Chronic Myeloid Leukemia Treatment Guidelines
(2022 Edition)
Chronic myelogenous leukemia (CML) is a malignant disease of hematopoietic stem cells that is predominantly myeloproliferative.  ~20
~20  , occurring in all age groups; the incidence increases with age, and the median age of diagnosis is younger (40-50 years) in Asian countries and older in Europe and the United States.
, occurring in all age groups; the incidence increases with age, and the median age of diagnosis is younger (40-50 years) in Asian countries and older in Europe and the United States.
(55-65 years), with a male-to-female ratio of approximately 1.4:1 and a natural course of 3 to 5 years, the use of tyrosine kinase inhibitors (TKI) has revolutionized the course of CML. The use of tyrosine kinase inhibitors (TKI) has revolutionized the course of CML, and for the vast majority of patients, CML has become a chronic, controllable tumor.
CML is highly suspected if the patient presents with increased white blood cells (WBC) or splenomegaly and myeloid immature cells in the peripheral blood. the presence of a positive Ph chromosome and/or BCR-ABL fusion gene is necessary for the diagnosis of CML.
When CML is suspected, the patient needs to be noted for a history of other diseases (e.g., infection, autoimmune disease), history of specific medications, pregnancy, or stressful conditions. If increased WBCs are not explained by a leukemia-like response, cytogenetic and molecular studies are needed.
Cytogenetic and molecular tests are needed to identify diseases such as CML or other myeloproliferative neoplasms. 1. Leukoid response: seen in infections, drugs, pregnancy, malignancies, and
stress states, etc.
There are clinical manifestations associated with the primary disease. Ph chromosome and BCR-ABL fusion gene were both negative.
2. Myeloproliferative neoplasm.
- True erythrocytosis: Erythrocytosis is the most prominent manifestation, accompanied by hyperviscosity due to erythrocytosis, and most clinical manifestations such as splenomegaly; leukocytosis is mildly increased, but usually does not exceed 50×10. The white blood cells are mildly increased, but usually do not exceed 50×109/L. There is also a mild increase in platelets, and the red blood cell volume significantly exceeds normal values. Neutrophil alkaline phosphatase was high, Ph chromosome or BCR-ABL fusion gene was negative, and 95

Patients were detected with the JAK2V617F mutation. -
Primary thrombocythemia: significant thrombocythemia ≥450× 109/L, proliferation of large, mature megakaryocytes in the bone marrow, detectable JAK2, CARL or MPL mutations or other clonal abnormalities markers, but Ph chromosome and BCR-ABL fusion gene were negative.
-
Myelofibrosis: Significant proliferation of reticular fibers and collagen in the bone marrow, proliferation of megakaryocytes in the bone marrow with heterogeneity, and detection of JAK2, CARL, or MPL mutations or other clonal abnormalities. Myelofibrosis: significant proliferation of reticulocytes and collagen in the bone marrow with heteroplasmy, detectable JAK2, CARL or MPL mutations or other clonal abnormalities, but negative for Ph chromosome and BCR-ABL fusion genes.
The disease process of CML is generally divided into 3 phases: the chronic phase (CP), the accelerated phase (AP), and the acute phase
(blast phase, BP). Most patients with CML are in CP at the time of presentation and often have an insidious onset, with about 20 to 40
to 40 of patients are asymptomatic, with increased white blood cell counts found on routine examination, and may also present with fatigue, weight loss, night sweats, splenomegaly, anemia, or thrombocytosis. Most patients with CP progress to progressive (AP and BP) CML within 3 to 5 years of the natural course of the disease, and progression is accompanied by worsening of the clinical picture and associated symptoms of severe anemia, thrombocytopenia, and splenomegaly. Approximately 70
of patients are asymptomatic, with increased white blood cell counts found on routine examination, and may also present with fatigue, weight loss, night sweats, splenomegaly, anemia, or thrombocytosis. Most patients with CP progress to progressive (AP and BP) CML within 3 to 5 years of the natural course of the disease, and progression is accompanied by worsening of the clinical picture and associated symptoms of severe anemia, thrombocytopenia, and splenomegaly. Approximately 70
BP patients transition to acute myeloid leukemia, and 20  to 30
to 30 to acute lymphoblastic leukemia. The staging criteria for CML are shown in Table 1.
to acute lymphoblastic leukemia. The staging criteria for CML are shown in Table 1.

Table 1.
 Staging WHO Standard
Staging WHO Standard
Chronic stage Not meeting criteria for diagnosis of accelerated or acute stage
 Acceleration phase (1) Primitive cells in peripheral blood and/or bone marrow nucleated cells account for 10
Acceleration phase (1) Primitive cells in peripheral blood and/or bone marrow nucleated cells account for 10 ~19 (2) peripheral blood basophils ≥20
~19 (2) peripheral blood basophils ≥20 
- style=”margin-left: 73pt”>
-
Non-treatment-related platelet reduction (<100×109/L) or treatment-uncontrolled persistent thrombocytosis (>1000×109/L)
- Progressive splenomegaly and increased white blood cell count uncontrolled by treatment
- Progressive splenomegaly and increased white blood cell count uncontrolled by treatment
-
Phase of rapid evolution of cytogenetic clones other than the Philadelphia chromosome during treatment Consistent with at least 1 of the following indicators.
- style=”margin-left: 92pt”>
Primary cells in peripheral blood leukocytes or bone marrow nucleated cells ≥20

- style=”margin-left: 108pt”>
- Extra-medullary primitive cell infiltration
 Bone marrow biopsy showing large patches or focal primitive cells
Bone marrow biopsy showing large patches or focal primitive cells
Note: Primitive cells in WHO criteria can be of myeloid origin (including neutrophils, eosinophils, basophils, monocytes, erythroids, megakaryocytes For the few cases where the origin of the primary cells is morphologically indistinguishable, immunophenotyping is recommended for confirmation; lamellar and clustered megakaryocytic proliferation with significant reticulin or collagen fibrosis and/or severe granulocytic dysplasia suggest an accelerated phase. These phenomena are often accompanied by other features of the accelerated phase and have not been used as an independent diagnostic basis.
(ii) Disease risk for CP patients.
Currently, the commonly used scoring systems are Sokal and ELT (S EUTOS long term).
survival) scores, both of which use clinical indicators as predictors of survival associated with CML, are calculated as shown in Table 2. The study showed that the ELTS score, with a lower age weighting than Sokal, was more accurate in predicting long-term outcomes in the high-risk group. Regardless of the scoring system, high risk predicts poor response to treatment and shorter survival, and warrants closer monitoring of outcomes and more aggressive treatment.

Table 2. Sokal and ELTS integral formulas
|
Formula Low Risk |
Medium Risk |
High Risk |
|
|
Sokal points |
|||
|
Exp[0.0116×(age-43.4)]+0.0345× <0.8 |
0.8 to 1.2 |
>1.2 |
|
|
(spleen size – 7.51) + 0.188 x [(platelets
/700 ) 2< -0.563]+0.0887 × (original cells |
|||
|
-2.10) | |||
|
ELTS Points < |
|
0.0025 x (age/10)3 + 0.0615 x splenomegaly ≤1.5680 |
1.5680 |
~ >2.2185 |
|
Small +0.1052× peripheral blood primitive cells +0.4104× |
2.2185< |
|
|
(platelet count/1000)-0.5 |
Note: Platelet units are ×109/L, age in years, spleen size in centimeters below the rib cage, and primitive cells as a percentage of the peripheral blood classification. All data should be obtained before the start of any CML-related treatment.
More than 85 Patients with the disease are in the chronic phase at the time of onset, and some are asymptomatic, with routine blood abnormalities or splenomegaly detected on physical examination or by chance. Typical symptoms include fatigue, low-grade fever, night sweats, left upper abdominal distention, and weight loss. On examination, an enlarged spleen may be palpable or an abdominal ultrasound may show splenomegaly. If the disease is in an accelerated or acute phase, it worsens and is often accompanied by unexplained fever, bone pain, and progressive enlargement of the spleen.
Patients with the disease are in the chronic phase at the time of onset, and some are asymptomatic, with routine blood abnormalities or splenomegaly detected on physical examination or by chance. Typical symptoms include fatigue, low-grade fever, night sweats, left upper abdominal distention, and weight loss. On examination, an enlarged spleen may be palpable or an abdominal ultrasound may show splenomegaly. If the disease is in an accelerated or acute phase, it worsens and is often accompanied by unexplained fever, bone pain, and progressive enlargement of the spleen.
WBC increase, which may be accompanied by decreased hemoglobin or thrombocytosis. Immature granulocytes, basophils and eosinophils are seen in the peripheral blood leukemia classification.
Extremely active proliferation, predominantly of the granulocytic lineage, which may be accompanied by proliferation of the megakaryocytic lineage and relatively depressed proliferation of the red lineage.
Karyotyping by revealed banding method, with Ph chromosomes visible.
Peripheral blood or bone marrow specimens were tested by reverse transcription polymerase chain reaction (RT-PCR) to confirm the presence of the BCR-ABL fusion gene. If the BCR-ABL fusion gene is negative, myeloproliferative neoplasm-associated mutations such as JAK2, CARL, and MPL mutations need to be detected.
After 2000, the first TKI drug, Imatinib Mesylate, was developed and marketed for the BCR-ABL fusion protein, a key target molecule in the pathogenesis of CML. Imatinib mesylate, the first TKI drug to target the BCR-ABL fusion protein in the pathogenesis of CML, opened the era of targeted therapy for CML. Imatinib inhibits BCR-ABL kinase activity relatively specifically, inhibits CML cell proliferation and induces apoptosis in in vitro experiments. The introduction of imatinib significantly improved the survival of CML patients with 80 ~
~
90  of patients had near-normal survival and improved quality of life. Long-term results with imatinib as first-line treatment for patients with primary CML-CP confirmed a 10-year survival rate of 80
of patients had near-normal survival and improved quality of life. Long-term results with imatinib as first-line treatment for patients with primary CML-CP confirmed a 10-year survival rate of 80 to 90
to 90  . The successive introduction of second-generation TKI (e.g., nilotinib, dasatinib, bosutinib, and radolitinib) and third-generation TKI (e.g., ponatinib) has accelerated and improved the response rate and depth of response in patients, effectively overcoming most imatinib resistance and providing more options for imatinib-intolerant patients, making the deadly CML a manageable chronic disease.
. The successive introduction of second-generation TKI (e.g., nilotinib, dasatinib, bosutinib, and radolitinib) and third-generation TKI (e.g., ponatinib) has accelerated and improved the response rate and depth of response in patients, effectively overcoming most imatinib resistance and providing more options for imatinib-intolerant patients, making the deadly CML a manageable chronic disease.
(a) First-line treatment for patients with CP.
The internationally recommended first-line TKI for patients with CP include imatinib, nilotinib, dasatinib, bosutinib, and radolitinib. The drugs recommended in the CML Chinese Diagnostic and Treatment Guidelines (2020 edition) and their uses include imatinib 400 mg/d or nilotinib 600 mg/d or flumatinib 600 mg/d or dasatinib 100 mg/d.
Treatment goals for CML include prolonging survival, reducing disease progression, improving quality of life, and achieving treatment-free remission (i.e., discontinuation). The selection of first-line TKI should be based on the patient’s disease stage and risk, age, coexisting diseases and combination of drugs, based on a clear treatment goal. Patients at intermediate to high risk of disease progression are at higher risk than those at low risk and are suitable for first-line treatment with a second-generation TKI. For young patients who expect to discontinue, second-generation TKI is expected to achieve a rapid deep molecular response (DMR) and reach the threshold for discontinuation. In older patients and those with underlying disease, first-generation TKI have a better safety profile, whereas second-generation TKI-related cardiovascular embolic events, abnormal glucose and lipid metabolism, and pulmonary complications can be lethal and require particular caution.
(ii) Efficacy monitoring during TKI therapy.
Disease monitoring has become an integral component of TKI therapy, not only to assess changes in leukemic load and determine treatment response, but also to help ensure adherence to therapy, detect early drug resistance, predict long-term outcomes, guide individualized therapeutic interventions, and reduce overall treatment costs. Monitoring during TKI therapy includes hematologic, cytogenetic, molecular, and ABL kinase region mutation response analysis.
Hematologic monitoring includes complete blood counts and morphologic analysis of peripheral blood and bone marrow cells to determine disease stage and assess hematologic response. Cytogenetic monitoring includes traditional chromosomal banding (G-banding or R-banding) techniques and fluorescence in situ hybridization (FISH), which looks at the proportion of Ph-positive cells to assess cytogenetic response.
and can identify Ph chromosomal variants and additional abnormalities in Ph-positive (Ph+) or Ph-negative (Ph-) cells, identifying high-risk populations and disease progression. Molecular monitoring uses real-time quantitative reverse transcriptase-mediated PCR (qRT-PCR) to accurately identify BCR-ABL transcript levels in vivo and is the most commonly used and sensitive method to assess CML disease burden with a sensitivity of 0.001 to 0.01
to 0.01  . qRT-PCR is recommended for peripheral blood, which is convenient, minimally painful, reproducible, inexpensive, and has good patient compliance. The recommended method is direct sequencing (Sanger sequencing with a sensitivity of 10
. qRT-PCR is recommended for peripheral blood, which is convenient, minimally painful, reproducible, inexpensive, and has good patient compliance. The recommended method is direct sequencing (Sanger sequencing with a sensitivity of 10 to 20 . img src=”https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0827_20226.png” alt=””/>) or second-generation sequencing targeting the BCR-ABL kinase region to identify point mutations in the ABL kinase region and to identify TKI resistance and guide subsequent treatment choices.
to 20 . img src=”https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0827_20226.png” alt=””/>) or second-generation sequencing targeting the BCR-ABL kinase region to identify point mutations in the ABL kinase region and to identify TKI resistance and guide subsequent treatment choices.
(iii) Treatment response.
Treatment response in CML patients includes hematologic, cytogenetic, and molecular responses, and the criteria are shown in Table 3.

Table 3 Response to treatment in patients with CML
 Response Definition
Response Definition
Hematologic* Complete Hematologic Response (Complete)
hematological response, CHR)
White blood cells <10×109/L Platelets <450×109/L
Peripheral blood without myeloid immature cellsPeripheral blood basophils <5 
No signs or symptoms of extramedullary infiltration, spleen not palpable
Cytogenetics Complete cytogenetic response Ph+ 0


(Complete cytogenetic response, CCyR)
Partial cytogenetic response
(Partial cytogenetic response, PCyR)
Ph+ 1 ~35
~35 
Minor cytogenetic response ( MinorCyR)
Ph+ 36 ~65
~65 
Minor cytogenetic response (Min Imatinib al cytogenetic response , MiniCyR)
Ph+ 66 ~95
~95 
No cytogenetic response (NoCyR)
Ph+>95 
Major cytogenetic response ( MCyR)
Ph+≤35 
Molecular Major molecular reactions (Major
molecular response, MMR) or MR3.0
BCR-ABL ≤ 0.1  (IS)
(IS)
MR4.0 BCR-ABL≤0.01 (IS); or ABL transcription
(IS); or ABL transcription
BCR-ABL is not measurable at >10 000
MR4.5 BCR-ABL ≤ 0.0032 (IS); or ABL to
(IS); or ABL to
BCR-ABL is not measurable for transcripts >32 000


MR5.0 BCR-ABL≤0.001 (IS); or ABL to
(IS); or ABL to
 < span style="font-size:12pt">BCR-ABL is not measurable for recordings >100 000
< span style="font-size:12pt">BCR-ABL is not measurable for recordings >100 000
Note: *, hematologic response required to meet criteria for ≥4 weeks; IS, International scale.
When TKI is used in first-line therapy, patient outcomes are classified by the European LeukmiaNet (ELN) recommendations (2013 version) as best, warning, and failure at important time points based on hematologic, cytogenetic, and molecular monitoring metrics. See Table 4.
Table 4 European LeukmiaNet Recommendations (2013 version)
 Response criteria for first-line tyrosine inhibitor therapy
Response criteria for first-line tyrosine inhibitor therapy
 Best Warning Failure
Best Warning Failure
Baseline NA high risk, or CCA/Ph+, NA major pathway
3 months BCR-ABL ≤ 10
and/ or Ph+≤35
BCR-ABL>10  and/ or Ph+36
and/ or Ph+36  ~95
~95 
No CHR and / or Ph+>95 
6 Months BCR-ABL<1 
and/ or Ph+0
BCR-ABL 1 ~10
~10  and
and
/ or Ph+ 1 ~35
~35 
BCR-ABL>10 
and / or Ph+ >35
12 months BCR-ABL ≤0.1 
BCR-ABL>0.1  ~1
~1 
BCR-ABL>1 
and / or
Ph+ >0
Anytime after BCR-ABL ≤ 0.1
CCA/Ph-(-7 or 7q-) Loss of CHR
Loss of CCyR Confirmation of loss of MMR* mutation


 < span style="font-size:12pt">CCA/Ph+
< span style="font-size:12pt">CCA/Ph+
Note: CCyR, complete cytogenetic response; CHR: complete hematologic response; MMR, major molecular response i.e. BCR-ABL ≤ 0.1  or better; NA, not applicable; *, in 1 of 2 consecutive assays, BCR- ABL transcript levels ≥1
or better; NA, not applicable; *, in 1 of 2 consecutive assays, BCR- ABL transcript levels ≥1  ; CCA/Ph+, clonal chromosomal abnormalities in Ph+ cells. CCA/Ph-, clonal chromosomal abnormalities in Ph- cells.
; CCA/Ph+, clonal chromosomal abnormalities in Ph+ cells. CCA/Ph-, clonal chromosomal abnormalities in Ph- cells.
The ELN recommendations (2020 version) place more emphasis on the molecular response at each time point of
importance, and a common standard for assessing response to first- and second-line TKI therapy. The same idea is that patients who achieve an “optimal” response are predicted to have a durable good outcome and can maintain their therapy; those who achieve “failure” have a significantly increased risk of disease progression and death and need to switch therapy; and “warning” is the gray area in between, where patients need to be monitored closely and switch regimens as soon as the “failure” criteria are met.
(iv) Second-line TKI therapy.
ABL mutation type is the primary indicator for selection of second-line TKI, see Table 5. Only 20 of imatinib-resistant patients  to 50
to 50  ABL mutations are present, and the majority of mutations do not differ or are not known to differ in sensitivity to the two second-generation TKI doses. In such cases, the choice of drug type and dose needs to be based on the patient’s disease stage, age, coexisting disease, and adverse drug reactions. In patients with CP, both dasatinib and nilotinib are available, while in patients with progressive disease, dasatinib is more advantageous. Nilotinib may be more appropriate in patients with pulmonary disease, a history of bleeding, and those receiving NSAIDs. In contrast, dasatinib is more appropriate for patients with pancreatitis and diabetes mellitus. However, for most patients, when there is no clear basis that can guide the choice of dosing, refer to the physician’s opinion on
ABL mutations are present, and the majority of mutations do not differ or are not known to differ in sensitivity to the two second-generation TKI doses. In such cases, the choice of drug type and dose needs to be based on the patient’s disease stage, age, coexisting disease, and adverse drug reactions. In patients with CP, both dasatinib and nilotinib are available, while in patients with progressive disease, dasatinib is more advantageous. Nilotinib may be more appropriate in patients with pulmonary disease, a history of bleeding, and those receiving NSAIDs. In contrast, dasatinib is more appropriate for patients with pancreatitis and diabetes mellitus. However, for most patients, when there is no clear basis that can guide the choice of dosing, refer to the physician’s opinion on
Familiarity with the drug, the patient’s lifestyle, and price are all factors that should be considered in making a choice. Older patients and patients with prior TKI intolerance may be considered for appropriate reduced-dose therapy.

Table 5 Selection of treatment modality according to ABL mutation status
 Mutations Treatment Options
Mutations Treatment Options
T315I ponatinib, hematopoietic stem cell transplant, clinical trial V299L ponatinib, nilotinib
T315A Puneatinib, Nilotinib, Imatinib*, Bosutinib
F317L/V/I/C ponatinib, nilotinib, bosutinib
Y253H, E255K/V, F359C/V/I
Punatinib, Dasatinib, Bosutinib
Any other mutation Puneatinib, Dasatinib, Nilotinib, Bosutinib

Note: *, if it is seen in dasatinib treatment. There are few clinical data on bosutinib against imatinib resistance mutations, and some in vitro data suggest that the E255K/V mutation is not sufficiently sensitive to bosutinib.
(v) No therapeutic remission.
For CML-CP that has achieved a long-term, stable, profound molecular response
Patients discontinuing TKI and pursuing treatment free remission (TFR) could be considered a new therapeutic goal. Although several editions of TFR guidelines have been published in Europe and the United States, many questions remain unanswered. The European Steering Group, composed of hematologists and CML patient advocates (some with discontinuation experience), took patients
centric, aims to guide patients’ treatment choices (including TFR), help build a better patient-physician relationship, and address patients’ emotional and psychological needs. From the unique perspective of the combined patient-physician community, the European Guidance Group has published recommendations for discussion on how to understand and practice TFR, including the following key areas: what is TFR, the appropriate time for TFR, who is or is not eligible for discontinuation, factors for patients to consider when discontinuing medication, discontinuation syndromes, potential patient psychological issues, molecular relapse, and restarting treatment. This is the most comprehensive and actionable comprehensive recommendation to date for CML patients pursuing discontinuation and trying TFR, and is worthwhile for Chinese patients and physicians interested in this area, as shown in Table 6.
Table 6 Comprehensive CML patient-physician discussion from the European Steering Group.
 Recommendations for stopping medication and trying TFR
Recommendations for stopping medication and trying TFR
Treatment goals for CML (1) Early goal is rapid reduction of tumor load or number of leukemias
- style=”margin-left: 145pt”>
- Long-term goal is maximum survival
- style=”margin-left: 145pt”>
- The same quality of life as before the diagnosis of CML
Definition and timing of TFR (1) Definition: TFR refers to a state in which patients who have stopped TKI therapy continue to maintain MMR and do not need to restart therapy
(2) Timing: Patients with chronic phase of CML who continue to achieve stable DMR for at least 2 years can be considered to discontinue and try TFR
Which patients meet the criteria for trying TFR
The following factors need to be considered before attempting TFR.
- style=”margin-left: 38pt”>
- In chronic phase at initial diagnosis
- style=”margin-left: 38pt”>
- Never had resistance to any TKI at any time
- style=”margin-left: 38pt”>
- Attained DMR for at least 2 years
- style=”margin-left: 38pt”>
- Patients should be well informed about TFR and proactively discontinue rather than be pressured to take the medication.


Force
- style=”margin-left: 115pt”>
-
Patients should fully understand that molecular relapse does not mean treatment “failure” and that treatment needs to be restarted at this time
- Molecular monitoring can be repeated in 2 to 4 weeks
- Molecular monitoring can be repeated in 2 to 4 weeks
Which patients are not candidates to try TFR
Patients who have achieved MMR but have not yet reached DMR are not candidates to try TFR!
-
Physicians should ensure that these patients continue treatment and reach their treatment goals or are in a safe harbor to achieve a life expectancy similar to that of the general population!
-
These patients can maintain their original treatment and wait to achieve a deeper molecular response, and as long as they achieve sustained DMR, TFR is likely to be attempted
-
If a patient desires to discontinue or has special needs that require a change in therapy, the physician should communicate with the patient Switching to a 2nd generation TKI to help patients achieve a deeper molecular response
-
Physicians need to inform patients about the side effects of different TKI’s
-
Patients considering stopping TKI therapy
Patients should consider or be aware of the following factors before discontinuing.
- Physicians should emphasize the importance and frequency of follow-up visits, and that patients need more frequent visits
- TFR does not mean that the disease is cured, and molecular relapse can occur at any time and require restart of therapy
- Even if TFR is obtained, physicians should remind patients of the need for ongoing or even lifelong outpatient follow-up and regular monitoring
TKI discontinuation syndrome For patients considering discontinuation, physicians should communicate the TKI discontinuation syndrome and how to manage.
- style=”margin-left: 146pt”>
- Some patients experience musculoskeletal pain after discontinuation and are usually given pain medication


Can
- style=”margin-left: 115pt”>
-
In addition to ongoing disease monitoring, routine outpatient testing can help identify long-term toxicity from prior TKI therapy that can occur even after discontinued can still occur
- Discontinuation syndrome should be monitored and can be treated
- Discontinuation syndrome should be monitored and can be treated
Psychological impact of discontinuation and trying TFR
- Current guidelines are silent on the psychological issues associated with discontinuing TKI and trying TFR therapy
- The guideline group advocates attention to potential psychological problems in TFR patients and routine monitoring, as professional psychological help is necessary for some patients
- Physicians should be aware that fluctuations in BCR-ABL levels during TFR monitoring may cause anxiety in patients
 Molecular Relapse and Restart Therapy
Molecular Relapse and Restart Therapy
Patients should be aware that treatment-free periods last for varying lengths of time, months or years. Physicians should explain the possibility of restarting treatment due to molecular relapse
Note: DMR, deep molecular response i.e. BCR-ABL transcripts ≤0.01 ; MMR, major molecular response i.e. BCR-ABL transcript ≤0.1
; MMR, major molecular response i.e. BCR-ABL transcript ≤0.1 ; TFR, no treatment remission.
; TFR, no treatment remission.
The European Steering Group highlighted factors to consider for patients eligible for TFR
and advocates that patients with CML should be seen at a hospital that offers high-quality, regular molecular monitoring, with specialized CML physicians and psychological support. Although it is uncertain which patients are the best group to try TFR and which factors predict loss of major molecular response after discontinuation, a durable duration of TKI therapy and DMR duration, and regular high-quality molecular monitoring are favorable guarantees of TFR success. Currently, the majority of patients undergoing discontinuation trials and trying TFR are on continuous imatinib therapy, and there is no evidence yet to suggest a difference in the probability of molecular relapse after discontinuation of imatinib and second-generation TKI dosing, ie, imatinib and second-generation TKI discontinuation is obtained
There is no significant difference in the success rate of obtaining TFR, but treatment with second-generation TKI does shorten the time to meet the criteria for discontinuation. As trying TFR becomes a quest and part of disease management for many CML patients, patient concerns about discontinuation will be at the forefront of patient-physician discussions. Therefore, well-informed and more available TFR data will result in more CML patients willing to attempt discontinuation. It is emphasized that adequate communication, the right population, the right timing, and standardized high-quality monitoring and management are necessary for CML patients to pursue TFR success.
(vi) Treatment of patients with progressive disease.
For patients with AP and BP, the recommended initial dose of imatinib is 600 mg/d or 800 mg/d, 400 mg twice daily for nilotinib, and 70 mg twice daily or 140 mg once daily for dasatinib.
For treatment of patients with progressive disease, there were 2 categories: those who had not used a TKI and those who had progressed from CP disease to AP or BP on TKI therapy. All patients with BP and patients with AP who did not achieve optimal response to therapy should be recommended for allogeneic HSCT after achieving a response to TKI or combination chemotherapy.
Appendix 1.
Chronic Myeloid Leukemia Diagnosis and Treatment Flowchart
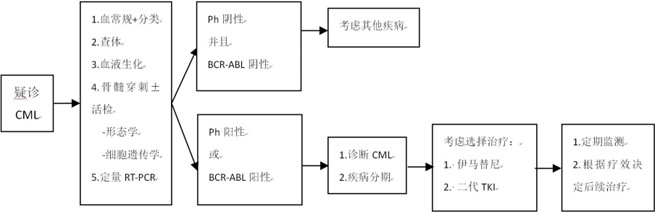
Figure 1. Flow chart of chronic myeloid leukemia diagnosis and treatment
Appendix 2.
Chronic Myeloid Leukemia Guidelines for the Treatment of Chronic Myeloid Leukemia (2022 Edition) Writing and Validation Expert Group
Team leader:Huang Xiaojun
Members: Jing Wang, Haixia Fu, Lanping Xu, Qian Jiang, Hao Jiang, Xiaohui Zhang, Shenmiao Yang, Yuanyuan Zhang, Jin Song Jia, Xiaojun Huang, Jin Lu