Myelodysplastic Syndrome with Primordial Cellularity
(MDS-EB) Guideline
(2022 Edition)
Myelodysplastic syndromes (MDS) are a group of heterogeneous myeloid clonal disorders of hematopoietic stem cell origin characterized by abnormal development of myeloid cells. MDS is a group of heterogeneous myeloid clonal disorders of hematopoietic stem cell origin characterized by abnormal myeloid cell development, manifested by ineffective hematopoiesis, refractory hematocrit, and a high risk of transformation to acute myelogenous leukemia (AML).
The diagnostic and staging criteria for MDS have been refined over the past 40 years since they were first established by the FAB Collaborative Group in 1982. The subtype MDS with excess blasts (MDS-EB) is defined as a subtype of MDS with 5 ~19
~19  , with a further increased risk of transition to AML than other subtypes.
, with a further increased risk of transition to AML than other subtypes.
II, Diagnostic Techniques and Applications
The global incidence of MDS is approximately (2-12)/100,000, and the incidence in China is
(0.23 to 1.51)/100,000. The incidence of MDS increases with age, with 80 Age of onset is >60 years. MDS is more common in men than in women, with a prevalence of 33.9 per 100,000 men and 18 per 100,000 women in the German population aged ≥70 years, and a ratio of 1.8:1 in men to women in the Swedish population.
Age of onset is >60 years. MDS is more common in men than in women, with a prevalence of 33.9 per 100,000 men and 18 per 100,000 women in the German population aged ≥70 years, and a ratio of 1.8:1 in men to women in the Swedish population.
The clinical manifestations of MDS-EB are nonspecific, with a predominance of allogeneic cytopenias, often
Significant anemia, hemorrhage, and infections may be associated with splenomegaly, often progressing to acute leukemia within a short period of time, with a conversion rate of up to 40 , and some patients do not progress to acute leukemia but often die from infection and bleeding.
, and some patients do not progress to acute leukemia but often die from infection and bleeding.
The diagnosis of MDS relies on a combination of laboratory testing techniques, of which bone marrow aspiration smear cytomorphology and cytogenetic testing techniques are central to the diagnosis of MDS.
- Bone marrow aspiration smear: Morphologic abnormalities in peripheral blood and bone marrow smears of MDS patients are divided into 2 categories: increased percentage of primitive cells and abnormal cell development. Primitive cells can be divided into 2 types: type 1 (EB-1) are primitive cells without asplenophilic granules; type 2 (EB-1) are primitive cells with asplenophilic granules but without paranuclear halo area, and those with paranuclear halo area are judged as early juvenile granulocytes. In a typical patient with MDS, abnormal developmental cells account for ≥10
 of the cells of the appropriate lineage. All patients with proposed MDS should have a bone marrow iron stain to count ringed iron-granulated juvenile erythrocytes, defined as those with more than 5 blue granules in the cytoplasm of the juvenile erythrocytes and more than 1/3 of the circumference around the nucleus.
of the cells of the appropriate lineage. All patients with proposed MDS should have a bone marrow iron stain to count ringed iron-granulated juvenile erythrocytes, defined as those with more than 5 blue granules in the cytoplasm of the juvenile erythrocytes and more than 1/3 of the circumference around the nucleus. -
Bone marrow biopsy pathology: All patients with suspected MDS should undergo a bone marrow biopsy, usually at the posterior superior iliac spine, of at least 1.5 cm in length. Bone marrow biopsy cytology helps to exclude other factors or diseases that may contribute to hematocrit and provides important information on the degree of marrow cell proliferation, megakaryocyte count, primitive cell population, degree of myelofibrosis, and tumor marrow metastasis. Patients with suspected MDS should undergo Gomori silver staining and in situ immunohistochemistry, and commonly used markers include CD34, MPO, GPA, CD61, CD42, CD68, CD20
and CD3.
-
Karyotype analysis: All patients with suspected MDS should undergo karyotype testing, usually for ≥20 mid-phase divisions of bone marrow cells, and karyotyping in accordance with the International System for the Nomenclature of Human Cytogenetics (ISCN) 2013. (40
 to 60
to 60  of MDS patients have non-random chromosomal abnormalities, with +8, -7/del (7q), del (20q), -5/del (5q), and -Y being the most common. Some of the common chromosomal abnormalities in patients with MDS are of diagnostic value: (i) unbalanced chromosomal abnormalities: -7/del (7q); del (5q); (i17q)
of MDS patients have non-random chromosomal abnormalities, with +8, -7/del (7q), del (20q), -5/del (5q), and -Y being the most common. Some of the common chromosomal abnormalities in patients with MDS are of diagnostic value: (i) unbalanced chromosomal abnormalities: -7/del (7q); del (5q); (i17q)/t(17p); -13/del(13q); del(11q); del(12p)/t
(12p); del(9q); idic(X)(q13). (ii) Balanced chromosome abnormalities: (t11;16)(q23.3;p13.3); (t3;21)(q26.2;q22.1).
(t1;3)(p36.3;q21.2); (t2;11)(p21;q23.3); inv
(3)(q21.3;q26.2)/t(3;3)(q21.3;q26.2); (t6;9)
(p23;q34.1). And +8, del(20q) and -Y can also be seen in aplastic anemia and other hemocytopenic disorders. Patients who do not meet the morphologic criteria (<10
 of 1 or more lineage cell developmental abnormalities), but who also have persistent Patients with persistent hematocrit who have cytogenetic abnormalities of diagnostic value for MDS should be diagnosed as MDS-Unclassified (MDS-U).
of 1 or more lineage cell developmental abnormalities), but who also have persistent Patients with persistent hematocrit who have cytogenetic abnormalities of diagnostic value for MDS should be diagnosed as MDS-Unclassified (MDS-U). -
Fluorescence in situ hybridization: application of a set of probes for common abnormalities of MDS for Fluorescence in situ hybridization (FISH) can improve the detection rate of cytogenetic abnormalities in some MDS patients. Therefore, for those with suspected MDS, bone marrow stem aspiration, no intermediate
FISH should be performed in suspected MDS patients with dry bone marrow aspirations, no mid-stage divisions, or <20 analyzable mid-stage divisions. CEP7, 7q31, CEP8, 20q, CEPY, and TP53.
-
Bone marrow flow cytometry: there are no MDS-specific antigenic markers or combinations of markers. The diagnosis of MDS cannot be made on the basis of flow cytometry results alone in patients who lack diagnostically definitive cytomorphologic or cytogenetic manifestations. However, flow cytometry has applications for prognostic stratification of MDS.
-
Mutation detection: Next-generation gene sequencing technologies can detect at least 1 mutation in the vast majority of patients with MDS. Common mutations in MDS include TET2, RUNX1, ASXL1, DNMT3A, EZH2, SF3B1, etc. Some
Mutation status of genes is valuable for differential diagnosis and risk stratification of MDS and is recommended as an elective test, including: TP53, TET2, DNMT3A, IDH1/2, EZH2, ASXL1, SRSF2, RUNX1, U2AF1, SETBP1, etc.
Primary cellularity is the main diagnostic criterion for MDS-EB.
- style=”margin-left: 48pt”>
- MDS-EB-1: bone marrow 5
 ~9
~9  or peripheral blood 2
or peripheral blood 2 ~4 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0955_12.png" alt=""/>, no Auer small
~4 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0955_12.png" alt=""/>, no Auer small
- MDS-EB-1: bone marrow 5
Body.
- style=”margin-left: 61pt”>
- MDS-EB-2: Bone Marrow 10
 ~19
~19 or peripheral blood 5
or peripheral blood 5 ~19< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0955_16.png" alt=""/>or with Auer
~19< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0955_16.png" alt=""/>or with Auer
Small bodies.
(v) Prognostic stratification.
Common risk stratification systems for patients with MDS include the International Prognostic Scoring System
(international prognostic score system, IPSS), WHO
the WHO adapted prognostic scoring system (WPSS) and the revised international prognostic scoring system (IPSS-R). In addition, the MD Anderson Cancer Center (MDACC) stratification system introduced parameters such as age and physical status in addition to the usual primary parameters.
1. IPSS: The grading of IPSS risk was developed in 1997 and was determined based on 3 factors: the proportion of bone marrow primitive cells, the degree of hematocrit, and the cytogenetic characteristics of the bone marrow. Bone marrow progenitor cells 5 to 10
to 10  (EB-1) score of 0.5.
(EB-1) score of 0.5.
Bone marrow primitive cells 11 ~20
~20 (EB-2) Points 1.5. 2. WPSS: developed in 2007, erythrocyte infusion-dependent and iron overload not only leads to
(EB-2) Points 1.5. 2. WPSS: developed in 2007, erythrocyte infusion-dependent and iron overload not only leads to
Organ damage can also directly impair hematopoietic function, which may affect the natural course of MDS patients. As a time-continuous evaluation system, prognosis can be assessed at any point in the patient’s disease course. Bone marrow primitive cells 5 to 10
to 10  (EB-1) score of 2.
(EB-1) score of 2.
Bone marrow primitive cells 11 ~20
~20 (EB-2) Score 3.
(EB-2) Score 3.
3. IPSS-R: The IPSS-R scoring system is considered the gold standard for prognostic assessment of MDS and is the latest version of the IPSS prognostic scoring system revised by the International Task Force on MDS Prognosis in 2012, and its validity for assessing prognosis is It is significantly better than IPSS and WPSS.2 
 ~10
~10  (EB1) score 2, bone marrow primitive cells >10
(EB1) score 2, bone marrow primitive cells >10  (EB-2) score 3 points. However, IPSS-R also has its limitations. Whether its prognostic assessment
(EB-2) score 3 points. However, IPSS-R also has its limitations. Whether its prognostic assessment
applicable to patients treated with chemotherapy or targeted agents remains unknown; furthermore, other factors with independent prognostic significance are not included, such as infusion dependence of red blood cells, genetic mutations, and especially genetic mutations may contribute to a more precise prognostic assessment.
The treatment of MDS should be based on the prognostic grouping of patients with MDS, as well as a comprehensive analysis of the patient’s age, physical status, co-morbidities, and adherence to treatment, etc. MDS can be divided into 2 groups according to the prognostic score system. The lower risk group [IPSS low risk group, intermediate risk-1 group, IPSS-R very low risk group, low risk group, and intermediate risk group (≤
-
score), WPSS very low risk, low risk and intermediate risk groups] and higher risk groups [IPSS intermediate risk-2 group, high risk group, and MDS-EB stage patients with reduced blood counts are basically in the higher risk group, and their treatment goals are to delay disease progression, prolong survival, and cure.
The primary goal of supportive care is to improve the patient’s quality of life. In patients with MDS-EB, this includes component transfusions: red blood cell transfusions are usually given when hemoglobin is <60 g/L or when there are significant anemia symptoms. In elderly patients, with limited compensatory capacity and increased oxygen demand, red blood cell transfusion is recommended for hemoglobin ≤ 80 g/L. Platelet transfusion should be given if the platelet count is <10×109/L or if there is active bleeding.
Commonly used demethylating drugs include 5-azacitidine (azacitidine.
AZA) and 5-aza-2′-deoxycytidine (decitabine). In the higher-risk group of MDS patients, demethylating drugs reduced the risk of progression to AML and improved survival compared with the supportive care group.
-
AZA: recommended use is 75 mg/m2 daily< span style="font-family:Times New Roman">×7 days by subcutaneous injection for 28 days. The median time to first treatment response in patients with MDS treated with AZA was 3 treatments, with approximately 90
 Treatment response was achieved within 6 courses in patients with effective treatment. Therefore, it is recommended that patients with MDS be evaluated for treatment response after 6 courses of AZA therapy and that effective patients continue to be treated.
Treatment response was achieved within 6 courses in patients with effective treatment. Therefore, it is recommended that patients with MDS be evaluated for treatment response after 6 courses of AZA therapy and that effective patients continue to be treated. -
Decitabine: The recommended regimen is 20 mg/m2 daily×5 days every 4 weeks. It is recommended that patients with MDS receive decitabine for 4 to 6 courses to evaluate treatment response and that effective patients continue.
Patients with MDS-EB in higher-risk groups, especially those with an increased proportion of primitive cells, have a poor prognosis, and chemotherapy is one of the treatment modalities for patients selected for non-hematopoietic stem cell transplantation (HSCT). The standard 3+7 induction regimen for AML or the prestimulation regimen can be adopted. The prestimulation regimen is widely used in China for higher-risk MDS patients and consists of low-dose cytarabine (10 mg/m2 subcutaneously every 12 hours for 14 days) in combination with granulocyte colony-stimulating factor and aclarubicin or hypertrigonelline or desoxorubicin. Pre-excitation regimens for higher-risk MDS patients have achieved complete remission rates of up to 40
 ~
~60
 , and in older or less able patients. and older or less able patients tolerate prestimulation regimens better than conventional AML chemotherapy regimens. Pre-excitation regimens can also be combined with demethylating drugs.
, and in older or less able patients. and older or less able patients tolerate prestimulation regimens better than conventional AML chemotherapy regimens. Pre-excitation regimens can also be combined with demethylating drugs.
The combination of BCL-2 inhibitors [(Venetoclax (VEN)], immune checkpoint inhibitors (programmed death protein-1 inhibitors, etc.), oral histone deacetylase inhibitors, and CD47 monoclonal antibodies for demethylation in the treatment of high-risk MDS has yielded initial promising results. The future has the potential to improve the overall prognosis of patients with MDS-EB.
(E) Allogeneic hematopoietic stem cell transplantation.
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is currently the only cure for MDS. The indications for allo-HSCT are: (i) patients <65 years of age in the higher risk group for MDS; (ii) patients <65 years of age with severe hematocrit, who have failed other treatments, or who have poor prognostic genetic abnormalities
(e.g., -7, 3q26 rearrangements, TP53 mutations, complex karyotypes, haplotypes) in the lower-risk group. Patients with MDS-EB to undergo allo-HSCT may be treated with chemotherapy or demethylating agents or a combination of both to bridge allo-HSCT while awaiting transplantation, but transplantation should not be delayed.
Based on the internationally standardized efficacy criteria proposed by the International Working Group (IWG) on MDS in 2000 and revised in 2006, the response to treatment for MDS includes the following four categories.
(i) Modification of the natural course of the disease.
- style=”margin-left: 54pt”>
- Complete remission: bone marrow: primitive cells ≤5
 and all cell lines are maturing positively
and all cell lines are maturing positively
normal. Peripheral blood: primitive cells were 0, hemoglobin ≥110 g/L, neutrophils ≥1.0×109/L, platelets ≥100×109/L.
-
Partial remission: absolute peripheral blood values must persist for at least 2 months and all other criteria for complete remission are met (anyone with pre-treatment The patient must be in partial remission: absolute peripheral blood values must be in complete remission for at least 2 months (all other criteria are met for those with pre-treatment abnormalities), but the bone marrow progenitor cells are only reduced by ≥50
 compared to pre-treatment, but still >5
compared to pre-treatment, but still >5 , regardless of the degree of myeloid proliferation and morphology.
- Bone marrow CR: bone marrow: primitive cells ≤5
 and ≥50 reduction from pre-treatment
and ≥50 reduction from pre-treatment  ; Peripheral blood: if hematologic improvement is achieved, this should be noted as well.
; Peripheral blood: if hematologic improvement is achieved, this should be noted as well. - Disease stabilization: minimum criteria for partial remission not met but no evidence of disease progression for at least 8 weeks.
-
Failure: death or disease progression during treatment as evidenced by increased hematocrit, increased bone marrow primitive cells, or progression to more progressive Fibroblast than before treatment. The disease may develop into a more progressive FAB subtype than before treatment.
-
Progression: primitive cells <5
 People: primitive cell increase ≥50
People: primitive cell increase ≥50  up to 5
up to 5 ; Primordial cells 5
; Primordial cells 5  to 10
to 10  those with ≥50 increase in primordial cells
those with ≥50 increase in primordial cells  up to 10
up to 10 ; primitive cells 10
; primitive cells 10 to 20
to 20  People: ≥50 increase in primitive cells
People: ≥50 increase in primitive cells  up to 20
up to 20 ; peripheral blood: neutrophils or platelets decreased ≥ 50 percent from optimal remission/therapy
; peripheral blood: neutrophils or platelets decreased ≥ 50 percent from optimal remission/therapy  ; hemoglobin decline ≥ 20 g/L; transfusion dependent.
; hemoglobin decline ≥ 20 g/L; transfusion dependent.- style=”margin-left: 48pt”>
- Complete reaction: disappearance of chromosomal abnormalities and no new abnormalities.
- Partial response: reduction in the proportion of chromosomally abnormal cells by ≥50
 .
.
(iii) Hematologic improvement.
- style=”margin-left: 48pt”>
- Red system reaction (pre-treatment hemoglobin <110 g/L): hemoglobin
- Complete reaction: disappearance of chromosomal abnormalities and no new abnormalities.
Elevated ≥15 g/L; decreased red blood cell transfusion, at least 4 U per 8-week infusion compared to pretreatment; only pretreatment hemoglobin ≤90 g/L and requiring red blood cell transfusion were included in the red blood cell transfusion efficacy assessment.
-
Platelet response (pre-treatment platelets <100×10< span style="font-size:8pt">9/L): pre-treatment platelets > 20× 1099/L before treatment, the net value added is ≥ 30× 109/L or increases from < 20× 109/L to > 20× 109/L and at least increase by 100
 .
. -
Neutrophil response (pre-treatment) Neutrophils <1.0×109/L): increased 100
 above and absolute value increment >0.5×109/L.
above and absolute value increment >0.5×109/L. -
Progression or relapse after hematologic improvement: at least 1 of the following: neutrophil granulocyte or platelet decline ≥ 50
 , hemoglobin decline ≥ 15 g/L, transfusion dependent .
, hemoglobin decline ≥ 15 g/L, transfusion dependent .(iv) Improving the quality of survival.
using various questionnaires or the WHO Physical Fitness Score.
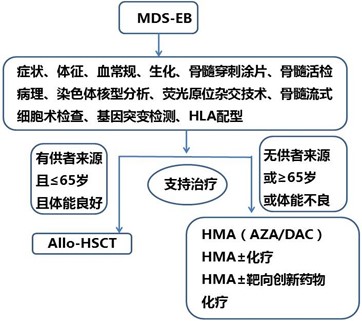
Diagnostic and Treatment Process for MDS-EB Patients
 < span style="font-size:10pt">
< span style="font-size:10pt">
Myelodysplastic Syndrome with Primordial Cellularity
(MDS-EB) Guideline (2022 Edition)
Writing Validation Expert Group
Team leader:Huang Xiaojun
Members:Jing Wang, Haixia Fu, Lanping Xu, Qian Jiang, Hao Jiang, Xiaohui Zhang, Shenmiao Yang, Yuanyuan Zhang, Jin Song Jia, Xiaojun Huang, Jin Lu