Cervical Cancer Treatment Guidelines
(2022 Edition)
I. Overview
Cervical cancer is one of the common gynecologic malignancies , with the second highest incidence rate among female malignancies in China. The incidence of cervical cancer is the second most common malignant tumor among women in China , after breast cancer. In 2018 the number of new cases of cervical cancer worldwide exceeded 569,000 and the number of deaths exceeded 31.1 million cases. Of these, 85% of cases occurred
in developing countries. China had about 111 million new cases and deaths in 2015 .
-
million. The distribution of cervical cancer deaths in China is generally slightly higher in rural than in urban areas, and about twice as high in the central and western regions as in the eastern regions. The median age of onset of cervical cancer in China is 51 years, but it is mainly prevalent in 2 age groups, with 40< span style="font-family:Arial">to50years old is the most, years old is the most, years old is the most. span style=”font-family:Times New Roman”>60to70 years old. span>A further peak occurs at the age of 20 . However, it is of concern that the average age of onset of cervical cancer has been gradually decreasing in recent years, with a trend towards younger age. Therefore, there is a great need to standardize the diagnosis and treatment of cervical cancer nationwide. On the other hand, the occurrence of cervical cancer can be effectively controlled through the screening and management of precancerous lesions. Experience in Western countries has shown that the incidence of cervical cancer is reduced by 70% to 90% in people who are closely screened. 2020 Year 11 month 17 on WHO launched the Global Strategy to Accelerate the Elimination of Cervical Cancer.
The guidelines apply to squamous, adenocarcinoma and adenosquamous carcinoma of the cervix, which account for 90% of all cervical cancers. Some specific pathologic types, such as small cell carcinoma, clear cell carcinoma, and sarcoma, have a low incidence and there is no international or national consensus, so this guideline is not appropriate for these rare pathologic types of cervical cancer. This guideline draws on internationally accepted guidelines for the management of cervical cancer, such as the national comprehensive cancer network.
network, network, network, network, network. span>, NCCN) guidelines, the international federation of gynecology and obstetrics (international federation The guidelines of the International Federation of Gynecology and Obstetrics (FIGO), etc., were revised together with the previous guidelines in China. In clinical practice, cervical cancer focuses on the concept of standardized and comprehensive treatment, but also on individualized treatment, which needs to be combined with the hospital’s equipment, technical conditions and the patient’s condition. For patients with complex cervical cancer not covered by this guideline, participation in clinical trials is recommended.
II. Etiology
High-risk human papilloma virus (human papilloma virus, HPV) persistent infection is a necessary factor for the development of cervical cancer and precancerous lesions, i.e. HPV infection is the most critical in the process of cervical carcinogenesis. link. During a woman’s lifetime, the probability of being infected with high-risk HPV is more than 70%, but less than 10% of women develop cervical cancer or cervical intraepithelial neoplasia (cervical intraepithelial neoplasia, CIN), mainly because 80% of women with cervical intraepithelial neoplasia have CIN. span style=”font-family:Times New Roman”>HPV infection is transient. In addition to the role of persistent high-risk HPV infection, the combined involvement and action of other endogenous and exogenous factors are required to cause the development of cervical cancer. Therefore, the risk factors for cervical cancer can be divided into two categories: first, biological factors, namely high-risk HPV persistent infection; and second, exogenous behavioral risk factors.
(i) HPV infection.
Multiple subtypes of 200 have been identified and characterized family:Times New Roman”>HPV, and approximately 54 species can infect the genital mucosa. Each type of HPV is classified into high-risk and low-risk types depending on its risk of cervical cancer. High-risk types (such as HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68 type ) are associated with the development of cervical cancer, especially HPV types 16 and 18 are most closely associated with cervical cancer. Low-risk types of HPV (e.g.
6 The company’s main business is to provide a wide range of services, including 11, 42, 43, 44 ) infections may cause genital and perianal warts. The HPV vaccine is now available in China and can be promoted at an appropriate age to prevent cervical precancer and cervical cancer.
(ii) Behavioral risk factors.
-
Due to HPV is primarily sexually transmitted, some of the possible increases in HPV factors such as young age at sexual debut, multiple sexual partners or partners with multiple sexual partners, poor sexual hygiene, or a history of sexually transmitted diseases can increase HPV infection. Roman”>HPVinfection increases the risk of cervical cancer.
-
Menstrual and maternal factors: early marriage, early childbearing, multiple pregnancies and multiple births, poor menstrual and puerperal hygiene.
- style=”margin-left: 44pt”>
- Smoking.
- Oral contraceptives.
- Smoking.
- Autoimmune disease or long-term immunosuppression (e.g. kidney transplant patients requiring long-term oral immunosuppressive drugs).
-
Poor nutritional status, nutritional disorders: e.g. beta carotene, folic acid, vitamin A, vitamin C , vitamin , vitamin “font-family:Arial”>deficiency, imbalance of trace elements, etc.
III.
(a) Symptoms.
Cervical precancer and early cervical cancer can be asymptomatic. As the severity of lesions increases, contact vaginal bleeding, abnormal leukorrhea such as bloody leukorrhea, increased leukorrhea , irregular vaginal bleeding or postmenopausal vaginal bleeding may occur. In addition, there may be corresponding symptoms due to tumor invasion of other organs, such as invasion of the bladder, which may result in blood.
urine, bloody stool due to invasion of rectum, fistula due to tumor invasion of bladder and rectum, back pain due to parametrial compression of ureter leading to hydronephrosis, cough and hemoptysis due to lung metastasis, etc. The tumor may be infected with fever; there may also be renal failure and cachexia.
(ii) Physical signs.
Early invasive carcinoma of the cervix (stage IA1 and IStage A2 ) may not have any associated abnormal signs, and cervical invasive carcinoma (Stage IStage B1 and above) can be detected by gynecologic examination as cervical masses, which can be broadly classified as cauliflower, The cervical type is sometimes characterized by a smooth cervical surface with only a marked thickening and hardening of the cervical canal. If the vagina is invaded, tumors of the vaginal vault or vaginal wall may be found. In patients with parametrial involvement, gynecologic triangulation may reveal parametrial thickening, such as in stage IIIB patients with tumors extending into the pelvic wall; in advanced patients, enlarged lymph nodes may be found in the groin or supraclavicular region.
IV. Diagnostic tests
(a) Cervical/vaginal cytology smear and HPV test.
Cervical /vaginal cytology smear and HPV testing. family:Times New Roman”>HPV testing is the primary screening tool at this stage for the detection of early cervical cancer and precancerous lesions (CIN), especially for the diagnosis of early lesions with insignificant clinical signs. The material should be taken at the migratory zone of the cervical epithelium, i.e. the area between the junction of the old and new squamous –columnar epithelium. The current main use of cervical fluid-based thin-layer cytology
(thin-prep cytology test, thin-prep cytology test, TCT). The HPV test can be a useful complement to the TCT and the combination of the two is beneficial to improve screening efficiency. For patients with positive HPV16 and 18 types, direct referral for colposcopy with histologic biopsy is recommended.
(ii) Colposcopy.
Colposcopy is useful for detecting precancerous cervical lesions, early cervical cancer, and identifying disease
The site of the lesion is important and can increase the positive rate of biopsies. In medical units where colposcopy is not available, it is possible to apply 3% or 5% acetic acid or iodine solution to the cervix after visualization. The biopsy should be taken in the presence of vinegar white epithelium or where the iodine does not stain and sent for pathological examination. The importance of colposcopic biopsy with cervical canal scraping should be noted, especially when colposcopy reveals squamous intraepithelial lesions extending from the transformation zone into the cervical canal, when cytologic screening suggests atypical glandular cells, and when no squamous –columnar transformation zone is seen colposcopically. Only a specialist colposcopist should decide that cervical canal scraping can be omitted; otherwise, all patients undergoing colposcopic biopsy should undergo cervical canal scraping.
(iii) Gynecologic examination.
Gynecologic examination is the most important tool for clinical staging, which requires 2 gynecologists with associate or higher titles to decide, and once staging is determined , staging cannot be changed after treatment.
- style=”margin-left: 54pt”>
- Visualization
Visualization should be performed under adequate illumination, directly on the vulva and through a vaginal speculum on the vagina and cervix. In addition to general observation, the extent of cancer infiltration, the location, extent, shape, volume, and relationship to surrounding tissues of the cervical tumor should be noted.
- style=”margin-left: 54pt”>
- Palpation
The texture of the tumor, the extent of infiltration, and its relationship to the surrounding area must be determined by palpation. In some cases of submucosal and intraductal infiltration, palpation is more accurate than visual examination. The triadic examination can reveal the presence of infiltrates in the paravaginal, paracervical, and parametrial areas, the relationship between the tumor and the pelvic wall, the uterosacral ligament, the utero-rectal recess, the rectum itself, and the surrounding area.
(iv) Pathologic diagnosis.
Pathologic examination of the cervical histology biopsy under colposcopy or direct vision is the gold standard for final confirmation of the diagnosis. For rare or difficult pathological types (e.g., adenocarcinoma or small cell carcinoma), a free
Immunohistochemistry should be performed to assist in the identification and diagnosis. In cases where the diagnosis is not confirmed by multiple bite biopsies, excisional methods are used when further deeper tissue is required. When cervical surface biopsy is negative, vaginal cytology smear is positive or imaging cannot exclude cervical ductal carcinoma, conical hysterectomy can be performed for pathological examination. Because of the small size of the cervical biopsy tissue, the depth and extent of infiltration of cervical lesions cannot be fully determined, so for early stage IA1 and IA2 cervical biopsies, it is not possible to fully determine the depth and extent of infiltration. span>stage IA and stage IA.
(v) Imaging.
Because of the superficial anatomy, most cervical cancers can be diagnosed by gynecologic examination and cytopathologic examination. The value of imaging in the diagnosis of cervical cancer is mainly to understand the extent of metastasis, invasion and degree of tumor (including evaluation of the extent of local invasion, lymph node metastasis and distant organ metastasis), to guide clinical decision making and to evaluate the efficacy. Imaging methods used for cervical cancer include.
- style=”margin-left: 62pt”>
-
Abdominopelvic ultrasound
It is mainly used to visualize localized lesions in the cervix and to observe metastases in the pelvic and retroperitoneal regions, as well as metastases in other organs of the abdominopelvic cavity, and to detect metastases in superficial lymph nodes. Due to resolution limitations, assessment of cervical focal lesions and systemic metastases is currently based on MRI and CT.
- style=”margin-left: 62pt”>
-
Pelvic Pelvic span>MRI
Radiation-free, multi-sequence, multi-parametric imaging with excellent soft tissue resolution is the best imaging method for cervical cancer, helping to detect lesions and determine their size and location, especially for biopsies of CIN3 patients can be used to exclude endogenous lesions; define the extent of lesion invasion, provide an important basis for pre-treatment staging, and show lesion invasion of the uterus.
Depth of the cervical stroma, to determine whether the lesion is confined to the cervix, invades the parametrium, or invades the pelvic wall. It is difficult to distinguish between a lesion protruding into the vaginal cavity adjacent to the vaginal wall and a direct invasion of the vaginal wall. Lymph node metastases in the pelvis, retroperitoneum and inguinal region are also detected. For patients treated non-operatively, it can be used for radiotherapy target area outlining, in-treatment efficacy monitoring, end-of-treatment efficacy assessment, and post-treatment follow-up.
- style=”margin-left: 62pt”>
-
Abdominopelvic. /span>CT.
CT has low soft tissue resolution, and the density of flat-scan lesions is similar to that of the normal cervix. The contrast of enhanced CT scans is better than that of plain scans, but nearly 1/2 of the lesions are equivocal. span>of lesions are isointense and difficult to define the extent. The advantages of CT are mainly in the demonstration of intermediate and advanced lesions, the evaluation of cervical lesions in relation to surrounding structures (e.g., bladder, rectum, etc.), lymph node metastases, and the presence of metastases in other organs of the abdominopelvic cavity on a wide scan. For patients with contraindications to MRI, CT is an option.
- style=”margin-left: 62pt”>
-
Chest Radiography and Chest Photography and chestCT examinations
The main purpose is to exclude lung metastases and mediastinal lymph node metastases, chest X-ray can only exclude obvious lung metastases and cannot evaluate mediastinal lymph nodes, so hospitals that have the conditions should still perform chest CT should be performed if available.
- style=”margin-left: 62pt”>
-
Nuclear medicine imaging
Positron emission computed tomography (positron emission) is not recommended. tomography-computed tomography, PET-CT) for the evaluation of local infiltration of cervical cancer, but PET-CT is recommended for those who are able to use it in the following cases “font-family:Times New Roman”>PET-CT: (1) FIGO staging of stage IB1 and above in primary patients with pre-treatment staging (including stage IB1 with preserved birth
patients with functional needs for fertility); (2) patients who underwent hysterectomy for other reasons (3) Patients with unexpected detection of cervical cancer by simple hysterectomy for other reasons to be evaluated systemically; (3) Patients who need imaging assistance to outline the target area for proposed radiotherapy; (4) Patients with high-risk factors are monitored at the end of treatment 3 to 6 months later; (5) patients with suspected recurrent metastases during follow-up, including the development of clinical symptoms or elevated associated tumor markers. Nuclear bone scan is only used for patients suspected of having bone metastases.
- style=”margin-left: 54pt”>
- Lumpectomy
Cystoscopy and proctoscopy: Patients with clinical suspicion of bladder or rectal invasion should undergo appropriate lumpectomy. If not, the patient should be referred to a higher level hospital.
(vi) Tumor marker examination.
Abnormally elevated tumor markers can assist in diagnosis, efficacy evaluation, disease monitoring, and post-treatment follow-up monitoring, and are especially important in follow-up monitoring. Serum squamous carcinoma-associated antigen levels above 1.5ng/ml are considered abnormal. Because squamous cell carcinoma is the most common form of cervical cancer, squamous carcinoma-associated antigen is the most commonly tested serologic tumor marker in the diagnosis and treatment of cervical cancer. Cervical adenocarcinoma can have carcinoembryonic antigen, glycoconjugate antigen (carbohydrate antigen, CA >) elevation of 125 or CA19-9 .
V. Classification and staging of cervical cancer
(A) Histological classification of cervical cancer.
Cervical cancer mainly includes cervical squamous cell carcinoma, adenocarcinoma, adenosquamous carcinoma, and other rare types. Among them, squamous cell carcinoma is the most common, accounting for about 80%, and adenocarcinoma accounts for 15% to 20%. With the development of cervical cancer screening, the incidence and mortality rate of squamous cell carcinoma of the cervix have been decreasing, but the incidence of adenocarcinoma has been increasing in recent 30 years. The prognosis of squamous carcinoma is the best among the various pathological types, and the prognosis of cervical adenocarcinoma and adenosquamous carcinoma is relatively poor.
This difference is more pronounced in patients with advanced disease. The current pathological types of cervical malignancies are mainly based on the pathological staging published by the World Health Organization (WHO, 2014 ) (Table 1).
Table 1 Histologic classification and coding of cervical tumors (< span style="font-family:Times New Roman">WHO, 2014)
|
Histological classification of tumors |
Coding |
||
|
epithelial tumors |
|||
|
Squamous carcinoma and precursor lesions |
|||
|
squamous intraepithelial lesions |
|||
|
Low-grade squamous intraepithelial lesions |
8077/0 |
||
|
High-grade squamous intraepithelial lesions |
8077/2 |
||
|
Squamous cell carcinoma, non-specific type (NOS) |
8070/3 |
||
|
Keratotic carcinoma |
8071/3 |
||
|
Non-keratinizing carcinoma |
8072/3 |
||
|
papillary squamous carcinoma |
8052/3 |
||
|
basal-like carcinoma |
8083/3 | ||
|
< span style="font-family:Arial; font-size:14pt">Wart cancer |
8051/3 |
||
|
Warty carcinoma |
8051/3 |
||
|
Squamous–Migratory cell carcinoma |
8120/3 |
||
|
Lymphoepithelioma-like carcinoma |
8082/3 |
||
|
Benign squamous epithelial lesions < /td> | |||
|
Squamous metaplasia |
|||
|
Acute Warts |
|||
|
Squamous epithelial papilloma |
8052/0 |
||
Migratory cell metastatic adenocarcinoma and precursor lesion adenocarcinoma in situ 8140/2 adenocarcinoma 8140/3 cervical adenocarcinoma, common type 8140/3 mucinous carcinoma, non-specific (NOS) 8480/3 gastric type 8482/3 intestinal type 8144/3 indolent cell type 8490/3 choriocarcinoma 8263/3 endometrioid carcinoma 8380/3 clear cell carcinoma 8310/3 plasmacytoma 8441/3 mesonephric ductal carcinoma 9110/3 mixed adenocarcinoma-neuroendocrine carcinoma 8574/3 benign glandular Epithelial tumors and neoplastic lesions cervical polyps mullerian epithelial papilloma nasal cyst tunnel-like glandular plexus microglandular hyperplasia lobular cervical glandular hyperplasia diffuse laminar cervical duct glandular hyperplasia mesonephric duct remnants and hyperplasia A-S reaction cervical duct endometriosis endometriosis fallopian duct endometrioid chemosis ectopic prostatic tissue other epithelial tumors adenosquamous carcinoma 8560/3 hairy glass cell carcinoma 8015/3 Adenoid basal cell carcinoma 8098/3 adenoid cystic carcinoma 8200/3 undifferentiated carcinoma 8020/3 neuroendocrine tumor low-grade neuroendocrine tumor carcinoid 8240/3 atypical carcinoid 8249/3 high-grade neuroendocrine carcinoma small cell neuroendocrine carcinoma (small cell carcinoma) 8041/3 large cell neuroendocrine carcinoma 8013/3 mesenchymal tumor and aneurysmal lesion benign smooth muscle tumor 8890/0 rhabdomyosarcoma 8905/0 other malignant smooth muscle sarcoma 8890/3 rhabdomyosarcoma 8910/3 adenoid soft tissue sarcoma 9581/3 angiosarcoma 9120/3 malignant peripheral nerve sheath tumor 9540/3 other sarcoma liposarcoma 8850/3 undifferentiated cervical sarcoma 8805/3 ewing sarcoma 9364/3 oncotic lesion post-surgical spindle cell nodule Lymphoma-like lesion mixed epithelial-mesenchymal tumor adenomyoma 8932/0 adenosarcoma 8933/3 carcinosarcoma 8980/3 melanoma blue nevus 8780/0 malignant melanoma 8720/3 germ cell tumor yolk cystic tumor lymphatic and myeloid tumor lymphoma myeloid tumor secondary tumor
(ii) Staging of cervical cancer.
The clinical staging criteria for cervical cancer as modified by the FIGO 2018 meeting are currently used. Clinical staging is determined by gynecologic examination (Table 2). Firstly, the width of horizontal interstitial infiltration is no longer considered in the diagnosis of stage IA. The new version of the criteria only differentiates stage IA1 from stage IA2 according to the depth of interstitial infiltration, mainly because the width may be influenced by human factors. Secondly, the sub-stage of stage IB has been refined, from the original 2 sub-stages to 3 sub-stages, which is more conducive to the selection of postoperative adjuvant therapy and prognosis of patients. The last important change is the inclusion of lymph node metastasis in the staging system, defining lymph node metastasis as stage IIIC, and the addition of evidence labeling for lymph node metastasis (r for imaging lymph node metastasis and p for pathologic confirmation).
Table 2 Clinical staging criteria for cervical cancer of the International Federation of Gynecology and Obstetrics (FIGO 2018)
Staging description Ⅰ Tumor strictly confined to the cervix (extension to the uterine body will be ignored) ⅠA Infiltrating carcinoma diagnosed microscopically only, with a maximum depth of infiltration measured ≤5.0 mm 
, the
Vesicular edema cannot be classified as stage IV IVA tumor invading bladder or rectal mucosa IVB tumor spreading to distant organs
VI. Treatment
(A) Treatment modalities of cervical cancer.
Cervical microscopic infiltrating carcinoma (micro-infiltrating carcinoma)
As the determination of stage IA tumor is based on microscopic measurement, the bitten biopsy specimen cannot contain all lesions and cannot measure the extent of lesions, so cone biopsy is required for proper diagnosis.
Extra-fascial total hysterectomy (type I hysterectomy) is feasible for stage IA1 patients without fertility requirements. If the patient has fertility requirements, cervical conization is performed, and patients with negative margins are followed up regularly. Because of the lymph node metastasis rate in stage IA1<1%, lymph node dissection is currently considered unnecessary in stage IA1. If the lymphatic vascular space is invaded, cervical conization (with negative margins) or revisional radical hysterectomy with pelvic lymphadenectomy can be performed.
For stage IA2 cervical cancer, the lymph node metastasis rate is about 3%-5%, and subextensive hysterectomy (type II modified radical hysterectomy) with pelvic lymph node dissection is feasible. For those who want to preserve reproductive function, cervical conization (with negative margins) or radical hysterectomy with pelvic lymph node dissection can be chosen (radical hysterectomy is recommended for patients with reproductive requirements).
Invasive cervical cancer
Stage IB1, IIB2, IIA1: Good prognosis with surgery or radiotherapy.
The surgical approach is type III radical hysterectomy and pelvic lymph node dissection ± abdominal aortic lymph node sampling. The adjuvant postoperative treatment is described as radiation therapy. If the cervical tumor does not exceed 2 cm in diameter, radical hysterectomy with pelvic lymph node dissection ± abdominal aortic lymph node sampling can be chosen for those who require preservation of fertility.
Stage ⅠB3, ⅡA2: the treatment options are: ① Simultaneous radiotherapy.
(2) Radical hysterectomy with pelvic lymph node dissection, abdominal aortic lymph node sampling, and postoperative individualized adjuvant therapy; (3) Surgery after neoadjuvant chemotherapy; (4) Adjuvant hysterectomy after synchronous radiotherapy and chemotherapy. The FIGO guidelines (2018) recommend an additional option for the treatment of locally advanced cervical cancer, namely radical hysterectomy and lymph node dissection after neoadjuvant chemotherapy. The impact of neoadjuvant chemotherapy followed by surgery on the prognosis of patients with cervical cancer is still controversial and is generally recommended in clinical trials or in areas where radiotherapy is not available, especially for pathological types that are relatively insensitive to radiotherapy (e.g. adenocarcinoma).
The overall 5-year survival rate for stage IB is approximately 80%-90%, with only 40%-70% for those with cervical tumors larger than 4 cm in diameter, with high-risk factors such as lymph node metastasis, parametrial invasion, and/or positive cut margins. When choosing treatment for some patients with early-stage cervical cancer, it should be considered that patients with high-risk factors may benefit more from radiotherapy. The standard treatment for locally advanced patients is still considered to be simultaneous radiotherapy.
Stage IIB-IVA: Synchronized radiotherapy (see Radiotherapy and Sensitization Chemotherapy for specific protocols)
-
IVB<
(ii) Surgical treatment.
Surgical treatment is mainly applied to early-stage cervical cancer, i.e. ⅠA >~IIA stage. The surgery consists of both hysterectomy and lymph node dissection. The extent of resection varies by stage. To better describe the extent of surgical resection, several authors have tried to propose various staging systems for cervical cancer surgery, including the Piver staging and the Q-M staging is the surgical staging system for cervical cancer that is accepted and adopted by most scholars nationally and internationally.
1. Piver surgical staging system
The Piver 5, which was proposed in 1974 . type hysterectomy classification system is still widely used today.
used.
Type I: extrafascial hysterectomy. [Type I: extrafascial hysterectomy.
patients with lymph-vascular space invasion (LVSI)]
Type II: modified radical hysterectomy that also includes the 1/2 sacral, main ligament, and upper 1/3 vagina. (for patients with stage IA1 with LVSI and stage IA2)
Type III: radical hysterectomy including resection of the main ligament adjacent to the pelvic wall, resection of the sacral ligament from the sacral attachment, and resection of the upper 1/2 vagina. 2 of the vagina. (standard radical hysterectomy for patients with stage IB1, IB2, and selective IB3/IIA1)
Type IV: Extended radical hysterectomy. (for some recurrent patients) Type V: pelvic organ contouring. (for some patients with stage IVA and recurrence) 2. Q-M Surgical staging
In order to more accurately describe the scope of surgery and better individualize the surgical plan, 2008 French experts Querleu and Morrow consulted with anatomists and cervical cancer surgeons from around the world to synthesize a new radical cervical cancer treatment This three-dimensional anatomy-based staging is also known as Q-M staging. In 2015 , the US NCCN guidelines recommended the use of Q-M staging .
Q-M staging includes both surgical staging of the uterus and lymph node dissection grading. The surgical staging relates only to the extent of parametrial resection, which is defined by a fixed anatomic structure.
Type A (minimal paracervical resection type) paracervical tissue is resected to the medial ureter, but the uterosacral ligament and bladder-uterine ligament are largely unresected on the lateral side of the cervix, and the vagina is resected
<1cm, without resection of the paravaginal tissue. (for stage IA1 patients without LVSI) Type B (resection of paracervical tissue up to the ureter) Paracervical tissue resection up to the ureter
Tunnel level, partial excision of the uterosacral and bladder uterine ligaments, no excision of the sacral plexus below the deep uterine vein in the paracervical tissue, and vaginal excision of at least 1 cm (for stage IA1 with LVSI and stage IA2 patients)
B1 as described above
B2 as described above with parametrial lymph node dissection
Type C (resection of paracervical tissue to the junction with the internal iliac vascular system) resection of the cysto-uterine ligament at the level of the bladder, resection of the vagina and associated paravaginal tissue 1.5-2 cm from the tumor or lower edge of the cervix (for IB1, IB2) (for patients with stage IB1, IB2, selective IB3/IIA1)
C1 preserved autonomic nerve C2 not preserved autonomic nerve
Type D (lateral enlarged resection) resection of paracervical tissue up to the pelvic wall, vascularization over the internal iliac vascular system, and exposure of the sciatic nerve root completely free (for some patients with stage IVA and recurrence)
D1 Excision of paracervical tissue to the pelvic wall
D2 As described above, with resection of the inferior abdominal vessels and accessory fascia or muscle tissue (pelvic
expanded resection of the cavity)
Grading of lymph node dissection : The extent of retroperitoneal lymph node dissection, using the artery as an anatomic landmark, is divided into 4 levels. Closed lymph nodes were routinely resected by default. Grade 1 : resection of peri-iliac artery lymph nodes, with Grade 2 demarcated by the bifurcation of the internal and external iliac arteries;< span style="font-family:Times New Roman">Grade 2 : resection of peri-iliac lymph nodes, with Grade 3 demarcated by the bifurcation of the abdominal aorta;Grade 3 : resection of the parietal aortic lymph nodes to the level of the inferior mesenteric artery; Grade 4 : resection of the lymph nodes to the level of the inferior left renal vein of the abdominal aorta .
Postoperative abnormal bladder function, abnormal colorectal motility, and abnormal sexual function due to damage to the pelvic autonomic nerves from radical hysterectomy, radical hysterectomy with preservation of nerves (nerve-sparing radical hysterectomy, NSRH) has been continuously researched and promoted, and NSRH has been used to treat patients with autonomic nerve injury. span style=”font-family:Times New Roman”>NSRH surgery belongs to the Q-M fraction of C1 type radical treatment, NSRH can be accomplished by open, laparoscopic, and robotic laparoscopic routes.
Extrafascial hysterectomy (type I or Type A ) can be done by transvaginal or open or minimally invasive (laparoscopic and robotic laparoscopic) routes. There are now prospective randomized controlled trials showing lower disease-free and overall survival rates with minimally invasive radical hysterectomy compared with open radical hysterectomy.
Lymph node dissection in cervical cancer surgery involves pelvic lymph nodes and abdominal aortic lymph nodes. IA1 (with LVSI) /span>) to IIStage A A should be performed with pelvic lymph node dissection ± abdominal para-aortic lymph node sampling. The study showed that the postoperative pelvic lymph node metastasis rates in patients with stage I and stage II cervical cancer were 0 to 16.5%, respectively. Roman”>0-16.0% and 24.5%-31.0%, respectively. Therefore, selective lymph node dissection according to the status of anterior lymph node metastasis can reduce the incidence of postoperative complications in patients with cervical cancer. The tracers used for sentinel lymph node detection are biological dyes, radioisotopes, and fluorescent dyes, which can be identified by visual recognition, nuclide detection, or infrared light.
detection. Systemic lymph node dissection and localized resection of anterior lymph nodes can be accomplished by open, laparoscopic, and robotic laparoscopic routes.
I-IIA stage squamous cervical cancer has an ovarian metastasis rate of less than 1%, and normal-looking ovaries can be preserved intraoperatively in non-menopausal patients who require preservation of ovarian function. The probability of occult ovarian metastasis in cervical adenocarcinoma is currently considered to be high, so preservation of the ovaries should be done with caution. The preserved ovary can be relocated intraoperatively (e.g., intraperitoneally or high in the retroperitoneal paracolic sulcus) to avoid damage to ovarian function from postoperative pelvic radiotherapy.
In recent years, fertility-preserving surgery has been performed in young patients with early-stage cervical cancer without lymph node metastases who desire fertility. Stage IA1 without LVSI is feasible. Cervical conization with negative margins is feasible, and hysterectomy is feasible if the lesion is extensive; IA1 with LVSI and Stage IA2 patients with viable margins Negative (negative margin width preferably up to 3mm) cervical conization / hysterectomy / =”font-family:Times New Roman”>+ transabdominal or laparoscopic pelvic lymph node dissection ± with abdominal para-aortic lymph node sampling, or radical transabdominal, transvaginal or laparoscopic cervical resection + pelvic
luminal lymph node dissection ± with sampling of the para-aortic lymph nodes in the abdomen; IB1 stage (<2cm) pick
with radical hysterectomy + pelvic lymph node dissection ± abdominal para-aortic lymph node sampling. For IA2 to IB1 period with LVSI and IStage IB2 patients have not yet reached a uniform conclusion on the feasibility of fertility-preserving surgery and need to be considered carefully.
Patients with cervical cancer need to select adjuvant therapy after surgery based on risk factors for recurrence to reduce recurrence rates and improve prognosis, as detailed in the section on principles of radiation therapy.
(iii) Radiation therapy.
Medical institutions that are not qualified for radiotherapy should promptly refer patients who need radiotherapy to medical units that are qualified for it. Patients with cervical cancer who require intracavitary brachytherapy should be advised to seek treatment at
Patients with cervical cancer requiring intracavitary brachytherapy should be advised to consult with the appropriate unit prior to external irradiation to avoid interruption of radiotherapy.
For all stages of cervical cancer. Radiotherapy includes external irradiation and brachytherapy or a combination of the two. Studies have shown that simultaneous radiotherapy improves the efficacy and reduces the risk of recurrence compared with radiotherapy alone. In patients with early-stage cervical cancer, pathological examination after surgery reveals high-risk factors (unclear surgical margins, parametrial invasion, lymph node metastasis, etc.) or intermediate-risk factors (intraoperative / if large tumors, deep interstitial invasion and / or interstitial invasion of the vasculature) need to be supplemented with postoperative adjuvant radiotherapy.
- style=”margin-left: 53pt”>
- Principles of radiotherapy
The principles of radiotherapy for malignant tumors, like other treatments, are to maximize the killing of cancer cells and to protect normal tissues and vital organs as much as possible, i.e., to maximize the therapeutic effect and minimize complications. Therefore, appropriate treatment tools, appropriate irradiation range, adequate irradiation dose, uniform dose distribution, reasonable irradiation volume, and individual treatment are the basic requirements of radiotherapy.
The duration of radiotherapy completion is a necessary factor for optimal outcomes. The duration of radiotherapy beyond 9
weeks have a higher rate of pelvic control failure than patients treated for less than 7 weeks, and the recommended 56 days to complete all external irradiation and brachytherapy.
When radical radiotherapy is administered, a radical dose of radiation is given to the tumor area, and because of the large area and high dose, treatment should focus on the normal tissues and organs adjacent to the tumor, especially those that are sensitive to radiation. The purpose of palliative radiotherapy is to protect the tumor from the radiation. The purpose of palliative radiotherapy is to alleviate symptoms and reduce patient suffering, but it may not necessarily prolong the survival time of patients. Radical and palliative treatments are relative and can be interchanged during treatment depending on the tumor and the patient’s condition.
If radiotherapy is combined with surgery, the decision to use postoperative radiotherapy depends on the tumor and the patient’s condition. Preoperative radiotherapy is planned to reduce the viability of cancer cells or reduce the chance of implantation and spread; to reduce the extent of tumor and improve the surgical resection rate; to kill subclinical lesions and reduce the local recurrence rate. Postoperative radiotherapy is decided according to the pathological examination results after surgery, and has adverse prognostic factors: if there are any high-risk factors such as unclean surgical margins, parametrial invasion, or lymph node metastasis, postoperative adjuvant radiotherapy is required. If intermediate risk factors such as large tumor, deep mesenchymal invasion and / or interstitial invasion of the vasculature are found after intraoperative /, the patient will be treated according to /. span style=”font-family:Times New Roman”>2015 NCCN guidelines for Sedlis criteria (Table 3), postoperative adjuvant pelvic radiotherapy or radiotherapy is required. If lymph node metastasis, positive cut margins, parametrial infiltration, deep mesenchymal infiltration, large local tumor volume in the cervix, and vascular tumor embolism, postoperative radiotherapy is feasible, and postoperative adjuvant radiotherapy reduces local recurrence and improves outcomes, but the use of both surgery and radiotherapy also increases treatment complications.
Table 3 Indications for postoperative pelvic radiotherapy for cervical cancer combined with intermediate risk factors
|
LVSI |
depth of interstitial infiltration |
Tumor diameter (clinical examination) |
|
+ |
outside 1/3 |
any size |
|
+ |
Mid 1/3 |
≥2cm |
|
+ |
in 1/3 |
≥5cm |
|
– |
Medium 1/3 and outside 1/3 |
≥4cm |
- style=”margin-left: 54pt”>
- Extracorporeal irradiation
- style=”margin-left: 42pt”>
-
Conventional radiotherapy: i.e. radiotherapy under positioning in a simulator or CT simulator. Target areas: should generally include uterus, cervix, parametrium and upper 1/2 vagina, pelvic gonadotrope
Bar drainage areas such as internal iliac, foramen ovale, external iliac, and common iliac lymph nodes. Stage IIIA patients include all
part of the vagina. Include the groin area if necessary. Four-field box irradiation or isocentric anterior-posterior penetration irradiation is used. Apply high-energy 6 to 12MV X rays.
Boundaries: upper boundary: ventral main bifurcation (generally at L3 inferior edge to L5 superior border); inferior border: lower border of the foramen occulta (IIIA stage patients), the line between its endpoint and the widest part of the set field passes approximately through the internal femur 1/3; external: outside the true pelvis 1.5 ~2.0 cm; anterior border: anterior border of the pubic symphysis (depending on the tumor); posterior border: all of the sacrum within the irradiated field (depending on the tumor). A multileaf grating or irregular lead-blocking shield was applied to protect normal tissue.
Dose: conventional fractionated irradiation at 1.8 ~2.0Gy per week. style=”font-family:Times New Roman”>5 times per week. Total dose 45 to 50Gy, 5 to 6 weeks.
-
3D conformal radiotherapy and intensity-modulated conformal radiotherapy: to CT or MRIbased plan design and conformal shielding techniques are the current standard of care for external radiation therapy. For patients with inoperable cervical cancer, positron emission tomography (positron emission tomography, PET) examination helps to determine the extent of lymph node metastasis and also helps to determine whether the patient has residual positive postoperative lymph nodes for diagnosis. The tumor target area (gross target volume, based on gynecologic examination as well as imaging span style=”font-family:Times New Roman”>GTV), to identify clinical target areas by direct cervical cancer spread and lymph node metastasis pathways () (clinical target volume, CTV ). The target area for external irradiation needs to include the uterine body, cervix, parametrium, vagina (lower border at least 3 cm from the tumor) and the corresponding lymphatic drainage area . If no positive lymph nodes are found on surgery or imaging, irradiation should include the external iliac lymph nodes, internal iliac lymph nodes, foraminal lymph nodes, and presacral lymph node drainage areas. If the risk of lymph node metastasis is high (e.g.
Tumor volume ≥4 cm or IIstage B or more or suspicious /identified lymph node metastases in the true pelvis).
Irradiation will also include the common iliac lymph node area. If metastases to the common iliac or para-aortic lymph nodes have occurred, irradiation of the extended pelvic field and para-aortic lymph nodes is required, with the upper border
The upper border should be at the level of the renal vasculature (or higher depending on the extent of lymph node involvement). If the lesion has invaded the inferior 1/3 of the vagina, bilateral inguinal lymph nodes should also be included in the irradiation. With CTV outwardly placed at a certain distance (0.5 to 1.5 cm) to form the planned target area (0.5 to 1.5 cm) = “font-family:Times New Roman”>planning target volume, PTV). Radiotherapy dose: 45-50Gy/1.8-2Gy/5-6 weeks, while evaluating organs at risk, such as rectum, sigmoid colon, bladder, small intestine, bone, and other organs at risk in the irradiation range. For unresectable solid tumors or size-limited sarcoid lesions or metastatic lymph nodes, the lesions can be treated with an additional dose of 10 ~20 Gy using intensity-modulated conformal radiotherapy techniques.
- style=”margin-left: 54pt”>
- Near radiation
Intracavitary irradiation is the direct placement of a sealed radioactive source into the body’s natural canal (e.g., uterine cavity, vagina, etc.). The radiation source is placed directly into the tumor tissues for inter-tissue irradiation, both of which are considered to be brachytherapy. The cervical and vaginal cavities have a high tolerance for radiation, the source is closest to the tumor, and the radiation effect can be achieved with a small volume of radiation.
- style=”margin-left: 74pt”>
-
Internal irradiation of radioactive sources: see Table 4.

|
Radiation sources |
radium-226 |
Cobalt– 60 |
Cesium-137 |
Iridium-192 |
| < p style="margin-left: 5pt">Radiometric ratio (Ci/cm 3) |
2.1 Maximum 3.8 |
< span style="font-family:Times New Roman; font-size:14pt">1900 |
27.5 |
9000 |
|
Half-life |
l590 year |
5.3 Year |
33 < span style="font-family:仿宋">Year |
74 days |

- Traditional intracavitary irradiation methods: the Stockholm, Paris, Manchester, and Beijing methods, which mostly use radium and cesium radioactive sources, are less commonly used today.
-
Post-mounted intracavitary radiotherapy and dose calculation: Post-mounted intracavitary radiotherapy involves placing an unloaded radiation vessel in the body cavity at the site of the lesion, and then placing it under protective shielding. The radiation source is then transported through the tube to the vessel for treatment at a distance with protective shielding.
Intracavitary radiotherapy is an important treatment in radical radiotherapy for cervical cancer. Intracavitary therapy using a cervical tube combined with a vaginal applicator is the most common method. Depending on the patient and the anatomical characteristics of the tumor, different vaginal applicators are selected for use in combination with the cervical tube. When combined with external radiation therapy, brachytherapy is usually administered in the late phase of radiation therapy when the tumor volume has shrunk significantly, allowing the placement of the applicator to achieve the ideal dose geometry for brachytherapy. Post-mounted intracavitary therapy machines can be divided into 3 categories according to their dose rates to the A site: low dose rate (0.667 ~3.33cGy/min), medium dose rate (min), medium dose rate (3.33
~20cGy/min), high dose rates (above 20cGy/min ). Weekly cone-beam CT validation is recommended for radical intensity-modulated conformal radiotherapy, and at the end of the 3 week external beam radiotherapy The imaging assessment determines whether the radiotherapy schedule needs to be modified.
Usually 1 to 2 times per week, and 2 times per week. span>times per week A point dose at 5 to 10 Gy, A site total dose in the range of 20 to 45Gy and total extracorporeal plus cavity therapy dose not less than 75Gy [2Gy fractionated radiation equivalent dose (equivalent dose in 2Gy/f, EQD2)], the total dose of extracorporeal plus intracavitary radiotherapy for the whole course varies according to the clinical stage and tumor size, and the total dose is usually between 2Gy/f and 2Gy/f. family:Times New Roman”>75-90Gy. The rectal and bladder ICRU reference point dose is limited to A point prescription dose of
60% to 70% or less, up to 80%, and consider reducing the residency site or lowering the prescribed dose for overdose. The dose recommendations in the NCCN guidelines for A point are based on traditional,
extensively validated low-dose rate and segmented brachytherapy. In this dose system, external irradiation is delivered at 1.8 to 2 Gy per day, and brachytherapy is delivered at a low dose rate of 40 to 70 cGy/h at A point dose. If high dose rates are used for brachytherapy, the dose at the high dose rate at the A point needs to be converted to a low dose rate dose with the same biological effect by a linear quadratic model with the formula:EQD2=D×(d+α/β)
(/ 2+α/β) , D is the actual total physical dose, d is the single dose, and tumor tissue α/β=10
Gy and normal tissue assessed for its late response at α/β=3 Gy (rectum, bladder, sigmoid colon). The most common high-dose-rate brachytherapy is to perform 4 or 5 sessions of brachytherapy. Roman”>5 sessions of uterine and vaginal applicator placement at A point dose of 6 or span style=”font-family:Times New Roman”>7 Gy, with a total A point dose of 28 Gy/4 times or 30 Gy/5 times, translating into a low dose rate equivalent biological dose of A point 40 Gy. To improve treatment outcomes and reduce the risk of radiotherapy complications, the use of image-guided 3D brachytherapy for intracavitary post-mounted radiotherapy is recommended for medical institutions in a position to do so.
But because the three-dimensional shape of the tumor and the interrelationship between the tumor and normal tissue structures are not taken into account, A point and ICRU rectal and bladder reference points have significant limitations. Image-guided brachytherapy has been shown to improve patient survival and reduce treatment side effects. MRI is the best imaging method for residual tumor assessment and is best performed MRI before brachytherapy. MRI can also be used when no CT equipment is available, but CT is much less accurate than MRI in determining the extent of the lesion and in outlining the target area. The dose target for brachytherapy is calculated in EQD2 , and the dose of brachytherapy can be reduced appropriately for small tumors and rapidly regressing tumors. Three-dimensional afterloading is recommended using the GTV, CTV recommended by the European Brachytherapy Group and the European Society of Radiation Oncology for three-dimensional afterloading treatment. span>concept, applying MRI images to outline the target area to T2WI sequences to show the tumor extent as GTV. Combining CTV
According to the risk of tumor load and recurrence into 3 categories: high-risk CTV (high risk CTV, HR-CTV) includes the extent of cervical and naked eye tumor invasion; intermediate-risk CTV
(intermediate risk CTV, IR-CTV) indicates the obvious microscopic tumor area, which is recommended to include the extent of tumor before the start of external irradiation; low-risk CTV refers to the possible microscopic dissemination area, which is usually treated with surgery or external irradiation. treatment. It is recommended that D90, D100
evaluate GTV, HR-CTV and IR-CTV at doses of V150, V200
to evaluate the high dose volume; with D1cm3, D2cm3
to assess the amount of organ endangerment. The A point dose still needs to be reported as a reference to evaluate the target area dose. HR-CTV dose up to 80 Gy, for large tumor size or poorly regressed lesions, the dose should < span style="font-family:Times New Roman">≥87 Gy. According to published guidelines, the limiting doses for normal tissue are: rectum 2 cm 3≤65 ~75 Gy; sigmoid colon 2 cm 3≤65 ~75 Gy; sigmoid colon 2cm3 ≤ 70 ~75 Gy; bladder 2cm< span style="font-size:10pt">3≤80 ~90 Gy. If these parameters are not met, additional intertissue insertion techniques should be considered to increase the dose.
- style=”margin-left: 54pt”>
- Combination of intracavitary and extracorporeal irradiation
With the exception of very few early-stage cervical cancers that require only intracavitary irradiation, a combination of intracavitary and extracorporeal irradiation is needed to form an effective treatment with a more uniform dose distribution within the target area of the cervical cancer. The total duration of radiation therapy is limited to 8 weeks as much as possible.
- style=”margin-left: 54pt”>
- Radiotherapy Complications
The probability and severity of radiation therapy complications vary depending on the type of radiation source, radiation method, irradiation area, irradiation site, unit dose, total dose, total number of fractions, and total treatment time, as well as the patient’s sensitivity to radiation. The probability and severity of radiation therapy complications vary. The patient’s sensitivity to radiation varies.
-
Recent complications: including Complications occurring during and shortly after treatment, such as infection, vaginitis, vulvodynia, dry and wet skin reactions, bone marrow suppression, gastrointestinal reactions, rectal reactions, bladder reactions, and mechanical injury.
-
Distant complications: common include radiation proctitis, radiation cystitis, changes in skin and subcutaneous tissue, changes in reproductive organs, and radioactive small bowel infection, etc. The most common one is radiation proctitis, which mostly occurs 1 ~1.5 years after radiotherapy. The main manifestations are: increased stool frequency, mucus stool, blood in the stool, and in severe cases, rectovaginal fistula. The next common manifestation is radiation cystitis, mostly in 1 year and a half, the main manifestations are frequent urination, painful urination, blood in urine, dyspareunia, and in severe cases, vesicovaginal fistula.
- style=”margin-left: 44pt”>
- Tolerable dose of organ endangerment
Organs at risk for radiation therapy for cervical cancer include the bladder, rectum, colon, bone marrow, skin, small intestine, ureter, etc., and are generally treated with TD< sub>5/5
denotes the minimum radiation tolerance, indicating that the incidence of serious complications does not exceed 5% within 5 years of treatment. span>. Table 5 is the TD5/5 for each organ at risk. - Tolerable dose of organ endangerment

|
Organic |
InjuriesTD5/5 |
irradiated area or length |
skin |
ulcerated, severely fibrotic 55 |
100cm2 |
|
Small intestine |
Ulcer, perforation, bleeding 50 |
100cm2 |
| Colon |
ulcer, stricture 45 |
100cm2 |
|
rectal |
Ulcer, stricture 60 |
100cm2 |
|
Kidneys |
Acute and chronic nephritis20 |
All Kidney |


|
Bladder |
contraction |
60 |
The entire bladder |
|
Ureter |
Narrow |
75 |
5~. /span>10cm |
|
ovaries |
permanent sterility |
2~3 |
The entire ovary |
|
The uterus |
necrosis, perforation |
< span style="font-size:14pt">>100 |
The entire uterus |
|
< span style="font-family:imitation-song; font-size:14pt">vagina |
Ulcers, fistulas |
90 |
All |
|
All |
|||
| Adult skeleton |
necrosis, fracture, sclerosis |
60 |
whole bone or < span style="font-size:14pt">10cm2 |
|
Spinal cord |
Infarction, necrosis |
45 |
10cm |
|
Adult Muscle |
fibrosis |
60 |
Whole Muscle |
| < p>Bone marrow |
Regeneration Defect |
2 |
Bone marrow throughout the body |
|
30 |
local bone marrow |
||
|
Lymph nodes and Lymphatic vessels |
< span style="font-family:imitation-song; font-size:14pt">atrophy, sclerosis |
50 |
whole lymph node |
|
Fetus |
< span style="font-family:imitation-song; font-size:14pt">Death |
2 |
The whole fetus |
|
peripheral nerves |
Neuritis |
60 |
10cm2 |
(iv) Chemotherapy.
The role of chemotherapy in the treatment of cervical cancer is gaining increasing attention and should be used mainly for radiotherapy sensitization with radiotherapy alone or in combination with chemotherapy, i.e. simultaneous radiotherapy and chemotherapy. In addition, there is also preoperative neoadjuvant chemotherapy and palliative treatment for patients with advanced distant metastases and recurrence. Treatment
The effective drugs for cervical cancer are cisplatin, paclitaxel, 5- fluorouracil, isocyclophosphamide, gemcitabine, and topotecan.
- style=”margin-left: 62pt”>
- Synchronous radiotherapy
Chemotherapy administered concurrently with radiotherapy, also known as sensitization chemotherapy. The current NCCN treatment guidelines recommend sensitization chemotherapy with a platinum-containing regimen during radiation therapy, with cisplatin being the preferred treatment of choice: 30to40mg/m2 per week 1. Roman”>1 time. Cisplatin toxicity intolerance can be replaced with carboplatin. There are also clinical studies with cisplatin combination regimens for concurrent chemotherapy: cisplatin 50 to 70 mg/m2, paclitaxel 135~175mg/m m2, radiotherapy for the first 1 and 1 and 29 days. Cisplatin + paclitaxel weekly therapy: cisplatin 25 to 30 mg/m2, paclitaxel 60 to 80mg/m2, radiotherapy for the first 1, 1, < span style="font-family:Times New Roman">8, 15, 15, 22 Roman”>22, 29 and 36 days. Dose adjustments need to be made based on the patient’s adverse reactions to radiotherapy.
The overall principle is not to interfere with the normal course of radiotherapy.
- style=”margin-left: 54pt”>
- Neoadjuvant chemotherapy
Neoadjuvant chemotherapy is when a patient undergoes 2 to 2 prior to surgery. family:Times New Roman”>3 courses of chemotherapy before surgery with the aim of reducing tumor size, eliminating micrometastases and subclinical lesions, and allowing patients who were previously inoperable to have surgery. Some non-randomized studies have shown that neoadjuvant chemotherapy reduces the probability of intraoperative dissemination and postoperative metastases. Currently, it is used primarily for early-stage patients with large localized tumors. Neoadjuvant chemotherapy regimens are often platinum-based combinations, such as cisplatin + paclitaxel, PVB regimens (cisplatin +vincristine + bleomycin), BIP regimens (cisplatin + bleomycin + isophosphamide +) (cyclophosphamide + mesylate sodium), etc. Routes of administration include intravenous systemic chemotherapy or arterial cannulation interventional chemotherapy. Paclitaxel +cisplatin is currently the most commonly used.
- style=”margin-left: 54pt”>
- Systemic chemotherapy
Primarily for patients with recurrent or metastatic cervical cancer who cannot be treated with either surgery or radiation.
2020 NCCN span>First-line recommended by cervical cancer treatment guidelines for recurrent or metastatic cancer
The chemotherapy regimens are: cisplatin in combination with paclitaxel, cisplatin in combination with paclitaxel and bevacizumab, paclitaxel in combination with topotecan and bevacizumab as a recommended regimen, and carboplatin in combination with paclitaxel and bevacizumab as a recommended regimen for patients who have received cisplatin. In addition, cisplatin in combination with topotecan and topotecan in combination with paclitaxel are also alternative regimens. The first-line single-agent chemotherapy options are carboplatin, cisplatin, and paclitaxel.
From 2018 the NCCN span>guidelines in second-line treatment of cervical cancer after failure of first-line therapy, pablizumab is first recommended for PD-L1 positive or highly microsatellite unstable / mismatch repair-deficient tumors, studies have shown objective remission rates of 14.3% and complete remission rates of 2.6%, and 91% of patients were in remission for more than six months.
2021 Keynote-826 (NCT03635567) results found that in first-line treated PD-L1 positive cervical cancer patients with chemotherapy ± bevacizumab compared with chemotherapy ± bevacizumab reduced the risk of patient death by 36% and significantly prolonged overall survival and progression-free survival, based on which the FDA approved pabrolizumab
+ chemotherapy ± bevacizumab in PD-L1 positive [ combined positive score (combined positive score, CPS) ≥ 1] for first-line treatment of recurrent or metastatic cervical cancer. second-line chemotherapeutic agents are: bevacizumab, doxorubicin, albumin-bound paclitaxel, gemcitabine, epi-amycin, 5-fluorouracil, isocyclic phosphoadenamide, irinotecan, mitomycin, pemetrexed, topotecan, and vincristine.
Multiple studies of immune checkpoint inhibitors in combination with targeted agents, chemotherapy, or radiation therapy are currently in clinical trials, and more clinical data are needed to support the use of these drugs in combination.
V. Follow up
For new cervical cancer patients, a complete case and related data file should be established, and treatment
Regular follow-up monitoring after treatment.
Every 2 years after the end of treatment: Times New Roman”>3 months 1 and the first 3 to 5 months every 6 years 1 times and then 1 times per year.Stage II patients are treated 3 to 6 months after treatment, a whole-body MRI or CT to assess pelvic tumor control and, if necessary, 5 years, depending on the patient’s condition.
Regular vaginal douching after radiation therapy, use of vaginal dilators if necessary, and early resumption of sexual intercourse are all helpful in reducing vaginal adhesions.
Attachment 1: Abbreviations
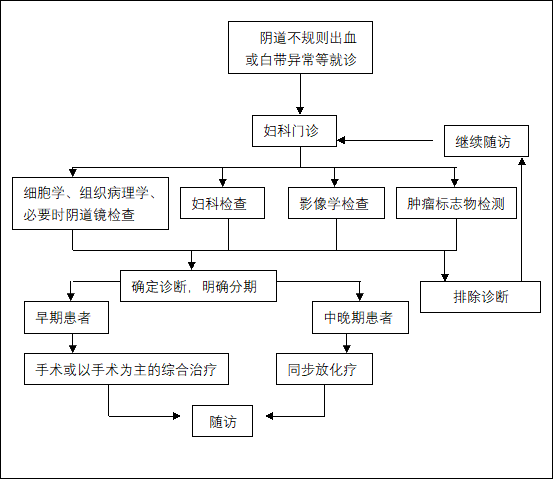
Attachment 2: Cervical Cancer Diagnosis and Treatment Process
Attachment 1
Abbreviations
CA: (carcinoma antigen)cancer antigen125 CEA: (carcinoembryonic antigen)carcinoembryonic antigenCIN: (cervical intraepithelial neoplasia)cervical intraepithelial neoplasiaCTV: (clinical target volume) clinical target area
FIGO: (International Federation of Gynecology and ObstetricsInternational Federation of Gynecology and ObstetricsHR-CTV: (high risk clinical target volume) high risk clinical target area (for brachytherapy) LVSI: (Lymph-vascular space invasion) lymphovascular space invasion
NCCN: (National Comprehensive Cancer Network) National Comprehensive Cancer Network NSRH: (Nerve-sparing radical hysterectomy) Nerve-preserving radical hysterectomyPTV: (planning target volume) planned target area
SCC: (squamous cancinoma-associated antigen) squamous carcinoma-associated antigen
Annex 2
Cervical Cancer Diagnosis and Treatment Process
Attachment 3
Cervical Cancer Treatment Guidelines (2022 Edition) Development and Validation Expert Group
(in surname stroke order)
Team leader: Martin
Members: Hua Keqin, Xiang Yang, Liu Congrong, Liu Aijun, Li Bin, Wu Xiaohua, Wu Lingying, Zhang Fuquan, Chen Yan, Lin Zhongqiu, Zhou Qi, Lang Jinyi, Lou Ge, Yao Shuzhong, Yuan Guangwen, Huang Manni, Dong Mei