good hair (Asian or African-American race); B represents longitudinal black nail strips ranging in color from brown to black and >3mm in width Roman”>3mm (brown to black); C represents nail change or lack of improvement of the diseased nail with adequate treatment
(change); D represents the order of most frequent involvement at the end of the finger/ toe, in order of thumb > lesser toe > index finger, with a single finger/ Roman”>/ toe involvement > multifidus / toe involvement (digit); E represents lesion extension (extension); F represents a personal or family history of dysplastic nevi and melanoma (family history).
ABCDE(F) ) The only shortcoming of the rule is that it does not take into account the speed of melanoma progression, such as the tendency for significant changes to occur within weeks or months. The application of dermoscopy, which can compensate for the lack of visual observation while detecting and comparing changes in suspected melanoma, can significantly improve the accuracy of early diagnosis of melanoma. Further development of melanoma may present with satellite foci, ulcers, recurrent non-healing, regional lymph node metastases and metastases. Symptoms of advanced melanoma vary depending on the site of metastasis, and the sites prone to metastasis are lung, liver, bone and brain. Melanoma of ocular and rectal origin is prone to liver metastases.
- style=”margin-left: 55pt”>
- Imaging Diagnosis
Imaging should be decided according to the local situation and the patient’s financial situation. Mandatory investigations include ultrasound of regional lymph nodes (neck, axilla, groin, popliteal fossa, etc.), chest CT, abdominopelvic ultrasound. Enhanced CT or MRI, whole-body bone scan and cranial enhancement MRI or CT examinations. Imaging is useful to determine if the patient has distant metastases, as well as to assist in preoperative evaluation (including X ray, ultrasound, etc.). If the primary focus
invasion is deep, local CT, MRI. Whole-body positron emission computed tomography (positron emission tomography-computed tomography, , PET-CT) examination, especially in patients with unknown primary foci. Positron emission tomography (positron emission tomography, PET) is an easier way to detect subclinical metastases. Most examiners consider PET to be insensitive and of low benefit in detecting metastatic lesions in early stage limited melanoma. For stage III patients, PET-CT scans are more useful and can help identify Lesions that cannot be clearly diagnosed by CT and areas that cannot be visualized by conventional CT scans (e.g., extremities). PET-CT has advantages over regular CT in detecting distant lesions.
-
Ultrasound: Ultrasound is the most commonly used imaging test in clinical practice because it is easy to perform, flexible and intuitive, and noninvasive and portable. Ultrasonography is the most common imaging method in clinical practice because of its easy operation, flexibility and intuitiveness, non-invasive and portable features. Ultrasound examination of melanoma is mainly used to determine the nature of regional lymph nodes and subcutaneous nodules, and to provide important information for clinical treatment selection and surgical planning. Real-time ultrasonography can reveal hemodynamic changes in metastases and is particularly advantageous in helping to identify and diagnose small liver metastases and lymph node metastases.
- CT. Conventional scanning+enhanced scanning (commonly iodine contrast) is used . At present, in addition to clinical diagnosis and staging of melanoma, it is also often used in the evaluation of melanoma efficacy, tumor volume measurement, and evaluation of metastasis in other organs such as lung and bone, and is widely used clinically.
- MRI: Conventional use of plain+enhanced scanning (commonly used contrast agent gadopentetate glucosamine) due to its radiation-free effect, high tissue resolution, and It can be multifaceted
Multi-site, multi-sequence parametric imaging with morphology binding capabilities (including diffusion-weighted imaging, perfusion-weighted imaging, and spectral analysis) is a comprehensive imaging technology capability for the clinical diagnosis and efficacy of melanoma. The results of this study are summarized below.
-
PET-CT:Fluorine-18-Fluorodeoxyglucose PET-CT The advantages of whole-body imaging are: 1) staging of tumors by 1 examination can comprehensively evaluate lymph node metastasis and distant organ metastasis; ② restaging, as PET functional images are not affected by anatomical structures, and can accurately show recurrent metastases after anatomical changes or in areas with complex anatomical structures; (iii) efficacy evaluation, which is more sensitive and accurate for targeted drugs that inhibit tumor activity; (iv) guidance outlining of biological target areas for radiotherapy and puncture biopsy of active areas of tumor lesions; ⑤ evaluation of tumor malignancy and prognosis. Conventional CT is less sensitive for the diagnosis of cutaneous or subcutaneous metastases, while PET-CT can compensate for this.
- style=”margin-left: 44pt”>
- Laboratory Tests
Blood workup, liver and kidney function, and lactate dehydrogenase, which are used primarily to prepare for subsequent treatment and to understand the prognosis. Although lactate dehydrogenase is not a sensitive indicator for detecting metastasis, it can guide prognosis. There are no specific serum tumor markers for melanoma, and tumor marker testing is not currently recommended.
- style=”margin-left: 44pt”>
- Focal biopsy
Biopsies for cutaneous melanoma include excisional biopsy, excisional biopsy, and circumferential biopsy, and chipping and puncture biopsy are generally not performed. For patients with melanoma that is initially judged to have no distant metastases, biopsy generally recommends a complete excisional biopsy with a margin of 0.3 to 0.5 cm , the incision should be made in the direction of the dermatoglyphic line (e.g. the limb is usually chosen to be cut along the long axis)
- Laboratory Tests
mouth), and puncture biopsy or partial excision is not recommended. Partial excisional biopsies are not conducive to histologic diagnosis and thickness measurement, increasing the risk of misdiagnosis and incorrect staging. Excisional biopsy and ring-drill biopsy are generally only used for diagnostic biopsy of large lesions or specific sites, such as lesions on the face, palms, soles, ears, fingers, toes, or under the nail, or huge lesions where complete excisional biopsy is not possible.
(iii) Pathologic diagnosis of melanoma.
- style=”margin-left: 63pt”>
- Pathologic Diagnostic Criteria for Melanoma
Histopathology is the primary tool for confirming the diagnosis of melanoma, and immunohistochemical staining is the primary adjunct for identifying melanoma. The diagnosis of melanoma is made by pathologic histology, regardless of whether it is a superficial lesion or a biopsy of a metastasis or surgically excised tissue specimen. The pathologic diagnosis must be combined with clinical evidence and a thorough understanding of the patient’s medical history and imaging studies.
- style=”margin-left: 63pt”>
- Guidelines for pathologic diagnosis of melanoma
The pathological diagnosis guidelines for melanoma consist of specimen handling, specimen sampling, pathological examination and pathological report.
-
Key points of specimen handling: ①The surgeon should provide the focal characteristics of the tissue sent for examination (ulceration< /Nodules/chromatophores), with dye staining or sutures to mark surgical margins and important lesions; ②larger specimens must be spaced 3mm apart fixed by left and right incisions; ③10%neutral buffered formalin (formaldehyde content 4%) fixation 6~48hours.
- style=”margin-left: 72pt”>
-
Specimen taking points: paint the cut edge with pigment. Vertical skin surface to 2~
-
 3mm >Separate the specimens in parallel and measure the tumor thickness and depth of infiltration. The sampling method is selected according to clinical requirements, specimen type and size, and the distance between the lesion and the incision margin; the thickest lesion, deepest infiltrate, and ulcer must be sampled. The skin between the main tumor and satellite foci must be sampled to clarify the relationship between the two. For tumors smaller than 2 cm , all of them should be taken, and those 3 cm or more should be taken according to 2 cm . family:Times New Roman”>1 block /5mm was taken. There are two methods of margin sampling, namely, vertical margin radial sampling and parallel margin dissection sampling, the latter of which cannot determine the distance between the negative margin and the tumor, and it is recommended that vertical margin radial sampling be used as much as possible to help histologically determine the distance between the negative margin and the tumor (Figure 1). span>). Only 1 block of skin tissue can be placed in an embedding cassette. The embedding should ensure that the section shows the structural level of the skin, mucosa, etc. at the site of tumorigenesis to ensure histology for T staging.
3mm >Separate the specimens in parallel and measure the tumor thickness and depth of infiltration. The sampling method is selected according to clinical requirements, specimen type and size, and the distance between the lesion and the incision margin; the thickest lesion, deepest infiltrate, and ulcer must be sampled. The skin between the main tumor and satellite foci must be sampled to clarify the relationship between the two. For tumors smaller than 2 cm , all of them should be taken, and those 3 cm or more should be taken according to 2 cm . family:Times New Roman”>1 block /5mm was taken. There are two methods of margin sampling, namely, vertical margin radial sampling and parallel margin dissection sampling, the latter of which cannot determine the distance between the negative margin and the tumor, and it is recommended that vertical margin radial sampling be used as much as possible to help histologically determine the distance between the negative margin and the tumor (Figure 1). span>). Only 1 block of skin tissue can be placed in an embedding cassette. The embedding should ensure that the section shows the structural level of the skin, mucosa, etc. at the site of tumorigenesis to ensure histology for T staging.
Figure 1. Dermal melanoma cut edge retrieval method: ①Radiographic retrieval of vertical cut edge.
2. Parallel marginal dissection retrieval
- style=”margin-left: 83pt”>
- Key points of pathological description.
1) Gross specimen description: Place the specimen according to the anatomical position provided by the clinic, observe and describe the size, shape and color of the tumor. Skin tumors must be described with or without surface
ulceration, the presence of surrounding satellite metastases, and the number and size of satellite metastases and their spacing from the main tumor nodes.
② Microscopic description: The diagnosis of melanoma is based on the WHO 2010 edition, focusing on the following The most common four histologic types are superficially disseminated, malignant freckle, acral freckle, and nodular; rare histologic types include pro-connective tissue proliferative melanoma, and melanoma of blue nevus origin. Melanoma of blue nevus origin, melanoma of giant congenital nevus origin, childhood melanoma, and nevus-like melanoma; depth of infiltration of melanoma: quantitative by Breslow thickness in millimeters, qualitative by Breslow thickness in millimeters. =”font-family:Times New Roman”>Clark level grading, describing the level of skin infiltrated; other prognostic indicators: including ulceration, vascular invasion, microsatellite foci, mitotic rate, etc.
Breslow thickness: refers to the tumor thickness of cutaneous melanoma, which is T basic indicator of staging. Non-ulcerated lesions refer to the vertical distance from the granular layer of the epidermis to the deepest part of the tumor infiltration; ulcerated lesions refer to the vertical distance from the base of the ulcer to the deepest part of the tumor infiltration. Clark level grading: refers to the depth of cutaneous melanoma infiltration and is classified as 5 levels. Grade 1 indicates that the tumor is confined to the epidermis (melanoma in situ); Grade 2 indicates that the tumor infiltrates the dermal papillae but has not Grade 3 indicates that the tumor cells have infiltrated the dermal papillary layer and reached the junction of the papillary and reticular layers; Grade 4 indicates that the tumor has infiltrated the dermal reticular layer indicates tumor infiltration of the dermal reticular layer; Grade 5 indicates tumor infiltration of the subcutaneous tissue.
③Immunohistochemistry: Melanoma has a variety of tumor cell morphologies, especially anaplastic lesions, and often needs to be differentiated from a variety of tumors such as carcinoma, sarcoma, and lymphoma. Commonly used characteristic markers of melanocytes include S-100, Sox-10, and
Melan-A, Melan-A, Melan-A, Melan-A. /span>, HMB45, Tyrosinase, MITF, etc. Among them, S-100 is the most sensitive and is a screening indicator for melanoma; however, its specificity is poor and it cannot be used as a definitive indicator for melanoma in general. Melan-A, HMB45 and Tyrosinase are more specific, but tumorigenic melanocytes can show abnormal expression with varying sensitivity, so it is recommended that both 2~ be used when differential diagnosis is needed. 3 of these markers, plus S-100, are recommended to improve the detection rate of melanoma.
④Specific types of melanoma: mucosal melanoma: generally infiltrative lesions that can be accompanied by intraepithelial Paget-like dissemination in the mucosa. The tumor cells may be epithelioid, spindle-shaped, plasma cell-like, balloon-like, etc., with or without pigmentation, and often require immunohistochemical staining with the aid of characteristic melanocyte markers for diagnosis; uveal melanoma: according to cell morphology, it is classified into spindle cell type, epithelioid cell type and mixed type. Cell type is an independent predictor of the risk of uveal melanoma metastasis, with the best prognosis for the spindle cell type and the worst prognosis for the epithelioid cell type.
- style=”margin-left: 67pt”>
- Report of pathological diagnosis of melanoma
For hospitals that are able to do so, routine pathological histology reports of primary cutaneous melanoma may be recommended to include: tumor site, specimen type, tumor size or extent, histological type, Breslow >thickness, presence or absence of ulceration, depth of infiltration (Clark level grading), splitting activity, status of cut margins (including the distance of each cut margin from the tumor and the histological type of the cut margin lesion), presence or absence of microsatellite metastases or satellite metastases, presence or absence of intraventricular tumor thrombi, and The presence or absence of nerve invasion (Table 2). The total number of lymph nodes detected, the number of metastatic lymph nodes, and the presence of extra-membranous involvement of lymph nodes should be reported for sentinel lymph nodes and regional lymph nodes. Recommendations for molecular testing related to targeted therapy include at least
BRAF, CKIT and NRAS are driver genes. The frozen section technique is not recommended for intraoperative pathologic diagnosis. In cases of diagnostic difficulties, it is recommended to refer to multiple hospitals for consultation.
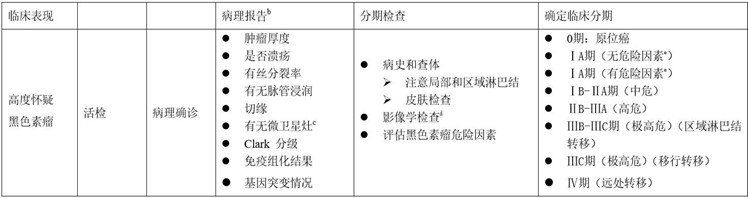
(iv) Clinical diagnostic criteria and roadmap for melanoma.
Melanoma is mainly diagnosed by clinical symptoms and pathology, combined with whole-body imaging to obtain complete staging (Appendix I).
III. Staging
The staging of melanoma is critical to the assessment of prognosis and the selection of a rational treatment plan. Different sites of melanoma use different pTNM staging indicators, and the pTNM staging of cutaneous melanoma is shown in Appendix Second, the scope of application includes: lips, eyelids, outer ear, other parts of the face, scalp and neck skin, trunk, upper extremities and shoulders, lower extremities and buttocks, skin spanning lesions, skin, labia majora, labia minora, clitoris, vulva spanning lesions, vulva, prepuce, glans, penis body, penis spanning lesions, penis, scrotum. Mucosal melanoma of the head and neck pTNM See Appendix III for staging for: nasal cavity, sinuses, oral cavity, oropharynx, nasopharynx, larynx, and hypopharynx. Ocular melanoma: There are different pTNM stages for ocular iris melanoma, ciliary body choroidal melanoma, and conjunctival melanoma, respectively, as described in
The AJCC Tumor Staging Manual ( 2016 th 8th edition) in the relevant section, see Appendix IV. There is no pTNM staging for the digestive tract (esophagus, small intestine, and large intestine) at this time. According to our clinical guidelines for the management of melanoma, it is recommended to describe the level of tumor infiltration into the GI tract. There is no pTNM staging for vagina at this time, and cervical melanoma pTNM staging refers to cervical cancer. Meningeal melanoma pTNM staging is the same as other meningeal tumors.
IV.
Because melanoma treatment involves multiple approaches and multiple disciplines, melanoma treatment must focus on a multidisciplinary team model, thus avoiding the limitations of single-discipline treatment, providing one-stop medical services, promoting interdisciplinary communication, and facilitating the establishment of a medical center. It is therefore important to focus on the multidisciplinary team model to avoid the limitations of single-disciplinary treatment, to provide one-stop medical services, to promote disciplinary communication, and to promote treatment principles and guidelines based on multidisciplinary consensus. The choice of appropriate treatment requires high-level evidence-based support, but also requires consideration of regional and economic disparities.
(i) Surgery and postoperative adjuvant therapy.
- style=”margin-left: 57pt”>
- Extended resection
Early-stage melanoma should be biopsy-confirmed with an expanded resection of the primary site as soon as possible. The safe margins of extended resection are based on the depth of tumor infiltration in the pathology report
(Breslow thickness) to determine: (Breslow thickness) family:Times New Roman”>1) for lesion thickness ≤1.0mm , the safe cutting edge is 0.5. Roman”>0.5 to 1cm; (2) thickness in 1cm; (2) thickness in =”font-family:Times New Roman”>1.01 to 2mm, the safety cutting edge is 1.01 to 2mm. Roman”>1 to 2cm; (3) thickness in 2.01 to 4mm, the safety cut edge is 2cm. Roman”>2cm; (4) when the thickness >4mm , the safety cutting edge is 2cm. In patients whose biopsy pathology fails to report a definitive depth, or who have a large lesion, a direct enlarged resection of 2 cm may be considered.
The surgical margins for site-specific melanoma can be adjusted to the patient’s specific primary lesion anatomy and function. Complete surgical excision of facial melanoma is sufficient, and there is no rigid requirement for margin coverage. After complete excision of extremity melanoma, the extent of expansion is generally determined by pathologic staging. From a surgical point of view, surgery for telangiectatic melanoma should not only take into account the cleanliness of the tumor, but also give due consideration to preserving as much function as possible, especially finger function. The aggressive use of amputation to treat acromegaly is not advocated.
For melanoma, amputation is a last resort, but amputation of only the end of the finger or toe is more complete because there is little loss of function. The first choice for melanoma at the end of the finger (or toe) is amputation as a last resort.
- style=”margin-left: 57pt”>
- Posterior lymph node biopsy
Sentinel lymph nodes are the first stop for regional lymph node metastasis in cutaneous and limbic melanoma, and sentinel lymph node biopsy is a means to assess whether regional lymph nodes are metastatic at pathologic stage. Sentinel lymph node biopsy is recommended for patients with tumors Breslow thicker than 1 mm . Sentinel lymph node biopsy is recommended for patients with combined ulcers when reliable depth of infiltration cannot be obtained by biopsy and pathologic techniques. Sentinel lymph node biopsy can be performed concurrently with complete resection or in separate sessions, and it helps to obtain accurate N staging and improve recurrence-free survival. The lymphatic drainage pathway only provides an anatomic reference for the sentinel biopsy, and the final detection of the sentinel lymph node needs to be determined by nuclear probes. Frozen sections are not recommended for intraoperative pathologic diagnosis of sentinel lymph nodes and regional lymph nodes.
- style=”margin-left: 66pt”>
- Lymph node dissection
Surgical indications: positive anterior lymph nodes (lymph node dissection can be withheld if the patient can receive regular lymph node B ultrasound follow-up) , patients with a stage III diagnosis confirmed by physical examination, imaging and pathology.
Surgical principles: complete resection of the base of the involved lymph nodes is required, and inguinal lymph node dissection should be required for at least 10 >more than one, and at least 15 of the cervical and axillary lymph nodes should be dissected. Prophylactic lymph node dissection is not recommended.
inguinal lymph node dissection: for patients with imaging diagnosis of pelvic lymph node metastasis
Superficial group + deep group dissection is required; superficial group + deep group dissection is required for preoperative palpable lymph nodes. span style=”font-family:Times New Roman”>+ deep group clearance; intraoperative detection of ≥3 suspicious lymph nodes in the superficial group or Cloquet lymph nodes with suspicious metastases (black or enlarged lymph nodes) require superficial group + deep group dissection.
Lymph node dissection in the axilla: LEVEL I-III lymph node dissection is performed when supra-axillary group lymph node metastasis is clearly confirmed preoperatively or intraoperatively. Group III lymph node dissection, and only LEVEL Group I-II lymph node dissection when there is no evidence of supra-axillary group lymph node metastasis or when micro-metastasis is confirmed by biopsy of the anterior lymph nodes.
Cervical lymph node dissection: avoid extensive cervical dissection and total cervical dissection as much as possible, and determine the extent of dissection in patients with clinical stage III based on the subdivision of the enlarged lymph nodes and the primary focus.
- style=”margin-left: 57pt”>
- Treatment of local recurrence or local metastasis
Local recurrence or metastasis to the limb can be treated with surgery, isolated limb heat infusion chemotherapy, and isolated limb heat infusion chemotherapy. For local recurrences, surgery remains the primary treatment.
- style=”margin-left: 66pt”>
-
Postoperative adjuvant therapy
The primary goal of postoperative adjuvant therapy is to reduce the patient’s risk of recurrence and metastasis. The main adjuvant drugs currently available for melanoma include: high-dose interferon alpha 2b therapy, BRAF inhibitors± MEK inhibitors (BRAF mutation), PD-1 monoclonal antibodies. Principles of adjuvant therapy for different subtypes of melanoma.
-
cutaneous melanoma: Forstage IIhigh-risk melanoma, high-dose adjuvant interferon therapy is still recommended as the primary treatment. For postoperative patients with stage IIIcutaneous melanoma, it is recommended that PD-1 monoclonal adjuvant. Phase IIC carriesBRAF V600 mutation: vimofenib 1 year.
III Phase III carries the BRAF V600 mutation: dabrafenib + trametinib 1 year.
- Limbic melanoma: High-dose interferon adjuvant therapy is still recommended primarily. For extremity melanoma IIIB~IIIC period or≥3 patients with 1 year regimen may be more beneficial forpatients with lymph node metastases, for IIB~IIIA stage or poorly tolerated patients, 4 week regimen Also available.
-
Mucosal melanoma: Temozolomide in combination with cisplatin recommended Adjuvant chemotherapy 6 cycles group prolonged relapse-free survival. Adjuvant high-dose interferon, adjuvantPD-1 monoclonal antibody may be used as an alternative, but neither improved relapse-free survival time overall as much as adjuvant chemotherapy. In postoperative head and neck mucosal melanoma, local radiotherapy is beneficial to improve local control rates.
-
Uveal melanoma: Some studies have demonstrated that high-dose interferon improves recurrence-free survival in uveal melanoma. Patients are encouraged to enroll in clinical studies.
(ii) Radiation therapy.
Melanoma is generally considered insensitive to radiation therapy (radiotherapy for short), but radiotherapy remains an important treatment in certain special circumstances. Radiotherapy includes: radical radiotherapy of the primary lesion in patients who cannot tolerate surgery, have positive surgical margins but cannot undergo a second surgery; localized postoperative adjuvant radiotherapy of the primary lesion in patients who do not have sufficient safe margins for resection of the primary lesion but cannot undergo another extended resection; adjuvant post-lymph node dissection, palliative radiotherapy of brain and bone metastases, and treatment of small or medium-sized choroidal melanoma.
(iii) Systemic therapy.
For patients with advanced melanoma without contraindications, systemic therapy can
Reducing tumor load, improving tumor-related symptoms, improving quality of life, and extending survival time.
- style=”margin-left: 57pt”>
- Anti-tumor therapy and its efficacy evaluation
-
Molecular targeted drugs: Currently, the domestic marketed melanoma-targeted drugs mainly include:BRAF inhibitors (vimofenib, darafenib),MEK inhibitors (trametinib),KITinhibitors (imatinib, nilotinib).
- style=”margin-left: 74pt”>
- Systemic chemotherapy:Traditional cytotoxic agents, including dacarbazine,
timozolomide, formoglutethimide, paclitaxel, albumin paclitaxel, cisplatin, and carboplatin, have single-agent or conventional combination efficiencies of 10% to 15%.
- Systemic chemotherapy:Traditional cytotoxic agents, including dacarbazine,
- Immunotherapy: Currently, the approved immunotherapy drugs for melanoma in China mainly include PD-1 monoclonal antibodies (pablizumab, teraplizumab).
-
Efficacy assessment of systemic therapy: chemotherapy and targeted therapy using clinical efficacy evaluation criteria for solid tumors () style=”font-family:Times New Roman”>response evaluation criteria in solid tumor, RECIST)1.1 < span style="font-family:Arial">Evaluate the efficacy with reference to both lactate dehydrogenase as well as changes in the degree of tumor necrosis, generally every 66days during the treatment period. “font-family:Arial”>to8 weeks during the treatment period for imaging evaluation, and also by dynamic observation of patients’ symptoms, The assessment is comprehensive by dynamically observing the patient’s symptoms, signs, and treatment-related adverse effects. Immunotherapy can be evaluated using RECIST 1.1 or the Immunotherapy Efficacy Evaluation Criteria for Solid Tumors (). style=”font-family:Times New Roman”>immune RECIST,iRECIST) to evaluate the efficacy.
- style=”margin-left: 46pt”>
- Different subtypes of advanced melanoma
- Different subtypes of advanced melanoma
- Dermal melanoma: if carryingBRAF mutation, consider giving BRAF inhibitor±MEK inhibitor therapy. For late-stage without targeted mutations
stage cutaneous melanoma, either chemotherapy + anti-angiogenic drugs or immunotherapy. For patients with brain metastases, neurosurgical evaluation for surgery or stereotactic radiotherapy in the radiotherapy department is the recommended local treatment option.
-
Extremity melanoma: If carrying “font-family:Times New Roman”>BRAF mutation, consider giving BRAF inhibitors±MEK Inhibitor therapy. For advanced limbic melanoma without targeted mutations, chemotherapy or immunotherapy may be an option. However, immunotherapy alone is less effective in advanced limbal melanoma, and clinical studies of immune combinations for limbal melanoma are ongoing.
- Mucosal melanoma: For advanced mucosal melanoma, chemotherapy may be considered+anti-angiogenic drugs,BRAF inhibitors±MEKinhibitors are important PD-1 monoclonal antibodiesin clinical studies are an important option; +Axitinib is expected to become the standard regimen in the future.
-
Uveal melanoma: Advanced uveal melanoma The main features of treatment are low mutation rate, susceptibility to liver metastasis, insensitivity to immunotherapy, and overall poor prognosis. Chemotherapy+anti-angiogenic drugs±hepatic artery chemoembolization regimens remain an important option in clinical settings.
- style=”margin-left: 54pt”>
- Treatment of specific metastases
- Treatment of specific metastases
- Liver metastases from melanoma: Hepatic artery chemoembolization with cisplatin and formolastine can improve the outcome and survival of liver metastases compared to systemic therapy only.
- Brain metastases from melanoma: Surgical resection remains an important treatment for brain metastases.
Significantly elevated, obstructive hydrocephalus, and uncontrollable epilepsy should be surgically resected. Stereotactic radiotherapy is recommended for melanoma brain metastases, and whole-brain radiotherapy is recommended for patients with symptomatic brain metastases, clinical or pathologic findings of meningeal metastases who are unable to perform stereotactic radiotherapy, and for patients with poor PS scores and too many brain metastases may not be beneficial.
-
Bone metastases from melanoma: Bone metastases from melanoma are treated primarily based on the site of the metastasis (whether it is weight-bearing bone) and symptoms, with treatment aimed at reducing bone events and relieving pain. Isolated bone metastases can be considered for surgical resection, which can be supplemented with local radiotherapy after surgery. Patients with multiple bone metastases should be treated with local therapy in addition to systemic therapy, which includes surgery, bone cement filling and local radiotherapy. Regular treatment with bisphosphonates may reduce the incidence of bone events, and pain medication may be added for patients with pain. The management plan for spinal cord compression depends on the general status of the patient. For patients with a better prognosis and light tumor load, surgical decompression and postoperative radiotherapy can be combined, while radiotherapy alone is considered for patients with poor general condition. The indications for radiotherapy are relief of bone pain and postoperative treatment of internal fixation.
- style=”margin-left: 46pt”>
- Symptomatic supportive therapy
Moderate rehabilitation exercises can strengthen the body’s immune function. In addition, symptomatic supportive therapy should be strengthened, including aggressive analgesia, correction of anemia, correction of hypoalbuminemia, and nutritional support in patients with advanced melanoma, control of blood glucose in patients with combined diabetes, and management of concomitant symptoms such as pleural and abdominal effusion and jaundice.
- Symptomatic supportive therapy
For patients with advanced melanoma, we should understand the patient’s and family’s state of mind, take positive measures to adjust their state of mind accordingly, transform negative psychology into positive psychology, and provide them with a sense of security and comfort and less depression through palliative care. The patient and family should understand the patient’s state of mind and take positive measures to adjust the patient’s state of mind accordingly.
V. Appendix
Appendix I: Clinical Staging and Treatment Roadmap for Melanoma
Appendix II: Staging of Cutaneous Melanoma (AJCC Edition 8)
|
T Staging |
thickness |
ulcer |
|
Tx: primary tumor thickness cannot be measured (e.g. scratch biopsy) those who have been diagnosed) |
not applicable |
Not applicable |
|
T0: no evidence of primary tumor (e.g., no known primary tumor) where the primary tumor is or the primary tumor is completely regressed) |
Not applicable |
Not applicable |
|
Tis(melanoma in situ)< /span> |
Not applicable |
Not applicable |
|
T1 |
≤1.0mm |
unknown or unspecified |
|
T1a |
<0.8mm |
No ulcers |
|
T1b |
T1b |
<0.8mm |
|
0.8~1.0mm< /p> |
with or without ulcers |
|
|
T2 |
>1.0~2.0mm |
< span style="font-family:Arial; font-size:10pt">not known or not specified |
|
T2a |
>1.0~2.0mm |
< span style="font-family:Arial; font-size:10pt">No ulcers |
T2b
>1.0~2.0mm
>
with ulcers
T3
>2.0~4.0mm
unknown or unspecified
T3a
>2.0~4.0mm
No ulcers
T3b
>2.0~4.0mm
With ulcers
tr>
T4
>4.0mm
not known or not specified
T4a
>4.0mm
No ulcers
T4b
4.0mm
with ulcers
|
< span style="font-family:Times New Roman">N Staging (regional lymph nodes) |
Number of lymph nodes involved |
Is there a shift shift, satellite foci and /or microsatellite foci |
|
Nx |
Regional lymph nodes not evaluated (e.g., regional lymph node biopsy not performed, or regional lymph nodes previously removed for some reason) Exceptions:T1 Tumors do not require N N staging, noted as cN |
none |
|
N0 |
No regional lymph node metastasis |
none |
|
N1 |
1 lymph node involvement, or no lymph node involvement but metastases, satellite foci and /or microsatellite foci |
|
|
N1a > |
1 clinically occult lymph node involvement (microscopic metastasis, e.g., anterior lymph node biopsy found) |
none |
|
N1b > |
1 clinically significant lymph node involvement |
none |
|
N1c |
No lymph node involvement |
Yes |
|
N2 |
2~ “font-family:Times New Roman”>3 lymph nodes involved, or 1 < span style="font-family:Arial">lymph node involvement with concomitant metastases, satellite foci and /or microsatellite stoves |
|
|
N2a |
2~3 clinically insidious lymph node involvement (microscopic metastases, as detected by biopsy of anterior lymph nodes) |
none |
|
N2b |
2~3 lymph nodes involved, with at least 1 1 are clinically dominant lymph nodes |
none |
|
N2c |
at least 1 clinically occult or overt lymph node involvement |
< span style="font-family:Arial; font-size:12pt">Yes |
|
N3 |
4 lymph node involvement, or 2 or more lymph node involvement with metastases, satellite foci, and /or microsatellite foci, or any fusion lymph node with or without metastases, satellite foci, and style=”font-family:Times New Roman”>/or microsatellite foci |
|
N3a |
4 >clinically occult lymph node involvement (microscopic metastasis, as detected by biopsy of anterior lymph nodes) |
none |
|
N3b > |
4 or more lymph nodes involved, with at least 1 clinically dominant lymph node, or any number of fused lymph nodes |
|
|
N3c |
2one or more clinically occult or overt lymph node involvement and/or Any number of fused lymph nodes |
Yes |
|
M Staging |
Staging criteria |
|
|
Anatomical site |
Serum lactate Dehydrogenase Levels* |
|
|
M0 |
No evidence of distant transfer |
Not applicable |
|
M1 |
See below |
|
|
M1a |
Distant metastasis to skin, soft tissue weave (including muscle) and/or non-regional lymph nodes |
No record or unclear |
|
M1a (0) |
Not elevated |
|
|
M1a (1) |
elevated |
|
|
M1b |
Distant metastasis to lung, contained or not contained Part in M1a |
Not documented or unclear |
|
M1b (0) |
Not elevated |
|
|
M1b (1) |
elevated |
|
|
M1c |
< span style="font-family:Arial">Distant metastases to non-CNS visceral organs with or without M1aor M1b in parts |
No record or unclear |
|
M1c (0) |
Not elevated |
|
|
M1c (1) |
elevated |
|
|
M1d |
distant transfer to the CNS with or without M1a. M1bor M1c in the part |
No record or unclear |
|
M1d (0) |
Not elevated |
|
|
M1d (1) |
elevated |
|
AJCC The 8th Edition Pathology Staging
N0 N1a N1b N1c N2a N2b N2c N3a N3b N3c Tis < span style="font-family:Times New Roman; font-size:10pt">0 – – – < strong>– – T0 – > – IIIB IIIB < span style="font-family:Times New Roman; font-size:10pt">– IIIC IIIC < span style="font-family:Times New Roman; font-size:10pt">– IIIC IIIC T1a ⅠA IIIA > IIIB IIIB IIIA IIIB IIIC IIIC IIIC IIIC T1b Ⅰ >B IIIA < strong>IIIB IIIB > IIIA IIIB IIIC IIIC IIIC IIIC T2a < strong>ⅠB IIIA > IIIB IIIB IIIA IIIB IIIC IIIC IIIC > IIIC T2b < td style="border-top: none; border-left: none; border-bottom: solid black 0.5pt; border-right: solid black 0.5pt"> < span style="font-size:10pt">IIA IIIB IIIB III >B IIIB < strong>IIIB IIIC > IIIC IIIC T3a IIA IIIB > IIIB IIIB IIIB IIIB IIIC IIIC IIIC > IIIC T3b < td style="border-top: none; border-left: none; border-bottom: solid black 0.5pt; border-right: solid black 0.5pt"> < span style="font-size:10pt">IIB IIIC IIIC III >C IIIC < strong>IIIC IIIC > IIIC IIIC IIIC T4a IIB IIIC IIIC IIIC IIIC > IIIC IIIC IIIC IIIC IIIC T4b IIC < span style="font-size:10pt">IIIC IIIC IIIC III >C IIIC < strong>IIID IIID > IIID M1a < td style="border-top: none; border-left: none; border-bottom: solid black 0.5pt; border-right: solid black 0.5pt"> < span style="font-family:Arial; font-size:10pt">IV < strong>IV IV IV IV IV IV IV < td style="border-top: none; border-left: none; border-bottom: solid black 0.5pt; border-right: solid black 0.5pt"> < span style="font-family:Arial; font-size:10pt">IV < strong>IV M1b IV IV IV < span style="font-family:Arial; font-size:10pt">IV < strong>IV IV IV IV IV IV M1c IV IV IV > IV IV IV IV IV IV IV
IIIC
IIIC
IV
Appendix III: Mucosal Melanoma of the Head and Neck TNM Staging (AJCC Edition 8)
|
T Staging |
standard |
|
T3 |
Tumors are confined to the mucosa and the soft tissues immediately beneath it, regardless of tumor thickness and maximum diameter; for example, nasal polypoid melanoma, oral, pharyngeal, or laryngeal pigmented or non-pigmented melanoma of the oral cavity |
|
T4 |
Moderately progressive or highly progressive |
|
T4a |
Moderate progression: tumor invades deep soft tissue, cartilage, bone, or surface skin |
|
T4b |
Highly progressive: tumor invades brain, dura mater, skull base, low cranial nerves () =”font-family:Times New Roman”>Ⅸ. XX “font-family:Arial”>,D.C., Ⅻ), masticatory space, carotid artery, anterior vertebral space, or mediastinal structures |
|
N Staging |
< span style="font-family:Arial; font-size:12pt">Standard |
|
NX |
Regional lymph nodes not evaluated |
|
N0 |
No regional lymph node metastasis |
|
N1 |
with regional lymph node metastasis |
|
Mstaging |
standard |
|
M0 |
No distant shift < /td> |
|
M1 |
with distant metastases |
Appendix IV. Staging of Choroidal, Ciliary Body Melanoma (AJCC Version 8)
|
T Staging |
standard |
|
|
T1 |
Tumor size 1 level |
|
|
T1a |
tumor size 1 grade, without ciliary involvement without extraspheric growth |
|
|
T1b |
T1b |
Tumor size 1grade with ciliary involvement |
|
T1c > |
Tumor Size 1Grade, without ciliary involvement, with extraspheric growth and maximum diameter ≤5mm |
|
|
T1d > |
Tumor Size 1Grade with ciliary involvement, with extraspheric growth, and maximum diameter ≤5mm |
|
|
T2 |
Tumor size 2Grade |
|
|
T2a |
Tumor size 2< span style="font-family:Arial">Grade without ciliary involvement and no extraspheric growth |
|
|
T2b |
Tumor Size 2 Grade with ciliary involvement |
|
|
T2c |
Tumor Size2 grade, without ciliary involvement, with extraspheric growth and maximal diameter ≤5mm |
|
|
T2d > |
Tumor size 2Grade with ciliary involvement, with extraspheric growth, and maximum diameter ≤5mm |
|
|
T3 |
Tumor size 3 Grade |
|
|
T3a |
Tumor size 3 < span style="font-family:Arial">Grade without ciliary involvement and no extraglomerular growth |
|
|
T3b |
Tumor Size 3 Grade with ciliary involvement |
|
|
T3c |
Tumor Size3 grade, without ciliary involvement, with extraspheric growth and maximal diameter ≤5mm |
|
|
T3d > |
Tumor size 3 Grade with ciliary involvement, with extraspheric growth, and maximum diameter ≤5mm |
|
|
T4 |
Tumor size 4 Grade |
|
|
T4a |
Tumor size 4 < span style="font-family:Arial">Grade without ciliary involvement and no extraspheric growth |
|
|
T4b |
Tumor Size 4 Grade with ciliary involvement |
|
|
T4c |
Tumor Size4 grade, without ciliary involvement, with extraspheric growth and maximal diameter ≤5mm |
|
|
T4d > |
Tumor size 4 Grade with ciliary involvement, with extraspheric growth, and maximum diameter ≤5mm |
|
|
T4e > |
any tumor size with extraspheric growth, maximum diameter > 5mm |
|
N Staging |
standard |
|
N1 |
Regional lymph node metastasis or presence of orbital tumor |
|
1 one or more regional lymph node metastases |
|
N1b |
No regional lymph node metastasis, but independent tumor invasion not contiguous with the eye Orbital |
|
M Staging |
standard |
|
M0 |
Clinical staging without distant metastases |
|
M1 |
with distant shift |
|
M1a |
maximum diameter of maximum metastatic foci ≤3.0cm |
|
M1b |
Maximum diameter of maximum metastatic foci 3.1~8.0cm |
|
M1c |
Maximum diameter of maximum metastatic foci ≥8.1cm< |
AJCC The 8th Edition Pathology Staging
|
T |
N0 |
N1 |
|
T1a |
Ⅰ |
IV |
|
T1b~d |
IIA |
IV |
|
< strong>T2a |
IIA |
IV > |
|
T2b |
IIB |
< span style="font-family:Arial; font-size:10pt">IV |
|
T3a |
IIB |
< strong>IV |
|
T2c~d |
IIIA > |
IV |
|
< strong>T3b~c |
IIIA |
IV |
|
T4a |
IIIA > |
IV |
|
T3d |
III B |
< strong>IV |
|
T4b~c |
IIIB > |
IV |
|
< strong>T4d~ee |
IIIC |
IV |
|
M1a~c |
IV |
IV |
Attachments
Melanoma Diagnostic and Treatment Guidelines (2022 Edition) Development and Validation Expert Group
(in surname stroke order)
Team leader: Guo Jun
Deputy team leaders:Niu Xiaohui, Lin Tongyu, Qin Shucui, and
Members:Yu Shengji, Liu Jiwei, Liu Ting, Liu Weifeng, Li Yongcheng, Wu Di, Zhang Hongxiang, Zhang Yanhua, Zhang Xiaosi, Lu Aiping, Chen Xiaohong, Chen Yu, Slu, Cai Jianqiang, Pan Hongming
Secretaries: Lili Mao, Bin Lian