Esophageal Cancer Treatment Guidelines
(2022 Edition)
I. Overview
Esophageal cancer has been one of the common malignancies worldwide, and according to the global cancer incidence in 2020 is expected to increase from 1,000 to 1,000.
The number of new cases of esophageal cancer reached 604,000 and the number of deaths reached 54.4 million. Although the incidence and mortality rate of esophageal cancer in China are decreasing, it is still the main malignant tumor threatening the health of Chinese residents. According to the 2015 Chinese malignant
tumor prevalence estimates, new cases of esophageal cancer in China were 246,000 and the crude incidence of esophageal cancer in China 17.8/100 million, the urban crude incidence rate is 12.6/100 million, and the rural crude incidence rate is 12.6/100 million. The crude incidence rate in rural areas is 24.6/100 million; the death rate of esophageal cancer is 18.8 million, and the crude death rate of esophageal cancer in China is 13.7/100 million, urban crude death rate 10.0/100 million, rural crude death rate 18.4/100 million, the incidence and mortality rate ranked 6th and 4th of all malignant tumors, respectively. span>position. There are obvious geographical differences in the incidence of esophageal cancer, with the high incidence areas mainly concentrated in the regions near the Taihang Mountains (Henan, Hebei, Shanxi, Shandong Tai’an, Shandong Jining, Shandong Heze), as well as in Anhui, Jiangsu Subei, Sichuan Nanchong, Sichuan Yanting, Guangdong Shantou, Fujian Minnan, and other regions. The epidemiology of esophageal cancer in China is typically characterized by a higher incidence rate in men than in women and a higher incidence rate in rural than in urban populations. However, since 2000, the incidence of esophageal cancer has been decreasing in both urban and rural areas, and in both males and females, with a particularly marked decrease in the incidence in females. The main histological type of esophageal cancer in China is predominantly squamous cell carcinoma, which is known to be closely related to dietary habits, including hot food, hot tea, alcohol consumption, and smoking, in addition to factors such as moldy, charcoal-grilled or smoked food preparation, drinking water, soil composition, or environmental microflora.
Preventing esophageal cancer by promoting healthy lifestyles and changing poor dietary habits, and improving early detection of esophageal cancer by targeting high-risk groups with early screening.
The implementation of early diagnosis and treatment strategies for esophageal cancer at all levels of care will help improve long-term survival and quality of life, and standardized care and multidisciplinary treatment modalities will further improve the prognosis of patients with locally advanced and late-stage esophageal cancer. The development and implementation of guidelines for the treatment of esophageal cancer is essential and requires the attention of all health professionals.
Diagnostic Guidelines for Esophageal Cancer
(a) Symptoms and signs. .
- style=”margin-left: 56pt”>
- Clinical symptoms
Typical clinical manifestations include progressive dysphagia, a sensation of choking, foreign body, burning, stagnation or fullness after eating, with or without retrosternal pain, acid reflux, heartburn, belching, initially with difficulty in eating a normal diet, and then gradually deteriorating to a semi-liquid or liquid diet only. It may or may not be accompanied by regurgitation of chyme or mucus immediately after eating, coughing up yellow pus sputum, fever, chest tightness, wheezing, vomiting, vomiting blood, black stool, chest and back pain, hoarseness, or choking on water. The risk of inadequate nutritional intake is elevated due to difficulty in eating and may accumulate over several months with wasting, weakness, lethargy, and diminished strength.
- style=”margin-left: 56pt”>
- Related Signs
Early stage esophageal cancer usually has no obvious specific signs; in the middle and late stage, there may be enlarged lymph nodes in the neck or supraclavicular region, suggesting possible lymph node metastasis; jaundice, palpable hepatomegaly or pressure pain in the liver area, etc., suggesting possible liver metastasis; restricted thoracic respiratory movement, shallow and rapid breathing The increase in abdominal wall tension, decreased abdominal respiratory motion, and mobile turbid sounds on percussion suggest the possibility of malignant ascites and peritoneal metastases; the recent significant weight loss, thinning of skin fold thickness, and navicular abdomen suggest malnutrition or cachexia.
(ii) Ancillary tests. .
- style=”margin-left: 60pt”>
- Imaging
- CT: Recommended thoracic segment esophageal cancerCT scans routinely include the cervical, thoracic, and abdominal regions; esophagogastric junction cancer CT scans may include the pelvic region depending on the condition (when clinically judged necessary). Intravenous drip as well as oral contrast enhancement is recommended,CT scanflat scan. family:Times New Roman”>/enhanced scans and multi-angle reconstructed images are used to determine the location of esophageal cancer, the depth of tumor infiltration, the relative relationship of the tumor to surrounding structures and organs, regional lymph node metastasis, and peripheral vascular invasion. If the patient has a contraindication to intravenous contrast, it is recommended to include a CT scan of the appropriate region or to supplement the ultrasound of the neck or abdomen.
-
Upper gastrointestinal tract imaging: for evaluation of primary esophageal tumor It is used to evaluate the primary tumor of the esophagus. It is more visual for determining the location and length of esophageal cancer, but does not assess the depth of primary invasion or regional lymph node metastasis. The examination should be performed in at least 3 positions: orthogonal, left anterior oblique, and right anterior oblique, with the upper border including the hypopharynx and the lower border reaching far from the pylorus.
- MRI: For CT unable to discern the relationship between the primary focus of esophageal cancer and the surrounding tracheal and bronchial membranes and the outer membrane of the aorta, < MRI can provide valuable additional information when the primary focus of esophageal cancer cannot be distinguished from the surrounding trachea and bronchiole, or the epiaortic membrane. In addition, it is clinically useful for diagnosing distant metastases in the liver, skull, and bones, and its recommendation is dependent on the judgment of the attending physician. Use with caution or contraindication in patients with intracorporeal metal implants or claustrophobic syndrome.
-
Positron Emission Computed Tomography (Positron Emission Computed Tomography span>positron emission tomography- computed tomography, span>PET-CT): for auxiliary diagnosis, pre-treatment/post-staging, efficacy assessment, and to assist in important clinical decision making. The scope of the scan is recommended for the whole body (including at least the base of the skull to the root of the thigh) . Patients with combined diabetes should have a blood glucose level of 11.1 mmol/L or less before the examination to avoid compromising the image quality. Re-staging recommendations after neoadjuvant therapy
Repeated examinations on the same instrument at the same center, fluoride-18- fluorodeoxyglucose (18F – fluorodeoxyglucose, 18F-FDG) dose differences should be within 20% of the activity and a resting time difference of 15 minutes after tracer injection. Known pregnant women should weigh the benefits of testing against the risks to clinical decision making and fetal development; breastfeeding women need to suspend breastfeeding after 18F-FDG injection 12 hours or more. Claustrophobia is a relative contraindication. There is a lack of consensus on the threshold for maximum standard uptake values in the diagnostic and assessment sessions, so they should be interpreted in the context of the attending physician’s experience and may be recommended in facilities where equipment allows.
-
Ultrasound: refers to routine body surface ultrasound, mainly applied to patients with esophageal cancer Bilateral cervical region, supraclavicular region lymph node assessment (N staging) and liver metastases assessment (M staging) diagnosis. Ultrasound-guided puncture biopsy may be performed to obtain pathologic diagnostic evidence. The above mentioned cervical and abdominal/pelvic ultrasound staging examinations are related to the experience of the diagnosing physician and can be selected by highly qualified medical institutions. In addition, it can be used to diagnose and localize thoracoabdominal effusions in patients with advanced esophageal cancer.
- style=”margin-left: 48pt”>
-
Endoscopy
-
-
Esophageal plain light microscopy. It is one of the necessary tests for the clinical diagnosis of esophageal cancer, taking into account the general typing of the primary lesion of esophageal cancer and biopsy pathology to confirm the diagnosis. For details of endoscopic staging, please refer to the chapter on esophageal cancer classification. family:Arial”>images for determination.
-
Esophageal pigment endoscopy: commonly used stains The stains include iodine solution, toluidine blue, etc., which can be used singly or in combination. By spraying pigment to contrast normal mucosa showing epithelial atypia or areas of multiple primary early carcinomas, the accuracy of T staging is improved.
-
Special endoscopic techniques: using narrow-band imaging combined with magnified endoscopy to observe Esophageal intraepithelial papillary collaterals (intrapapillary capillary loops,IPCL) with mucosal micro
The fine structure of the mucosa helps to better distinguish lesions from normal mucosa and to assess the depth of lesion infiltration; magnification endoscopy allows direct observation of the esophageal The magnification endoscope can directly observe the morphology of the mucosal surface of the esophagus and further identify the benign and malignant lesions and the possible infiltration depth of the esophageal lesions according to the staging of IPCL , which can guide targeted biopsies and determine whether the treatment indications are met; the laser confocal microendoscopy (confocal laser endomicroscopy, CLE) can magnify It can differentiate histologically between diseased and non-diseased areas without the need for biopsy, enabling 1000fold magnification of tissue to reveal cellular and subcellular structures from a microscopic perspective, enabling “optical biopsy“; these special endoscopic techniques can be considered if medical equipment allows.
-
Esophageal ultrasound endoscopy (endoscopic ultrasonography, < span style="font-family:Times New Roman">EUS): endoscopic ultrasound technique helps to show the level of invasion of the primary esophageal cancer lesion, and for -family:Times New Roman”>Tstaging diagnosis is more important. In addition,EUS also evaluates the esophagus and peri-abdominal trunk lymph nodes,EUS guided fine-needle aspiration biopsy (endoscopic ultrasonography guided fine-needle aspiration . EUS-FNA) was pathologically confirmed Nstaging. Imaging studies suggesting luminal narrowing resulting in EUS inability to pass or the presence of suspected perforation are contraindicated in patients. EUS is also influenced by the experience of the diagnostic endoscopist and is available at professionally qualified providers.
- style=”margin-left: 48pt”>
-
Other checks
-
-
There is a lack of esophageal cancer Specific blood tumor markers, such as circulating tumor cells, circulating tumor DNA/RNA, epigenetic markers (), and epigenetic markers () are currently lacking. span>DNA methylation, non-coding RNA, histone modifications, etc.), and exosomes are still in the laboratory or preclinical research stage and are not recommended for routine clinical care unless they are within the scope of clinical studies.
- Imaging of suspected upper esophageal thorax/middle cancer invading trachea/bronchial membrane, further bronchoscopy is recommended in equipped institutions/Ultrasound bronchoscopy.
- Medical institutions that have the equipment to do so may perform ultrasound bronchoscopy on trachea suspected by imaging< span style="font-family:Times New Roman">/Enlarged peribronchial lymph nodes can be diagnosed by ultrasound bronchoscopic aspiration biopsy for clear pathology.
-
MediastinoscopyThorax/Laparoscopic lymph node dissection biopsy and other invasive tests under general anesthesia can be performed in highly selective patients after multidisciplinary discussion to aid in diagnostic and treatment decisions.
(iii) Clinical diagnosis. .
The pathologic diagnosis (gold standard) requires an esophageal endoscopic biopsy to confirm the diagnosis. In cases where endoscopy is contraindicated or repeated biopsy attempts have failed to clarify the pathological diagnosis, a combination of upper gastrointestinal angiography,
(cervical) thoracic (abdominal) enhancement CT, whole-body PET-CT CT, and PET-CT. Roman”>PET-CT or EUS or ultrasound bronchoscopy
(endobronchial ultrasound, EBUS) guided puncture biopsy as an aid to diagnosis. Imaging of suspicious metastatic lymph nodes or distant organs should be based on a comprehensive assessment of medical conditions and operative risk factors, and a reasonable biopsy modality should be selected at the discretion of the attending physician.
The clinical staging diagnosis should include (cervical) thoracic / abdominal (pelvic) enhancement CT, depending on the medical condition, ultrasonography, EUS, PET-CT < /span> and MRI and other imaging evaluation methods. The diagnosis of restaging after neoadjuvant therapy remains based on the initial clinical staging approach before treatment, and invasive biopsy pathology may be performed for reconfirmation of suspected metastatic regional lymph nodes or distant organs, taking into account medical conditions and operational risks.
(iv) Screening of healthy people at high risk for esophageal cancer.
Age ≥40 years, from areas with high incidence of esophageal tumors, or with family history of esophageal tumors, high risk factors for esophageal cancer (smoking, heavy alcohol consumption, head and neck or respiratory tract The screening by endoscopic iodine staining of esophageal mucosa is recommended for those who are at high risk of esophageal cancer, or have a family history of esophageal cancer, or have high risk factors for esophageal cancer (smoking, heavy alcohol consumption, head and neck or respiratory tract cancer, preference for hot and pickled foods, poor oral hygiene, etc.). If no lesions are found endoscopically, regular follow-up endoscopy will be performed. If a superficial lesion is found, a biopsy is taken to assess the pathology. If the pathology is low-grade intraepithelial neoplasia /heterogeneous hyperplasia, follow up every 3 years 1 time; if the pathology is high-grade intraepithelial neoplasia /heterogeneous hyperplasia, the
Endoscopic treatment may be considered if the pathology is a high-grade intraepithelial neoplasia
and no vascular invasion is found. If the endoscopic presentation is more severe than the biopsy pathology, fine esophageal endoscopy (including magnification endoscopy, narrow-spectrum imaging, and staining) is recommended to assess the lesion and determine the plan of care.
Age ≥40 years with high-risk factors for esophageal cancer (cardia achalasia, corrosive stenosis, callosity, obesity) is recommended every 1 to 3 years for 1 endoscopic iodine staining evaluation of the esophageal mucosa.
For patients with known or newly identified risk factors for Barrett’s esophagus at endoscopy, it is recommended that endoscopic esophageal staining be performed every 2 cm in patients with known or newly identified risk factors for Barrett’s esophagus style=”font-family:Times New Roman”>4 point biopsies (at least 8 pieces of biopsy tissue). If there is a Los Angeles graded diagnosis of B, C, D class esophagitis, regular proton pump inhibitors are required for 8 to 12 weeks before endoscopic diagnosis; if there is no Barrett’s esophagus, endoscopic screening can be terminated; if the pathological diagnosis is Barrett’s esophagus without Barrett’s esophagus If the pathological diagnosis is Barrett’s esophagus without heterogeneous hyperplasia, repeat endoscopy and pathological biopsy every 3 to 5 years; if the pathological diagnosis is Barrett’s esophagus with low-grade intraepithelial neoplasia /, repeat endoscopy and pathological biopsy every / heterogeneous hyperplasia, endoscopic treatment of the esophagus or annual endoscopy and biopsy at 1 cm intervals would be required. Roman”>4 site biopsy; if the pathologic diagnosis is Barrett’s esophagus combined with high-grade intraepithelial neoplasia, endoscopic treatment or surgical treatment of the esophagus is required.
(E) Classification and staging of esophageal cancer.
- style=”margin-left: 60pt”>
-
Clinical segmentation of esophageal cancer
-
Cervical segment of esophagus: up from the hypopharynx The cervical esophagus is located at the level of the upper sternal notch, which is the entrance to the thorax. It is surrounded by the trachea, cervical vascular sheath, and spine. It is usually endoscopically located 15to20cm.
-
Suprastern esophagus: from the upper thoracic The upper part of the thoracic esophagus starts from the entrance of the thorax and goes down to the lower edge of the arch of the odd vein (i.e. above the level of the pulmonary hilum). It is surrounded anteriorly by the trachea, the 3 branches of the aortic arch, and the cephalic brachial vein, and posteriorly by the spine. Endoscopically it is usually 20to25cm.
-
Mid-thoracic esophagus: from the inferior border of the arch of the odd vein superiorly to the inferior border of the inferior pulmonary vein (i.e., between the levels of the pulmonary hilum). It is sandwiched between the two pulmonary hilum anteriorly, adjacent to the descending thoracic aorta on the left, adjacent to the spine posteriorly, and free and directly adjacent to the pleura on the right. It is usually endoscopically located 25to 30cm.
- style=”margin-left: 75pt”>
- The lower thoracic esophagus, starting from the inferior border of the inferior pulmonary vein above and ending at the esophagogastric junction
(i.e., below the level of the pulmonary hilum). The endoscope is usually 30 to 40 cm from the incisors.
Clinically, multiple imaging and endoscopic findings need to be combined to diagnose the esophageal segment in which the central location of the lesion is located.
- style=”margin-left: 48pt”>
- Definition of the esophagogastric junction
The esophagogastric junction, i.e., the end of the esophagus and the beginning of the stomach, corresponds to the level of the cardia incisura or peritoneal reflexion or the lower edge of the esophageal sphincter, and does not necessarily coincide with the histological squamocolumnar junction, with the anatomical extent including the lower thoracic esophagus, the esophagogastric junction line and the proximal stomach 5 cm range. Clinical management is often based on the Siewert staging, with the center of the lesion located at the esophagogastric junction line (also known as the squamocolumnar junction line, Z line or Zline). span>line or EGJ line) and within 5 cm above and below each other are classified as.
Siewert Type I: The center of the tumor is located above the esophagogastric junction line 1~5cm range.
Siewert Type II: The center of the tumor is located above the esophagogastric junction line 1cm to below 2cm
range.
Siewert Type III: The center of the tumor is located below the esophagogastric junction line 2~5cm range. If the tumor involves the esophagogastric junction, the center of the tumor is on the esophageal side of the esophagogastric junction or
If the tumor is within 2 cm of the gastric side (Siewert Type I and II), follow the esophageal cancer staging principles.
Tumor center outside the proximal gastric 2 cm (Siewert type III) or although the tumor center is in the proximal gastric type III the proximal stomach
within 2 cm but without involvement of the esophagogastric junction, the principles of gastric cancer staging are followed.
- style=”margin-left: 48pt”>
- Endoscopic staging of superficial esophageal cancer and precancerous lesions
- The lower thoracic esophagus, starting from the inferior border of the inferior pulmonary vein above and ending at the esophagogastric junction
Our endoscopic staging: occult (congested), cachectic, plaque, and papillary. International endoscopic typing (2005 Paris typing): augmented lesions (0- I), flat lesions (< span style="font-family:Times New Roman">0-II) and depressed lesions (0-III). The 0-I type is further divided into the tipped type (0-Ip) and non-tipped type (0-Ⅰs). Intramucosal carcinomas usually present as 0-IIb types, 0-IIa and 0-IIc
type with smooth or regular small granular lesion surface, while submucosal carcinoma is usually 0-type I and
0- type III, with irregular coarse granular or uneven small nodular lesion surfaces. See Appendix A for details.
Level classification of lesions: lesions that are confined to the epithelium and do not breach the basement membrane are M1 type ( High-grade intraepithelial neoplasia / severe heterogeneous hyperplasia; Tis); superficial esophageal cancer is divided into intramucosal and submucosal carcinoma : Intramucosal carcinoma is divided into M2 type and M3 type; M2 type refers to lesions that break through the basement membrane and invade the mucosal layer; M3 type refers to lesions that invade the mucosal muscular layer. Submucosal carcinoma can be classified according to the depth of invasion into SM1 type, SM2 type, SM3, SM1 type means that the lesion invades the upper 1/3 of the submucosa Roman”>1/3; SM2 type means that the lesion invades the middle 1/3 of the submucosa; SM3 type refers to lesion invasion of the submucosal layer under 1/3. For endoscopically resected esophageal squamous carcinoma specimens, 200 μm was used as the threshold to distinguish between superficial and deep submucosal lesion invasion.
- style=”margin-left: 60pt”>
-
Broad staging of progressive esophageal cancer
Medullary type: The lesion is characterized by thickening of the esophageal wall with sloping rim elevation.
Muscarinic type: tumor rim is elevated with lip-like / mushroom-like ectopia and may be accompanied by superficial ulceration on the surface. Ulcerated type: The lesion has a distinct central ulcer, usually accompanied by a marginal bulge.
Constricted type: characterized by marked narrowing of the canal lumen, and the patient has significant dysphagia symptoms. Intraluminal type: The lesion appears mushroom-like or polyp-like with / no banding.
- style=”margin-left: 60pt”>
- Histologic types of esophageal cancer pathology
Refer to 2019 Edition WHO Classification of Tumors of the Digestive System, common pathological histological types include squamous carcinoma, adenocarcinoma, neuroendocrine tumors, and other types, as detailed in Appendix B. span>.
- style=”margin-left: 60pt”>
- International Staging Principles for Esophageal Cancer
Referring to the International Union for International Cancer Control (Union for International Cancer Control , UICC ) / American Cancer Society (/American Cancer Society (UICC) family:Times New Roman”>American Joint Committee on Cancer, AJCC) No. American Joint Committee on Cancer, AJCC. family:Times New Roman”>8th edition of the TNM staging system, which places the primary esophageal tumor (T), regional lymph nodes
- style=”margin-left: 56pt”>
-
, distant organ metastases (M) and degree of pathological differentiation (G< span style="font-family:Arial">) are defined as follows.
- Primary tumor (T)
Tx Primary tumor not evaluable
T0 No evidence of primary tumor
Tis high-grade intraepithelial neoplasia/heterogeneous hyperplasia T1a tumor invading mucosal lamina propria or mucosal muscularis T1b tumor invading submucosa
T2 Tumor invasion of the intrinsic muscular layer
T3 Tumor invasion of esophageal fibrous membrane
- Primary tumor (T)
T4a Tumor invades adjacent organs (resectable), such as pleura, pericardium, odd vein, diaphragm or peritoneum
T4b Tumor invades adjacent vital organs (unresectable), such as the aorta, vertebral body, or trachea
- style=”margin-left: 84pt”>
- Regional lymph nodes (N)
Nx Regional lymph nodes not evaluable
N0 No regional lymph node metastasis
N1 1~2 regional lymph node metastasesN2 3 to 6 Regional lymph node metastases N3 ≥7 regional lymph node metastases
- style=”margin-left: 80pt”>
-
Distant metastases (M)M0 No distant transferM1 with distant metastases
- Degree of pathological differentiation
Gx Degree of differentiation cannot be assessed
G1 Highly differentiatedG2 Medium differentiation G3 Low differentiation
- Degree of pathological differentiation
Clinical stage (cTNM), pathological stage according to different clinical conditions
(pTNM) and pathological staging after induction therapy (pTNM). family:Times New Roman”>ypTNM)3 types, as described in Appendix C.
The above staging principles apply to esophageal cancer, including squamous cell carcinoma, adenocarcinoma, adenosquamous carcinoma, undifferentiated carcinoma, neuroendocrine carcinoma, and adenocarcinoma with neuroendocrine features, but not to neuroendocrine tumors of the esophagus and non-epithelial tumors, such as lymphoma sarcoma, gastrointestinal mesenchymal tumor, and melanoma.
- style=”margin-left: 44pt”>
- International UICC/AJCC No. 8 version of esophageal cancerTNM staging of regional lymph node substage1R Right cervical paratracheal: right supraclavicular region around the trachea to the right apical region of the lung1L Left cervical paratracheal: left supraclavicular region around the trachea to the region of the left apical lung
2R Right upper paratracheal: the intersection of the inferior border of the cephalic brachial artery with the trachea to the right pulmonary apical region
Domain
2L Paratracheal left upper segment: superior border of the aortic arch to the left apical region of the lung
4R Right lower paratracheal segment: inferior border of cephalic brachial artery and trachea intersection to superior border of odd vein
region
4L Left lower paratracheal: area from the superior border of the aortic arch to the level of the rongeur
7 Subaortic: the area below the tracheal ridge
8U Suprastern paraesophageal: the area from the lung apices to the tracheal bifurcation
8M Mid-thoracic paraesophageal: area from the tracheal bifurcation to the inferior border of the inferior pulmonary vein
9R Right inferior pulmonary ligament: within the right inferior pulmonary ligament
9L Left inferior pulmonary ligament: within the left inferior pulmonary ligament
- style=”margin-left: 64pt”>
- Diaphragm: area from the top of the diaphragm to the foot of the diaphragm
- Parietal: the area immediately adjacent to the esophagogastric junction
- Left gastric artery: the area along the left gastric artery
- Common hepatic artery: the area immediately proximal to the common hepatic artery
- Spleen artery: immediately proximal to the area of the splenic artery
- Abdominal: the region of the root of the abdominal celiac artery
The lymph nodes in the VI and VII regions of the neck were referred to the regional lymph node substation criteria for head and neck tumors.
- style=”margin-left: 60pt”>
- Esophageal Society of Japan (Japan Esophagus Society, (JES), 11th Edition Esophageal Cancer
Staged Lymph Node Staging
JES Staging system for esophageal cancer focuses on surgical options and radiotherapy target planning for squamous esophageal cancer. The JES staging system for esophageal cancer is mainly for surgical planning and radiotherapy target planning for esophageal squamous carcinoma, and therefore also has reference value for the majority of patients with esophageal squamous carcinoma.
JES Regional Lymph Node Staging.
Cervical lymph nodes: superficial cervical lymph nodes (100), cervical paraesophageal lymph nodes (101), the deep cervical lymph nodes (102), the upper deep cervical lymph nodes (102up), the deep cervical lymph node in the middle (102mid), the retropharyngeal lymph node (103), supraclavicular lymph nodes (104)
Thoracic lymph nodes: upper thoracic paraesophageal lymph node (105), thoracic para-tracheal lymph node
(106 ), the paratracheal lymph node in the thoracic segment (106rec ), and the lymph node in the retrosternal nerve (106rec ). 106rec ), the left recurrent lymph node of the laryngeal nerve
(106recL ), right recurrent laryngeal node (106recR ), and right recurrent laryngeal node (106recR ). Roman”>106recR ), anterior tracheal lymph node
(106pre), tracheobronchial lymph node (106tb) Roman”>106tb), left tracheobronchial lymph node
(106tbL), right tracheobronchial lymph node (106tbR), subrhinal lymph node
(107), mid-thoracic paraesophageal lymph nodes (107), and mid-thoracic paraesophageal lymph nodes (108), main bronchial lymph nodes (hilar lymph nodes, 109), lower thoracic paraesophageal lymph nodes (110), supra-diaphragmatic lymph nodes (111), posterior mediastinal lymph nodes (112) Roman”>112), anterior thoracic aortic lymph node (112aoA), posterior thoracic aortic lymph node (112aoP), inferior pulmonary ligament lymph nodes (112pul), arterial ligament lymph nodes
(113), anterior mediastinal lymph nodes ( 114).
Abdominal lymph nodes: right cardia lymph node (1), left cardia lymph node (1) “font-family:Times New Roman”>2), the gastric lesser curvature lymph node (3), and the lateral gastric lesser curvature lymph node along the left branch of the gastric artery (3a), lymph nodes of the lesser curvature of the stomach distal to the second branch of the right gastric artery (3b), lymph nodes of the left gastric greater curvature along the short gastric artery
(4sa), left gastric greater curvature lymph node along the left gastroretinal artery (4sb), the right gastric greater curvature along the second branch of the right gastric retinal artery to the distal lymph nodes (4d), the suprapyloric lymph nodes (4d), and the suprapyloric lymph nodes (5), subpyloric lymph node (6), left gastric artery lymph node (7), anterosuperior lymph node of the common hepatic artery
(8a), posterior common hepatic artery lymph node (8p), abdominal trunk lymph nodes (9), splenic hilar lymph nodes (10), proximal splenic artery lymph nodes (11p), distal splenic artery lymph nodes (11d) Roman”>11d), lymph nodes along the intrinsic hepatic artery within the hepatoduodenal ligament (12a), lymph nodes along the common bile duct within the hepatoduodenal ligament (12b), lymph nodes along the portal vein within the hepatoduodenal ligament (12p), and lymph nodes behind the head of the pancreas (13), superior mesenteric vein lymph node (14v), middle colonic artery lymph node ( 15), lymph node of the abdominal aortic foramen ovale (16a1), lymph node of the peri-abdominal aorta between the superior border of the celiac trunk and the inferior border of the left renal vein (16a2) Roman”>16a2), periaortic lymph nodes between the inferior border of the left renal vein and the superior border of the inferior mesenteric artery (16b1), and periaortic lymph nodes between the superior border of the inferior mesenteric artery and the bifurcation of the main abdominal artery (16b1). span style=”font-family:Times New Roman”>16b2), anterior pancreatic head lymph node (17), inferior pancreatic margin lymph node (18), subphrenic lymph nodes (19), diaphragmatic esophageal foramen lymph nodes
(20).
(vi) Nutritional assessment of patients with esophageal cancer. .
Nutritional assessment of patients in the initial stage of esophageal cancer diagnosis and treatment is an important part of the comprehensive assessment at baseline. The nutritional assessment includes both nutritional risk screening and nutritional assessment.
- style=”margin-left: 60pt”>
- Nutritional Risk Screening
Nutritional risk screening is the process of applying nutritional risk screening tools to determine whether a patient has a nutrition-related risk that may affect clinical outcomes. The currently used clinical nutritional risk screening 2002 () Nutritional Risk Screening 2002, NRS2002) tool, among others. Patients should be screened within 24 hours of admission by trained physicians, dietitians, pharmacists, and nurse practitioners using the NRS2002 >Nutritional risk screening. For those at nutritional risk, a targeted nutrition diagnosis and intervention plan is required; for those not at nutritional risk, a repeat nutrition risk screening should be performed after 7 days.
For elective surgery, nutritional risk screening should be advanced to 10 days or more prior to surgery. The NRS2002 tool includes three components: impaired nutritional status score, disease severity score, and age score.
See Appendix D for details. When the total score ≥3 is “Nutritional Risk“ and requires a nutritional diagnosis and intervention plan.
- style=”margin-left: 60pt”>
- Nutritional Assessment
Nutritional assessment is a process to further understand the nutritional status of individuals at nutritional risk. It consists of two parts: a basic nutrition assessment and a malnutrition assessment.
-
Basic Nutrition Assessment: The Basic Nutrition Assessment is a nutritional management program for all individuals at nutritional risk. The assessment includes: nutrition-related medical history, dietary survey, physical examination
(height, body mass, etc.), laboratory tests (liver and kidney function, blood glucose, lipids, electrolytes, acid-base balance, etc.). These tests are routinely collected in hospitalized patients and are necessary for nutrition intervention planning, prescribing and monitoring.
-
Malnutrition assessment: Malnutrition assessment involves the diagnosis and classification of malnutrition. It is recommended that malnutrition be assessed according to the consensus of malnutrition diagnostic criteria initiated by global (nutrition) leaders. For those who screen positive for nutritional risk, if at least 1 positive for each of the manifest and etiologic indicators (Appendix ) span>E), a diagnosis of malnutrition can be made. In addition, a subjective global assessment (Subjective Global Assessment,SGA), patient participation in SGA and other rating scales.
II. Guidelines for the treatment of esophageal cancer
(a) Surgical treatment. .
Surgical treatment is one of the major radical treatments for esophageal cancer. Before 2000, the left thoracic approach was the main approach for surgical treatment of esophageal cancer in China, and the left thoracic aortic arch obscured and the supra-arch triangle narrowed, resulting in incomplete clearance of the upper mediastinal lymph nodes. The recurrence rate is as high as 30% to 40%, which seriously affects long-term survival. This has led to a 5 year survival rate of nearly 30 years after surgical treatment of esophageal cancer with a left thoracic approach in China
has hovered at 30% to 40%. With the progress of standardized treatment of esophageal cancer in China and the popularization of minimally invasive thoracic and laparoscopic surgery for esophageal cancer in recent years, the right thoracic approach has gradually increased. The right thoracic approach has a more complete lymph node dissection because there is no obscuration of the aortic arch. Lymph node dissection in the neck is elective in most hospitals. Compared with the left thoracic approach, complete thoracic and abdominal second-field or cervical, thoracic, and abdominal third-field lymph node dissection via the right thoracic approach can reduce the postoperative recurrence rate of cervical and thoracic lymph node metastases and significantly improve the 5-year survival rate. In addition, the surgical-only treatment paradigm for locally progressive esophageal cancer has been replaced by a multidisciplinary, integrated treatment model based on surgery, which includes preoperative neoadjuvant and postoperative adjuvant therapy involving chemotherapy, radiotherapy, and immunotherapy. This section focuses only on the content of guidelines related to surgical treatment.
- style=”margin-left: 60pt”>
-
Principles of Surgical Treatment
-
Surgical resectability is determined by an experienced thoracic surgeon in esophageal surgery. Surgical resectability needs to be assessed by an experienced thoracic surgeon in esophageal surgery, including surgical access and lymph node dissection strategy to achieve the goal of radical resection including the primary tumor and regional lymph nodes.
-
Surgical treatment plans should be based on a review of the esophageal cancer disease profile (including esophageal cancer involvement and clinical stage), patient comorbidities, and surgical patient outcomes.
- Surgical approach selection: for thoracic esophageal cancer, a right thoracic approach is recommended. For cancer of the middle and lower thoracic esophagus without lymph node metastasis in the upper mediastinum, the left thoracic approach can also be chosen.
-
Optional surgical approaches: traditional open or lumpectomy-assisted or Robotic-assisted McKeown esophagectomy for esophageal cancer (right thoracic free esophagus) “font-family:Times New Roman”>+Trans-epigastric free stomach+< span style="font-family:Arial">neck anastomosis),Ivor Lewis Esophageal cancer resection (trans-epigastric free stomach+trans-right thoracic free esophagus+intra-thoracic anastomosis),Sweet< span style="font-family:Arial">esophageal cancer resection (transthoracic free esophagus+) transdiaphragmatic free stomach+intra-thoracic or cervical anastomosis), combined left thoracoabdominal incision+neck or thoracic anastomosis
combination, combined thoracic and abdominal second-field or cervical, thoracic and abdominal third-field lymph node The lymph node dissection. For patients with cT1 to 2N0 stage esophageal cancer who do not tolerate transthoracic surgery, various procedures such as transdiaphragmatic fissure esophageal endorectal extraction can be chosen. In patients with stage 2N0 esophageal cancer, various procedures such as trans-diaphragmatic endorectal extraction can be chosen. For esophagogastric junction cancer, the choice of procedure is based on Siewert staging: Siewert type I Refer to esophageal surgery; Siewert Type III refer to gastric surgery; Siewert Type II surgery Treatment is more controversial and is currently decided more on the basis of the surgical habits and different proficiencies of thoracic and gastrointestinal surgeons together.
- Optional lymph node dissection: If there are no suspicious metastatic lymph nodes in the neck region, a complete two-field lymph node dissection of the thoracic and abdominal regions (conventional two-field thoracoabdominal < +lymph nodes in the upper mediastinal region, especially those around the bilateral laryngeal nerve chain); if there are suspicious metastatic lymph nodes in the neck region, or upper thoracic esophageal cancer, then cervical, thoracic and abdominal lymph node dissection is recommended (bilateral lower cervical region + bilateral supraclavicular region < span style="font-family:Times New Roman">+ the above mentioned complete diaphyseal lymph nodes).
-
Optional Surrogate Organs and Upper GI Reconstruction Pathways: The most commonly used surrogate organs are The most common substitutes for the esophagus are the stomach, colon and jejunum; whether microsurgical anastomosis with tipped vessels is required should be considered as appropriate. The upper gastrointestinal tract can be reconstructed from the original esophageal bed, posterior sternum, or anterior sternum.
-
The number of esophageal surgeries and the size of the associated specialty team are important factors affecting the perioperative complication rate and mortality of esophageal cancer. Therefore, it is recommended to perform esophagectomy in a large center with experienced esophageal cancer treatment or in a group of physicians who have received standardized training.
- style=”margin-left: 48pt”>
-
Guidelines for post-surgical follow-up
Post-operative 2 years 3 monthly and 1 semi-annually for 2 to 5 years The review will be conducted 1 time and 5 years later, the review will be conducted 1 time. The review will include a cervical /thoracic / abdominal CT or ultrasound of the neck and abdomen and various laboratory tests. Upper gastrointestinal imaging, whole-body PET-CT, bone scan, cranial MRI and upper gastrointestinal endoscopy The examination can be optional depending on the patient’s postoperative condition
-
Examinations. Pathologic biopsy may be performed as appropriate to clarify the diagnosis if a suspected recurrent or metastatic lesion is identified during follow-up.
(ii) Radiotherapy. .
Radiotherapy is an important part of the comprehensive treatment of esophageal cancer, involving preoperative neoadjuvant, postoperative adjuvant, radical and palliative treatment.
For cTis ~ 2 N1 to 3 M0 or cT3 to 4a Nany M0 stage esophageal cancer, preoperative neoadjuvant radiotherapy is recommended to improve radical resection rate, pathological complete remission rate, local tumor control rate, and thus long-term survival after surgery; for those who do not plan surgery or refuse surgical treatment, radical simultaneous radiotherapy is recommended; for those who are pathologically evaluated as non-radical resection after surgery (< span style="font-family: "font-family: "Times New Roman">4a Nany M0 stage esophageal cancer, preoperative neoadjuvant radiotherapy is recommended to improve long-term survival after surgery. span style=”font-family:Times New Roman”>R1 or R2), or although R0 excision, but for (y)pT4 Nany M0 stage, postoperative adjuvant concurrent radiotherapy can be considered depending on the patient’s recovery.
Superficial esophageal cancer assessed pathologically by endoscopic esophageal mucosal resection at stage T1b or Stage T1a combined with vascular thrombosis, nerve involvement, poorly differentiated or undifferentiated carcinoma or non-R0 excision, esophagectomy is the first choice, and those who are surgically If the patient is not suitable for surgery or refuses surgery, adjuvant radiotherapy or concurrent radiotherapy can be considered; for patients with unresectable cT4bNanyM0 stage esophageal cancer assessed by surgery or who refuse surgery, radical concurrent radiotherapy is recommended.
Postoperative local recurrence, advanced esophageal cancer combined with esophageal obstruction, extensive lymph node metastases, and combined distant organ metastases (lung, bone, brain, etc.) may be considered for palliative radiation therapy if the disease is assessed to be stable or regressed after systemic drug therapy.
- style=”margin-left: 57pt”>
-
Guidelines for Radiotherapy Protocol Development
-
Radiotherapy technique: 3D conformal radiotherapy or intensity-modulated radiotherapy is recommended, with the latter preferred. The latter technique is preferred. Several studies in radiation physics have shown that 3D conformal or intensity-modulated radiotherapy is more effective in target dose distribution and normal tissue and organ preservation than the earlier conventional 2D radiotherapy techniques.
The superior performance of 3D conformal or intensity-modulated radiotherapy compared to earlier conventional 2D radiotherapy techniques in terms of target dose distribution and normal tissue and organ preservation, especially for the heart and lung, reduces radiotherapy-related adverse effects.
-
CT. “font-family:Arial”>Simulated positioning: supine position with arms extended at the side of the body or with hands crossed over the elbows in front of the forehead. Patients with cervical and upper segments were recommended to have head and neck shoulder mask fixation, and middle and lower segments and esophagogastric junction cancer body membrane fixation. An intravenous contrast-enhanced scan with a layer thickness of 0.5 cm was performed. Enhanced scans may not be performed in those with a history of contrast allergy.
Cancer of the lower esophagus and esophagogastric junction, or patients who need to irradiate the left side of the stomach or abdominal lymph nodes, in order to reduce the difference in irradiation volume due to the size of the stomach filling, CT simulation of positioning before fasting 3 to 4 hours, CT scanning before and 15 minutes before each radiotherapy session, patients should take 200 to 200 to 200 minutes before each radiotherapy session. family:Times New Roman”>300ml semi-liquid diet (e.g., thick porridge, yogurt, etc., per dose).
Patients with a postoperative residual stomach located in the mediastinum should not fill the stomach and should be positioned in the absence of gastric contents, as is the case with radiation therapy.
- style=”margin-left: 68pt”>
- Target area definition.
- Target area definition.
-
Preoperative Neoadjuvant Synchronous Radiotherapy or Radical Synchronous Radiotherapy: There is no target area specification for esophageal cancer. It is recommended to outline the neoadjuvant radiotherapy target area according to the principles of radical radiotherapy target area design. The location of the anastomosis planned for the subsequent esophagectomy should be considered when drawing the target area, and the anastomosis should be avoided to be located in the field of projection.
Large Tumor Target Area (Gross Tumor Volume, GTV) and lymph node target areas
(Gross Tumor Volume – Lymph Node, GTVnd): the primary tumor of esophageal cancer visible in combination with each pretreatment clinical assessment was GTV, and the lymph nodes with confirmed metastasis or not excluded metastasis were GTVnd.
Clinical Target Volume (Clinical Target Volume, CTV). ①Cervical / upper thoracic esophageal cancer: GTV inferior and superior ectopia 3cm, GTVnd three-dimensional outgrowth 0.5 ~1cm. Generally need to include mid
neck, 1 (lower neck, bilateral supraclavicular), < span style="font-family:Times New Roman">2, 4, 4, 7 lymph node drainage areas. The cervical segment may not include 7 areas. The distant target area can be considered for involvement of field irradiation, such as upper segment esophageal cancer with abdominal lymph node metastasis. (ii) Mid-thoracic esophageal cancer: GTV extended 3 cm above and below, 3 cm, GTVnd three-dimensional flare 0.5~1cm. It generally needs to include 1, 2, 4, 7, and some 8 lymph node drainage areas. Because of the high probability of abdominal lymph node metastasis in middle esophageal cancer, some patients may require irradiation of 15, 16, 16, and 16. span style=”font-family:Times New Roman”>17 and even 20 areas. (iii) Lower thoracic esophageal cancer /Siewert I/Siewert type II esophagogastric junction cancer:GTV extended 3cm above and below, 3cm, GTVnd three-dimensional external expansion 0.5~1cm, which generally needs to include 7, 7, 7. 8, 15, 15, 16, 17, 20 lymph node drainage areas, and some patients may require include the proximal end of the 18, 19 area. Distal target areas may be considered for involvement by field irradiation, such as the lower esophageal cancer with lymph node metastases in 1 area.
Planning Target Volume (Planning Target Volume, PTV): determined by the actual pendulum error, generally based on the CTV three-dimensional outward expansion 0.5cm formation, and cervical segment or upper thoracic esophageal cancer fixed by head-neck-shoulder mesh can be extensively expanded 0.3cm.
PGTV (when sequential or simultaneous dosing is used):GTV+GTVnd 3D external expansion 0.5cm.
-
Postoperative adjuvant radiotherapy/< span>synchronous radiotherapy: to include anastomotic conditions: primary cervical or upper esophageal cancer, or incision margin ≤ 3 cm from the tumor. span>.
GTV and GTVnd:R1 or R2 after resection of the GTV including residual primary tumor, anastomosis with positive cut margins, and GTVnd including residual lymph nodes.
CTV: 1) Cervical segment / upper thoracic esophageal cancer: including GTV+GTVnd (if any), anastomosis, 1, 2, 4, 7 lymph node drainage areas. The cervical segment may not include 7 areas. T4b is required to include the tumor bed.
②Mid-thoracic esophageal cancer: including GTV+GTVnd (if any), 1, 2, 4, 4, 7, and some 8 lymph node drainage areas. As appropriate based on pathologic findings including 15, 16, 17, 20 lymph node drainage areas. T4b needs to include the tumor bed. (iii) Lower thoracic esophageal cancer /Siewert I/Siewert II esophagogastric
Junctional carcinoma: including GTV+GTVnd (if any), 1, 2, 4, 7, 8, 8, 15, 16, 17< /span>, 20 lymph node drainage areas. T4b needs to include the tumor bed.
PTV: determined by the actual positional error, generally at CTV with an outward expansion of 0.5cm
formation, and cervical segment or upper segment esophageal carcinoma with head and neck shoulder mesh fixation may be extensively expanded by 0.3cm.
PGTV (with tumor or lymph node remnants requiring sequential or simultaneous dosing):
PGTV (with tumor or lymph node remnants requiring sequential or simultaneous dosing).
GTV+GTVnd extension 0.5 cm.
- style=”margin-left: 57pt”>
- Prescribing Dose Guidelines
-
Preoperative Neoadjuvant Radiotherapy/synchronous radiotherapy:95% PTV 40-50Gy/1.8-2.0Gy /span>, daily 1 time per week < /span>5 times. Units that are available can also use simultaneous dosing techniques.
- style=”margin-left: 68pt”>
- Postoperative Adjuvant Radiotherapy/Synchronous radiotherapy.
R0 Postoperative: 95% PTV 50-54Gy/1.8-2.0Gy daily 1 times per week 5 times per week.
R1/2 Post-op: 95% PTV 50Gy/1.8 to 2.0Gy , sequential 95% PGTV
10Gy/1.8~2.0Gy, daily 1 time per week < span style="font-family:Times New Roman">5 times. Synchronized dosing techniques can also be used in units where available.
- Postoperative Adjuvant Radiotherapy/Synchronous radiotherapy.
-
Radical radiotherapy/Synchronous radiotherapy: ① 95% PTV 60Gy/ 1.8 to 2.0Gy daily 1 times per week 5 times per week. ② 95% PTV 50Gy/1.8~2.0Gy, sequential 95% PGTV 10Gy/1.8~2.0Gy, daily 1 time per week 5 times. Units that are available can also use simultaneous dosing techniques.
Note: The radiotherapy dose can be reduced to 50~54Gy in radical synchronous radiotherapy as appropriate, and most domestic units currently use 60Gy.
- style=”margin-left: 44pt”>
- Normal tissue dose
- Normal tissue dose
For patients treated with postoperative or preoperative radiotherapy, it is recommended to start with the full prescribed dose (e.g. 95% PTV 60Gy) and then perform the actual prescribed dose, while determining the actual amount of normal tissue received.
(1) Both lungs: mean dose <14Gy to 16Gy, V20 ≤ 28%, V30 ≤ 20%; those with concurrent radiotherapy V20 ≤ 25%; and those who have been treated with immune drugs have the lowest possible lung receptors.
(2) Heart: V30 <40%, V40<30%
(3) Spinal cord (planned organ endangerment):Dmax<45Gy
(4) Stomach: V< sub>40<40%, Dmax<55 to 60Gy
(5) Small intestine: V 40<40%, Dmax<55Gy
(6) Double kidney: V 20<30%
(7) Liver: V< sub>30<30%
- style=”margin-left: 57pt”>
-
Synchronous chemotherapy regimen
- Paclitaxel+ Platinums.
- Paclitaxel+ Platinums.
Paclitaxel 45-60mg/m2 >, IV drip, day 1.
Cisplatin 20-25mg/m2< , IV drip, day 1 [or carboplatin concentration [ = “font-family:Times New Roman”>- area under the concentration-time curve, area under the concentration-time curve, AUC)=2, intravenous drip, first 1 day).
Repeat weekly
-
Cisplatin+fluorouracil or capecitabine or tegeo: Capecitabine or tegeo can be used instead of fluorouracil due to similar or better efficacy than fluorouracil, less severe side effects, and ease of oral administration.
Cisplatin 30mg/m2, IV drip, day 1.
Capecitabine 800mg/m2, intravenous, 2 times daily, first 1 to 5 days; or Tegeo 40 to 60 mg/m2, orally, daily 2 times a day for the first 1 to 5 days.
Repeat weekly
- style=”margin-left: 41pt”>
- Paclitaxel+fluorouracil or capecitabine or tegeo: Paclitaxel45-60mg/m2, IV drip, day 1 .
Capecitabine 625 to 825 mg/m2, IV. 2 times daily for the first 1 to 5 days; or Tegeo 40-60mg/m2 orally, 2 times daily, first 1 to 5 days.
Repeat weekly
- style=”margin-left: 41pt”>
- Oxaliplatin+fluorouracil or capecitabine or tegeo (recommended for adenocarcinoma): oxaliplatin85mg/m2, IV drip, 1st1, , 15, 29 , 29 “font-family:Arial”>day.
Capecitabine 625 mg/m2, IV drip, daily < span style="font-family:Times New Roman">2 times on the first 1 to 5 days; or Tegeo 40-60mg/m2 orally, 2 times daily, first 1 to 5 days.
Repeat weekly
See Appendix F for details of efficacy assessment.
- style=”margin-left: 57pt”>
- Guidelines for Post-Radiotherapy Evaluation and Follow-up
- Post-operative neoadjuvant radiotherapy evaluation: recommended at the end of preoperative neoadjuvant radiotherapy 1 months after the end of preoperative neoadjuvant radiotherapy, including enhanced CT. span>(including neck, chest and abdominal region) and laboratory tests such as routine blood and biochemistry. Upper gastrointestinal tract imaging, whole body PET-CT, bone scan, cranial , and cranial family:Times New Roman”>MRI can be selected according to the condition; repeat esophageal endoscopy, fiberoptic bronchoscopy, and can be considered for accurate clinical re-staging as appropriate. family:Times New Roman”>EBUS guided transbronchoscopic needle aspiration biopsy () may be considered as appropriate for accurate clinical restaging. endobronchial ultrasoundguidedtransbronchial needle aspiration,EBUS-TBNA) or EUS-FNAre-biopsy of regional enlarged lymph nodes and other invasive tests. Radical esophageal cancer resection is recommended at 4 to 8 weeks after the end of radiotherapy.
- style=”margin-left: 82pt”>
-
Follow-up after postoperative adjuvant radiotherapy: recommended at the end of postoperative adjuvant radiotherapy 3 months
Start follow-up with a recommended frequency of initial 2 years within 2 years =”font-family:Times New Roman”>3 monthly follow-ups 1 time, 2 The review will be done semi-annually 1 time in ~5 years and annually after 5 years 1 times. This includes enhanced CT (including neck, chest and abdominal regions) and laboratory tests such as routine blood and biochemistry. Upper gastrointestinal tract imaging, whole-body PET-CT, bone scan, cranial MRI are optional depending on the condition; during follow-up if If suspicious metastases are found in the anastomosis, regional lymph nodes or distant organs during follow-up, upper gastrointestinal endoscopy, fiberoptic bronchoscopy and EBUS-TBNA or EUS-TBNA can be considered as appropriate. New Roman”>EUS-FNA invasive examination of regional enlarged lymph nodes.
-
Follow-up after radical radiotherapy: recommended at the end of radical radiotherapy The recommended frequency of follow-up visits is initially 1 to 2 months after the completion of radical radiotherapy2 years3 reviewed 1 monthly,and2 to 5 yearly review every 6 months 1 times, 5years lateryearly. span style=”font-family:Times New Roman”>1 time. This includes enhanced CT (including neck, chest and abdominal region) and laboratory tests such as routine blood and biochemistry. Upper gastrointestinal tract imaging, whole-bodyPET-CT, bone scan, cranial , and cranial family:Times New Roman”>MRIcan be selected according to the condition; if suspicious metastases in anastomosis, regional lymph nodes or distant organs are found during follow-up, upper gastrointestinal endoscopy, fiberoptic bronchoscopy and < span style="font-family:Times New Roman">EBUS-TBNAor EUS-FNA invasive examination of regional enlarged lymph nodes.
(iii) Systemic drug therapy. .
The clinical symptoms of early-stage esophageal cancer are not obvious and difficult to detect; most patients with esophageal cancer are already at a locally advanced stage or have distant metastases by the time of diagnosis. Therefore, systemic drug therapy aiming at controlling the dissemination occupies an important position in the treatment of esophageal cancer. In recent years, with the emergence and development of new drugs for molecular targeted therapy and immunotherapy, the role of pharmacotherapy in the comprehensive treatment of esophageal cancer is promising.
Currently, the main application areas of drug therapy in esophageal cancer include neoadjuvant and adjuvant therapy for patients with locally advanced disease, and adjuvant therapy for patients with advanced disease. The main areas of application for drug therapy in esophageal cancer include neoadjuvant and adjuvant therapy for locally advanced patients, as well as chemotherapy, molecular targeted therapy, and immunotherapy for patients with advanced disease.
-
Neoadjuvant therapy: neoadjuvant chemotherapy is beneficial for tumor downstaging, eliminating systemic micro-metastases, and observing tumor response to this chemotherapy. and observe the degree of tumor response to this chemotherapy regimen to guide postoperative chemotherapy. For squamous esophageal cancer, locally advanced patients who can be surgically resected can be considered for neoadjuvant chemotherapy, including cTis~ < span style="font-family:Times New Roman">2 N1~3 M0 < or cT3~4a Nany M0 stage cervical and thoracic segment esophageal cancer. Perioperative chemotherapy or neoadjuvant chemotherapy is recommended for surgically resectable locally advanced adenocarcinoma of the lower esophagus and esophagogastric junction, including cTis~. /span>2 N1~3 M0 or cT3~4aNany M0 term or questionable term family:Times New Roman”>cT4b stage adenocarcinoma of the esophagogastric junction.
-
Postoperative adjuvant therapy: esophageal squamous carcinoma Whether adjuvant chemotherapy should be routinely administered after radical surgery remains controversial, and for those with high-risk factors (T4a and N1~3 < span style="font-family:Arial">stage) can be considered for adjuvant chemotherapy or radiotherapy. The evidence for postoperative adjuvant chemotherapy for adenocarcinoma of the lower esophagus and esophagogastric junction comes from studies related to perioperative chemotherapy, and for patients who had preoperative neoadjuvant chemotherapy and completed radical surgery, postoperative adjuvant chemotherapy can be administered with the same regimen.
For patients with esophageal cancer and esophagogastric junction cancer (including squamous and adenocarcinoma) who have received preoperative neoadjuvant radiotherapy and have not achieved pathologic complete remission after radical surgery, treatment with nabumetinumab 1 year significantly prolongs disease-free survival. Currently, the State Drug Administration has not approved nabumetab for adjuvant treatment of esophageal or esophagogastric junction cancer, and it may be the recommended treatment strategy when approved. Adjuvant therapy is usually started after 4 weeks postoperatively.
- Recurrence/< span style="font-family:Arial">Pharmacological treatment of metastatic esophageal cancer: For patients with initially diagnosed advanced metastatic esophageal cancer, systemic drug therapy is feasible if they can tolerate it. In the case of metastatic esophageal cancer, systemic drug therapy is feasible if tolerated.
Progression of metastatic esophageal cancer after systemic therapy may be treated with a different regimen. Systemic drug therapy is feasible for patients who develop local recurrence or distant metastases after radical therapy, if tolerated.
- style=”margin-left: 81pt”>
- First-line therapy.
Currently, immune checkpoint inhibitors in combination with chemotherapy have become the standard of care for first-line treatment of advanced esophageal cancer. For patients with advanced esophageal cancer and esophagogastric junction cancer (both squamous and adenocarcinoma), first-line therapy can be given in combination with pablizumab in addition to cisplatin + fluorouracil chemotherapy regimen; for patients with advanced esophagogastric junction adenocarcinoma, first-line therapy can be given in combination with oxaliplatin < span style="font-family:Times New Roman">+ fluorouracil chemotherapy regimen. span style=”font-family:Times New Roman”>+ fluorouracil in combination with nabolutumab; for patients with advanced esophageal squamous carcinoma, first-line therapy can be given in combination with paclitaxel+ cisplatin chemotherapy; for patients with advanced esophageal squamous carcinoma, first-line therapy can be given in combination with paclitaxel+ cisplatin chemotherapy. span>cisplatin chemotherapy in combination with carrelixumab.
Chemotherapy alone may be considered for patients who are not candidates for immune checkpoint inhibitor therapy. Common chemotherapy regimens for advanced squamous esophageal cancer include cisplatin in combination with fluorouracil and paclitaxel in combination with platinum-based drugs. For advanced esophagogastric junction adenocarcinoma, cisplatin or oxaliplatin in combination with fluorouracil is the common chemotherapy regimen; for patients in good physical condition, a three-drug combination of paclitaxel with platinum and fluorouracil can also be considered as first-line therapy. In patients with HER-2 positive advanced esophagogastric junction adenocarcinoma, first-line therapy can be combined with cisplatin + fluorouracil The first-line treatment can be combined with trastuzumab in addition to a class of drugs.
- style=”margin-left: 81pt”>
- Second-line and beyond.
Immune checkpoint inhibitors have become an important treatment option for patients with advanced esophageal cancer who have failed chemotherapy. For patients with advanced esophageal squamous carcinoma who have failed first-line chemotherapy, either kallikreizumab or tirelizumab may be chosen as second-line therapy. Currently, the State Drug Administration has not approved tirelizumab for second-line treatment of advanced esophageal or esophagogastric junction cancer, and it may be a recommended treatment strategy when approved. For patients with esophageal squamous carcinoma with PD-L1 CPS ≥10 who have failed first-line chemotherapy, second-line therapy can be pablizumab monotherapy; for
patients with adenocarcinoma of the esophagogastric junction who have failed at least second-line chemotherapy, nabolutumab may be an option for third-line and beyond.
Second-line treatment options for patients with advanced esophagogastric junction adenocarcinoma include paclitaxel monotherapy, or irinotecan monotherapy, or docetaxel monotherapy. There is no standard regimen for second-line chemotherapy for advanced esophageal squamous carcinoma, and if immune checkpoint inhibitor therapy is not appropriate, the regimen for adenocarcinoma may be referenced in clinical practice.
In terms of targeted therapy, for HER-2 positive advanced esophagogastric junction cancer, vedicizumab is an option for third-line and beyond. Anti-angiogenic targeted agents are also available as treatment options: third-line and beyond for advanced esophagogastric junction cancer: Apatinib; second-line and beyond for advanced esophageal squamous cancer: Anlotinib or Apatinib.
- style=”margin-left: 57pt”>
- Assessment of relevant tests before systemic drug therapy
-
Assessment of tumor status: pathological type by pathology and cytology, medical history, physical examination, imaging The scope and development trend of the disease should be clarified by medical history, physical examination and imaging to determine the treatment target. Imaging evaluation should be performed prior to treatment and left as baseline information, as appropriate, to facilitate post-treatment comparison of efficacy or long-term follow-up.
-
Assess the patient’s physical condition: the patient should be in general be in good condition,ECOG PS score 0~1 score. See Appendix G for details.
Before the start of treatment 1 week routine blood, liver and kidney function, and electrocardiogram were performed. No significant abnormalities in heart, liver, kidney and hematopoietic functions. Absolute blood neutrophil ≥1.5×109/L, platelets ≥80×109/L, HGB ≥80g/L may be considered for treatment.
-
Assessment of co-morbidities: Patients should be free of serious complications such as active gastrointestinal perforation and bleeding, gastrointestinal obstruction, pulmonary embolism, and shock. If non-neoplastic fever is combined, the temperature should be
<38℃.
If the patient has a combination of cardiac, pulmonary, or other chronic medical disease, relevant tests may be performed depending on the condition, such as: cardiac enzyme profile, brain natriuretic peptide, 24 hour ambulatory electrocardiogram, echocardiogram, pulmonary function tests, etc.
- style=”margin-left: 57pt”>
-
Common systemic drug regimens
- Preoperative neoadjuvant therapy.
- Preoperative neoadjuvant therapy.
-
Fluorouracil< +Folic acid+Oxaliplatin+docetaxel (FLOT) (recommended for adenocarcinoma): oxaliplatin < span style="font-family:Times New Roman">85mg/m2IV drip, day 1, docetaxel 50mg/m2 Intravenous drip, first < span style="font-family:Times New Roman">1 day, folinic acid 200mg/m2 IV drip, day 1 day,day,5-fluorouracil2600mg/m2continuous intravenous drip 24 hours, day 1, every < span style="font-family:Times New Roman">2 weekly repetitions, preoperatively, operatively
4 cycles each after.
- style=”margin-left: 52pt”>
- Fluorouracil+cisplatin (PF).
1) Option 1: 5-Fluorouracil 800mg/m2 continuous intravenous infusion 24 hours, first 1 to 5 days, cisplatin 100mg/m2 intravenously, day 1, every 4 weeks, repeated preoperatively for 2 to 3 < /span> cycles, post-operative 3 to 4 cycles (recommended for adenocarcinoma).
② Option 2: 5-Fluorouracil 1000mg/m2 Continuous intravenous drip 24 hours, first 1 to 4 days and cisplatin 80 mg/m. span style=”font-size:10pt”>2 IV, day 1 every day Roman”>3 weekly repeats, preoperatively for 2 cycles.
- Fluorouracil+cisplatin (PF).
③ Option 3: 5-Fluorouracil 800mg/m2 continuous intravenous drip 24 hours, first 1 to 5
day, cisplatin 80mg/m2 IV drip, day 1 and repeated every 3 weeks, preoperatively 2 cycles
(recommended for squamous carcinoma).
- style=”margin-left: 65pt”>
- Paclitaxel+cisplatin (TPTP family:Arial”>) (recommended for squamous carcinoma).
1) Option 1: Paclitaxel 150mg/m2 IV drip, 1st 1 day, cisplatin 50mg/m2
IV drip, day 1, every 2 weeks repeated.
②Regimen 2: Paclitaxel 135mg/m2 IV drip, day 1, cisplatin 70mg/m2
IV drip, day 1, every 3 weekly repeats.
- style=”margin-left: 65pt”>
- Docetaxel+cisplatin+fluorouracil (DCF) (recommended for squamous carcinoma): docetaxel
70mg/m² IV, day 1 day, cisplatin 70mg/m² IV, day 1, 5- fluorouracil 750 mg/m² intravenously, day 1 to 5 days, repeated every 3 weeks.
- style=”margin-left: 81pt”>
- Postoperative adjuvant therapy.
- style=”margin-left: 65pt”>
-
Navulizumab: Navulizumab 240mg IV drip, first 1day, every
2 weekly repeats, treatment 16 weeks; then, navulizumab 480 mg intravenously, the first 1
day, repeated every 4 weeks. Total treatment duration should not exceed 1 year. (Note: Currently, the State Drug Administration has not approved nabumab for adjuvant treatment of esophageal or esophagogastric junction cancer as a recommended treatment strategy pending approval.)
-
Paclitaxel+cisplatin (TP) (recommended Squamous carcinoma): paclitaxel 150mg/m 2 Intravenous drip, 1st 11 span>day, cisplatin 50mg/m2 Intravenous drip, first 1day, every 2weekly repeats.
- style=”margin-left: 68pt”>
- Late first-line treatment.
- Late first-line treatment.
-
Fluorouracil< span style="font-family:Times New Roman">+Cisplatin (PF) span>):5-Fluorouracil750~1000mg/m2 Continuous intravenous infusion 24 hourly, for the first 1to span>4days, Cisplatin 70~100mg/m2 < span style="font-family:Arial">IV drip 4 hours, 1st 1day, every 3day, every 3day span>~4 weekly repetitions.
- style=”margin-left: 52pt”>
- Paclitaxel-like+Cisplatin (TP >).
1) Option 1: Paclitaxel 135-175 mg/m² intravenously 3 hours, day 1 , cisplatin 75 mg/m² intravenously, day < span style="font-family:Times New Roman">1 day and repeated every 3 weeks.
②Regimen 2: Paclitaxel 90-150 mg/m² IV drip 3 hours, day 1 and cisplatin
50 mg/m² IV, day 1, every 2 weekly repeats.
- Paclitaxel-like+Cisplatin (TP >).
3) Regimen 3: Albumin-bound paclitaxel 125 mg/m² IV, first 1, 8 days, cisplatin 75 mg/m² intravenously on day 1 and repeated every 3 weeks.
-
Oxaliplatin+calcium folinic acid+fluorouracil ( FLO) (recommended for adenocarcinoma): oxaliplatin 85 mg/m²IV drip 2 hour, day 1 day, calcium folinic acid 200mg/m²IV drip
Note 2 hours, day 1, followed by < span style="font-family:Times New Roman">5-fluorouracil 2600 mg/m² by continuous intravenous drip 24
hour, day 1 and repeated every 2 weeks.
-
Docetaxel+cisplatin+fluorouracil (modified) DCF regimen) (recommended for adenocarcinoma): docetaxel 40 mg/m²IV drip1 hour, day 1 day, cisplatin < span style="font-family:Times New Roman">40mg/m²IV drip
1 to 3 hours, day 3, 5-fluorouracil 2000 mg/m² by continuous intravenous drip 48 hours, the first
1 day and repeated every 2 weeks.
-
Iritecan+FluorouracilFluorouracil =”font-family:Arial”>Calcium folinic acid (recommended for adenocarcinoma): irinotecan 180 mg/m² Intravenous drip 30 minutes, 1st 1 day, calcium folinic acid 400mg/m² IV drip, day1 day, “font-family:Times New Roman”>5-fluorouracil 400 mg/m² intravenous push, day 1 day, /span>5-fluorouracil 1200 mg/m² continuous intravenous drip 24 hour, day 1 to 2 days, every day =”font-family:Times New Roman”>2 weekly repetitions.
-
Pabrolizumab+Fluorouracil+cisplatin: pablizumab 200mg IV drip, day 1 day, day, 5- fluorouracil =”font-size:16pt”>800mg/m2 IV drip, day 1 to 5 days, cisplatin80mg/m2 2 size:16pt”>IV drip, day 1 day and repeated every 3 weeks.
- style=”margin-left: 52pt”>
- Navulizumab+Fluorouracil-based+Oxaliplatin (recommended for adenocarcinoma).
1) Regimen 1: Navulizumab 360 mg IV drip, first 1 day and capecitabine 1000 mg/m2 > orally, daily 2 times, days 1 to 14 , oxaliplatin 130 mg/m2 intravenous doses, day 1 >day and repeated every 3 weeks.
- Navulizumab+Fluorouracil-based+Oxaliplatin (recommended for adenocarcinoma).
2) Regimen 2: Navulizumab 240 mg IV, first 1 day, oxaliplatin
85 mg/m2 IV drip, day 1 day, folinic acid 400 mg/m2 < /span>IV drip, day 1.
5-Fluorouracil 400mg/m2 IV, day 1 , 1. span style=”font-family:Times New Roman”>5-fluorouracil 1200mg/m2 Continuous intravenous drip 24 hours, day 1 to 2 days, every 2 weekly repetitions.
- style=”margin-left: 67pt”>
- Karelizumab+paclitaxel+Cisplatin (recommended for squamous carcinoma): carrilizumab
200 mg IV, day 1 >day, paclitaxel 175mg/m2 IV, day 1 day, cisplatin 75 mg/m2 IV drip, day 1 day and repeated every 3 weeks.
- style=”margin-left: 81pt”>
- Late second- and postline therapy.
- Carrilizumab monotherapy: carrilizumab 200mg IV, 1st 1day and repeated every 2 weeks.
- Pabrolizumab monotherapy: pabrolizumab 200mg IV, 1st 1 day and repeated every 3 weeks.
- Navulizumab monotherapy: navulizumab 3mg/kg IV drip, 1st 1 1 “font-family:Arial”>day and repeated every 2 weeks. (Note: Currently, the State Drug Administration has only approved nabolutumab for third-line treatment of advanced or recurrent adenocarcinoma of the esophagogastric junction and gastric cancer, and has not yet approved its indication for second- and second-line treatment of advanced squamous esophageal cancer.)
-
Tirelizumab monotherapy: tirelizumab Tirelizumab monotherapy 200mg IV, 1st 1day and repeated every 3 weeks. (Note: Currently, the State Drug Administration has not approved tirelizumab as an indication for second-line treatment of advanced esophageal or esophagogastric junction cancer, pending approval as a recommended treatment strategy.)
- style=”margin-left: 52pt”>
- Paclitaxel monotherapy.
1) Option 1: paclitaxel 175mg/m2 IV drip, day 1 and repeated every 3 weeks.
②Regimen 2: Albumin-bound paclitaxel 100 to 150 mg/m2 IV drip, first 1, 8 days, repeated every 3 weeks. span>weekly repeats.
- Paclitaxel monotherapy.
③ Option 3: Docetaxel 75 to 100 mg/m2 IV drips, day 1 and repeated every 3 weeks.
- Iritecan monotherapy: Irinotecan 150-180mg/m2 IV drip, day 1 day, every day, every day, every day family:Times New Roman”>2 weekly repetitions.
- Iritecan in combination with Tegeo: Irinotecan < span style="font-size:16pt">160mg/m2IV drip, day 1 day, Tegeo40-60mg orally, daily 2first1-10days, every day. span>2 weekly repeats.
-
Apatinib (recommended for adenocarcinoma): Apatinib 250-500mg orally, continuous.
Efficacy assessment of systemic drug therapy is detailed in Appendix F.
- style=”margin-left: 44pt”>
- Prevention of Treatment-Related Adverse Reactions
Laboratory tests should be performed regularly during treatment according to the characteristics of adverse reactions to the treatment regimen, and appropriate symptomatic supportive therapy should be given when necessary.
Bone marrow suppression, gastrointestinal reactions, and liver and kidney impairment are relatively common adverse effects of chemotherapy. The toxicity profile of immunotherapeutic and targeted therapeutic agents is different from that of chemotherapy and should be taken into account during treatment.
- Prevention of Treatment-Related Adverse Reactions
- Bone marrow suppression: Patients are advised to review weekly after chemotherapy 1 to 2 times after chemotherapy. Depending on the specific chemotherapy regimen and the characteristics of the patient’s blood count, the review interval may be increased or decreased as appropriate. In case of 3, 4degree leukocyte or neutrophil reduction should be discontinued and treated with granulocyte colony-stimulating factor and granulocyte macrophage colony-stimulating factor symptomatically, and the next cycle of chemotherapy delayed or reduced as appropriate. When platelets <50×109/L Interleukin should be given when 11 or recombinant human thrombopoietin, and hemostatic drugs as appropriate. These leukocyte- and platelet-raising agents may also be used prophylactically, depending on the patient’s normative blood results and the characteristics of the chemotherapy regimen.
-
Gastrointestinal reactions: Chemotherapy-related nausea and vomiting: can occur hours or days after chemotherapy. May be given alone or in combination with 5-hydroxytryptamine 3 receptor antagonists, glucocorticoids and neurokinin-1 < span style="font-family:Arial">receptor antagonists and other drugs. Metoclopramide is used in combination with diphenhydramine to enhance the antiemetic effect and to control extrapyramidal reactions. Symptomatic correction of water-electrolyte disturbances due to severe vomiting should be observed.
Decreased appetite: Particularly in postoperative patients, where surgical changes have caused abnormalities in the digestive system, nutritional support should be given more attention during chemotherapy. Nutritional preparations and appetite-enhancing drugs, such as megestrol, can be given orally. Alternatively, a gastric or jejunal nutrition tube may be placed and administered through the tube, with intravenous nutrition support if necessary.
Diarrhea: Avoid cold and coarse fiber-rich foods and take antidiarrheal medications promptly. If you have diarrhea more than 5 times a day or bloody diarrhea, stop chemotherapy and pay attention to adequate rehydration and correction of water-electrolyte disorders.
-
Hepatic and renal impairment: Patients should be informed of any history of hepatitis before chemotherapy. It is recommended that liver and kidney function be reviewed 1 time per chemotherapy cycle. In case of liver impairment, liver function should be fully evaluated and treated with liver-protective medications. Nephrotoxic drugs are contraindicated in renal insufficiency, and when nephrotoxic drugs, such as cisplatin, are administered, care should be taken to hydrate in adequate amounts and attention needs to be paid to drug-drug interactions.
- Neurotoxicity: Prior to administration of drugs such as oxaliplatin, patients should be advised to avoid exposure to cold items and given nerve-nourishing medications. Severe neurotoxicity should be discontinued.
-
Allergic reactions: use of glucocorticoids, < span style="font-family:Times New Roman">H2
receptor antagonists, and pre-treatment with diphenhydramine may reduce the probability of allergic reactions. When using allergy-prone chemotherapeutic agents, the patient should be closely observed within 2 hours after administration and discontinued immediately if allergy occurs, and
- Immune-related adverse reactions: immune Checkpoint inhibitors may trigger immune-related adverse reactions. Patients with a history of autoimmune disease require special caution in treatment decisions. Patients receiving immune checkpoint inhibitors as monotherapy or in combination must be monitored closely. It is recommended that all patients receiving these drugs have routine blood, liver and kidney function, cardiac enzyme profiles, and thyroid function monitored during treatment; adrenocorticotropic hormone and cortisol testing should be considered if patients have nonspecific symptoms such as fatigue; and chest imaging should be considered for symptoms such as shortness of breath, coughing, fever, chest pain, and hemoptysis. If immune-related adverse reactions are diagnosed, immune checkpoint inhibitors may be suspended or permanently discontinued depending on the condition, and the adverse reaction may be treated. Serious adverse reactions such as immune-associated pneumonia and myocarditis can be rapidly fatal and warrant special vigilance and, if necessary, rapid and aggressive immunosuppressive therapy with glucocorticoids.
-
Major Adverse Reactions to Apatinib: Common adverse reactions to Apatinib include proteinuria, leukocytopenia and neutropenia, hypertension, hand-foot syndrome, and elevated transaminases. During treatment with apatinib, blood pressure should be monitored, and routine blood, liver and kidney function, and urine tests should be performed regularly, and the drug should be discontinued and treated symptomatically if necessary.
- style=”margin-left: 44pt”>
- Follow-up after systemic drug therapy
- Follow-up after systemic drug therapy
-
For patients who are surgically resectable and receiving neoadjuvant The efficacy of chemotherapy should be evaluated in a timely manner for patients who can be surgically resected and receive neoadjuvant chemotherapy. A history and physical examination is recommended prior to each cycle of chemotherapy; 2 to 3 cycles later, imaging should be reviewed for efficacy. If the history, physical examination, or imaging findings suggest disease progression, chemotherapy should be discontinued and the resectability of the tumor re-evaluated; for patients with radical resectability, surgery should be performed promptly.
- For patients receiving adjuvant chemotherapy after radical surgery, imaging is recommended after completion of established chemotherapy as there are no clear indicators to observe. If the disease is stable and there are no self-conscious symptoms
situation, within 2 years after the end of treatment, it is possible to Follow-up visits every 3 to 6 months will include history taking, physical examination, review of imaging assessment, and review of routine blood tests, blood biochemistry, and esophageal endoscopy as clinically indicated. From year 3 onwards, follow-up visits can be performed every 6 to 12 months as above. From year 6 onwards, follow-up visits may be made 1 time per year as above.
-
For patients receiving palliative treatment for metastatic esophageal cancer, due to the short median remission period Imaging is recommended after completion of established chemotherapy. If the disease is stable and there are no conscious symptoms, follow-up visits can be performed every 2 months, including history taking, physical examination, review of imaging assessment, and review of blood tests according to clinical needs. The follow-up includes history, physical examination, review of imaging assessment, and review of routine blood tests, blood biochemistry, and esophageal endoscopy according to clinical needs.
(iv) Endoscopic treatment. .
- style=”margin-left: 44pt”>
- Preoperative evaluation of endoscopic treatment of early esophageal cancer
Endoscopic esophageal mucosal resection is recommended for early-stage esophageal cancer without lymph node metastasis. If the depth of esophageal cancer infiltration is assessed pathologically as SM2 or SM3 type, radical esophagectomy is recommended even if there is no regional lymph node metastasis on clinical assessment. Radical surgical esophagectomy is recommended even if there is no regional lymph node metastasis on clinical assessment. Therefore, accurate preoperative determination of the depth of tumor infiltration, extent of involvement, and regional lymph node metastasis is a prerequisite for rational treatment decisions and prognosis. It is recommended to use pigmented endoscopy and electronic staining endoscopy to assess the extent of lesion involvement; ultrasound endoscopy, squamous epithelial IPCL staging, and endoscopic morphologic staging of esophageal tumors to determine the depth of infiltration. Given the lack of guidelines for esophageal endoscopic evaluation and the vulnerability of the endoscopist’s level of experience, it is recommended to rely on post-esophageal mucosal resection pathology for clinical decision making.
- style=”margin-left: 44pt”>
- Principles of endoscopic treatment of early esophageal cancer
Compared with traditional esophageal surgery, endoscopic esophageal mucosal resection for precancerous esophageal lesions or early esophageal cancer is less invasive, has a lower risk of perioperative complications, and is more effective postoperatively than conventional esophageal surgery.
- Preoperative evaluation of endoscopic treatment of early esophageal cancer
Rapid recovery, higher medical economics, and a long-term prognosis approximating that of radical esophagectomy. Endoscopic esophageal mucosal resection is advantageous in terms of balancing clinical diagnosis and treatment with the preservation of esophageal organs to improve patients’ quality of life. It is recommended for patients with cTis ~ 1aN0M0 stage esophageal cancer, including those with severe heterogeneous hyperplasia of the esophageal mucosa, and (M1, M2); esophageal cancer with invasion confined to the epithelial layer of the esophageal mucosa or the lamina propria (M2); involvement of the muscularis mucosa (M3) or submucosal superficial layer (SM1) but without vascular aneurysm emboli or nerve invasion, without peri-esophageal area Lymph node enlargement. If the lesion involves more than 3/4 of the circumferential lumen, endoscopic treatment is not recommended if the experienced endoscopist assesses that the risk of postoperative esophageal scar stenosis is high.
- style=”margin-left: 60pt”>
-
Endoscopic esophageal mucosal resection approach
Mainly endoscopic mucosal resection (endoscopic mucosal resection , EMR), multi-band mucosectomy, multi-band mucosectomy , MBM) and endoscopic submucosal dissection (endoscopic submucosal dissection, ESD).
-
EMR =”font-family:Arial”>:EMR refers to endoscopic excision of whole or divided esophageal mucosal lesions for the diagnosis and treatment of superficial esophageal tumors. Methods include submucosal esophageal injection–lifting–Cutting method based on the gradual evolution of the transparent cap method (EMR with a cap) span>,EMRC), the lancing method (EMR with ligation, , EMRL), piecemeal mucosal resection (endoscopy piecemeal mucosal resection, EPMR) and other technologies. The basic principle of all EMRtechniques is the same, mostly the submucosal layer of the esophagus is separated from the intrinsic muscle layer by submucosal injection, and then different methods are used to remove the localized bulging esophagus. The technique is based on separating the submucosa from the lamina propria by submucosal injection and then removing the localized raised esophageal mucosal lesion using different methods.
EMRC is performed using a transparent cap placed at the front of the endoscope to attract the lesion and then perform a loop resection. EMRL is performed by lancing the lesion, blocking the blood flow and forming a subtip before resection.
clear field of view and less bleeding; EPMR is used for Larger lesions that cannot be completely resected in one pass by conventional EMR , with partial resection of the lesion in stages, for >2 cm of large flat lesions, but the difficulty of in vitro stitching of fractionally excised tissue specimens makes it difficult to assess the radical effect and predisposes to local residual lesions or recurrence.
-
MBMMBM =”font-family:Arial”>:MBMis a modification of the esophageal variceal ligature Multiple mucosal resection technique, which mainly includes the steps of marking, trap removal, and treatment of the wound. Compared to EMR ,MBM MBM does not require submucosal injection and can significantly reduce the operation time. At the same time, MBM is more effective than MBM with the same treatment results. family:Times New Roman”>EMR has the advantages of simple operation, low cost, short treatment time, safe and efficient, which is easy to promote at the grassroots level, and attention should be paid to standardize the operation to avoid lesion residue.
-
ESD:ESD is a submucosal injection for lesions of different sites, sizes and depths of infiltration, followed by A special electric knife is used to gradually separate the tissue between the mucosal layer and the intrinsic muscular layer, leaving the diseased mucosa and submucosal layer intact. The operation is roughly divided into 5 steps: (i) marking around the lesion; (ii) submucosal injection to fully elevate the lesion; and (iii) partial or circumferential mucosal dissection.
④Submucosal dissection to completely separate the mucosa from the lamina propria and remove the lesion in one complete pass.
⑤ Trauma management: including trauma vascular management and lesion margin examination. Classic ESD technology modified by tunneled mucosal dissection (marked –injection – distal opening– proximal dissection– establishment of tunnel –bilateral dissection) can also be used for esophageal mucosal lesions with more extensive involvement.
- style=”margin-left: 48pt”>
-
Common complications of endoscopic treatment and management
Although endoscopic resection is a minimally invasive treatment, it may be complicated by many factors such as the experience level of the endoscopist, the precision of the equipment and instruments, esophageal mucosal disease and the patient’s systemic comorbidities, and other postoperative complications such as esophageal mucosal bleeding, perforation, stricture, and infection The risk is high.
-
-
bleeding: including intraoperative bleeding refers to localized trauma bleeding requiring intraoperative hemostatic treatment (e.g., electrocoagulation or hemostatic clip hemostasis); late postoperative bleeding refers to postoperative bleeding after the operation 30 30 30 30 30 30 . “font-family:Arial”>signs such as vomiting blood, black stool, and hemoglobin drop 20g/L or more within days . EMR The risk of bleeding was positively correlated with the extent of esophageal mucosal lesions, with lesion diameters exceeding 2 cm was associated with a significantly higher risk of intraoperative and postoperative hemorrhage in those with mixed current resection and delayed hemorrhage in those with coagulation current resection. ESD bleeding may be related to lesion site, size and type, level of dissection, degree of lesion adhesion, vascular distribution, and operator proficiency. The bleeding may be related to the lesion site, size and type, level of dissection, degree of adhesion, vascular distribution, and operator skill.
-
Perforation:< span style="font-family:Times New Roman">ESD Intraoperative perforation risk is higher EMR is higher and can usually be detected intraoperatively. If the patient ESD suddenly develops anterior chest and cervicofacial subcutaneous emphysema after surgery, a plain chest radiograph or CT finding mediastinal gas or signs of perforation on examination, etc., should be considered for postoperative perforation. ESD perforation is related to operator experience, lesion location and size, and the presence of ulcer formation at the lesion. The use of CO2 gas and prophylactic clamping of the myocardial rupture during the procedure reduces the incidence of perforation, whereas exposure of the myocardium at the trabecular surface increases the risk of perforation. risk. The accumulation of large amounts of gas in the digestive tract can easily cause small myofibrotic lacerations to form perforations; therefore, the gas in the digestive tract should be suctioned promptly during the operation. Strict indications for endoscopic resection, adequate submucosal injection, and selection of appropriate instruments are also helpful in preventing the occurrence of perforation.
-
Esophageal stricture: refers to the narrowing of the lumen of the esophagus that requires endoscopic treatment after endoscopic esophageal mucosal resection, often accompanied by different degrees of dysphagia. degree of dysphagia, mostly seen about 1 month postoperatively. The extent of esophageal mucosal lesions, depth of infiltration, and circumferential ratio of resected trauma to longitudinal length are common risk factors for postoperative esophageal stricture. The incidence of postoperative strictures in esophageal mucosal lesions larger than 3/4 circumferential esophageal mucosal lesions treated by endoscopic resection can be as high as . style=”font-family:Times New Roman”>88% to 100%.
- style=”margin-left: 52pt”>
- Endoscopic non-mucosal resection treatment
- Endoscopic non-mucosal resection treatment
-
Radiofrequency ablation: Using the thermal effect of electromagnetic wave biophysics to exert treatment The treatment of tumors is achieved by dehydrating, drying and coagulating the tumor tissue. Because the effective treatment depth is limited to 1000 μm range, the risk of postoperative esophageal perforation or stricture is low, and it can be used to treat multiple primary tumors that are intolerant to surgical Multiple primary, single lesions of large extent that are resected or refuse surgery
(Involving the entire circumferential lumen) for precancerous esophageal lesions or early esophageal cancer.
-
Photodynamic therapy, argon ion coagulation, laser therapy, thermal probe therapy, and cryotherapy: these endoscopic non-excisional techniques can be used either alone or in combination with endoscopic resection. Photodynamic therapy is a therapy that uses a specific laser to excite a photosensitizer that selectively accumulates in the tumor tissue to produce monomorphic oxygen, resulting in tumor necrosis through a complex mechanism of physical, chemical, and immune mechanisms. Argon ion coagulation is a non-contact thermal coagulation method that is effective in the management of precancerous esophageal lesions, but its use in early-stage esophageal cancer requires strict indications. The non-excisional approach results in tumor destruction, but no tissue specimens are available for pathologic evaluation or to determine the curative status of the treatment, so close postoperative follow-up is still required and the long-term prognosis remains unclear.
- style=”margin-left: 48pt”>
- Guidelines for follow-up after endoscopic treatment
6 months and 12 months The endoscopic evaluation should be repeated 1 time each month and annually thereafter if there is no recurrence.
Scopy 1 time. Postoperative follow-up is recommended every 3 years for patients with mild heterogeneous esophageal mucosal hyperplasia, 1 times for moderate
Recommended postoperative 1 year follow-up for patients with heterogeneous hyperplasia 1 time. Endoscopic follow-up should be combined with staining and / or magnification endoscopy to find positive or suspicious lesions for selective biopsy and pathological diagnosis. After endoscopic mucosal resection of esophageal lesions, the trauma should be carefully inspected and evaluated with staining or narrow spectral methods if necessary, and if residual lesions are found, repeat esophageal endoscopy should be performed in a timely manner to help reduce the recurrence rate. Localized residual or recurrent esophageal mucosal lesions can mostly be treated by endoscopic
Treatment of localized residual or recurrent esophageal mucosal lesions can be cleared by endoscopy, and additional surgery or radiotherapy can be performed if endoscopic treatment fails. In addition, imaging assessment methods related to esophageal cancer diagnosis and treatment should not be ignored, and one should be alert for multiple primary esophageal squamous carcinomas or second primary carcinomas (e.g., head and neck squamous carcinoma, gastric carcinoma, etc.) at different times.
(v) Guidelines for pathologic evaluation. .
- style=”margin-left: 56pt”>
- Guidelines for specimen type and fixation
- Specimen Types: Common specimen types include endoscopic biopsy specimens,EMR/ESD and radical resection specimens.
-
Specimen fixation: should be timely and adequate, using 10%neutral buffered formalin fixative (containing 4%formaldehyde), which should be fixed immediately (also within half an hour if possible for surgically excised specimens), and the fixative should exceed the volume of the specimen by 10 fold or more, and fixation time 6 to 72 hours. Endoscopic biopsy specimens: After the specimens are separated from the body, the endoscopist or an assistant should use a small poking needle to place the biopsies
The tissue on the examination forceps should be removed immediately and should be spread with a small toggle needle on the finger to take small pieces of filter
Paper, flatten the spreading mucosa on the filter paper and immediately place it in the fixative to fix.
EMR/ESD Specimen: The specimen should be spread by the endoscopist, mucosa side up, and fixed on a cork board (cork board) using a non-rusty fine The specimen should be fixed on a cork board (or foam board) by the endoscopist with the mucosal side up, using a non-rusting fine needle, avoiding excessive stretching that may distort the specimen and should not wrinkle the specimen, marking the oral and anal side orientation, and immediately immersing it completely in the fixative.
Radical resection specimen: open the esophageal wall along the contralateral side of the tumor. The mucosa is pinned mucosa-side up and fixed to a cork board (or foam board) using a large head pin, which should be padded with gauze. The mucosa is pinned mucosa-side down and completely immersed in the fixative as soon as possible (within 30 minutes of separation).
- style=”margin-left: 56pt”>
- Taking and general description guide
- Checking: When taking the specimen, check basic information such as name, sending department, bed number, hospital number, specimen type, etc.
- style=”margin-left: 84pt”>
- Biopsy specimens.
- style=”margin-left: 68pt”>
- Bulk examination and documentation: describe the size and number of tissues sent for examination.
-
Taking: all mucosa sent for examination should be taken The mucosa should be wrapped in filter paper to avoid loss, and a drop of eosin should be added to facilitate the identification of the technician during embedding and sectioning. The different sizes should be separated into different dehydration boxes to prevent small pieces of biopsy tissue from being missed or over-cut. When embedding, it should be noted that the flattened mucosa must be buried vertically (i.e., the mucosa should be buried perpendicular to the bottom of the embedding box). The number of tissue slices in a wax block should not exceed 3 slices, and embedding should be done in a parallel direction (because precancerous esophageal lesions and early-stage cancers are mostly flat, and the determination of the extent of precancerous esophageal lesions and early-stage cancers is not possible. The judgment of the extent of pre-cancerous lesions and early stage cancer depends on the proportion of heterotypic cells involving squamous epithelium and whether there is mucosal lamina propria infiltration, which requires high definition of tissue level. (Only by doing the above two steps of spreading and standing burial can we ensure the clear hierarchy of biopsy tissue on the section, which is crucial to the accurate diagnosis of early esophageal cancer and precancerous lesions). The white edges of the wax block edges that do not contain tissue are removed with a knife as much as possible, and it is recommended that each slide contains 6~8 consecutive tissue slices to facilitate continuous observation.
- style=”margin-left: 44pt”>
- EMR/ESD Specimen
- EMR/ESD Specimen
-
Large body inspection and documentation: Measure and record specimen size (maximum diameter×minimum diameter× thickness), the length and width of the esophagus and stomach should be measured separately for esophagogastric junction specimens. The color of the mucosal surface, the presence of obvious lesions visible to the naked eye, the regularity of the contours of the lesions, the presence of obvious elevations or depressions, the presence of erosions or ulcers, etc., and the size of the lesions (maximum diameter) are recorded.
×minimum diameter × thickness), the general staging and the distance of the lesion from each margin (at least the closest distance between the lesion and the lateral mucosal margin should be recorded). Multiple resected specimens should be reconstructed by the surgeon prior to specimen fixation based on the endoscopic contour of the lesion / without iodine staining (esophageal squamous epithelial lesions). Clinicopathologic communication is recommended for complex specimens or the surgeon may provide a schematic diagram of specimen extension and reconstruction.
-
Taking of material:< span style="font-family:Times New Roman">EMR/ESD Specimens should be taken in their entirety. It is advisable to apply iodine (remove from fixative and rinse for at least half an hour before iodine staining) to identify the lesion (iodine unstained area) and the nearest lateral margin. The material should be taken perpendicular to the nearest lateral cut edge. The lateral mucosal margin and the basal margin can be marked with ink or carbon ink (different colors can be applied to the oral and anal sides for easy identification if possible) to allow localization of the margin during microscopic observation and to evaluate the tumor margin. The esophagogastric junction specimen should be taken in the oral–anal direction to better show the relationship between the tumor and the esophagogastric junction. Each interval 2 to 3 mm is cut in parallel and all the material is retrieved. If the specimen is too large, reshaping can be done by dividing one strip into n strips, marked separately a,b etc. Embedding in the same direction (embedding the cut surface of the first and last slice, and then flipping 180° if the first and last slice have lesions under the microscope) (embedding to ensure that the final section is observed around the mucosal margin) and record the order of embedding corresponding to the tissue block/site. Record the site corresponding to the tissue block (it is recommended to attach a photograph or schematic diagram and mark it well). It is recommended that multiple resected specimens be numbered and retrieved separately, without regard to the lateral margins, otherwise as for single resected specimens.
- style=”margin-left: 44pt”>
- Guide to Radical Resection Specimens
- Guide to Radical Resection Specimens
- Grand examination and documentation: record the length of the resected esophagus at the time of sampling, with or without the esophagogastric junction visible, and the length of the stomach if present. Tumor site (combined with surgery and endoscopy): cervical segment, upper thoracic esophagus, middle thoracic esophagus, lower thoracic esophagus, and esophagogastric junction. The distance of the tumor from the lateral and anal margins of the mouth and the circumferential margin should be recorded. The general tumor staging (including appearance description), size, section color, texture; depth of infiltration; involvement of /non-involved esophagogastric junction (tumor The relationship with the esophagogastric junction: the tumor is completely located in the esophagus and does not involve the esophagogastric junction; the center of the tumor is located in the distal esophagus and involves the esophagogastric junction; the center of the tumor is located in the esophagogastric junction; the center of the tumor is located in the proximal stomach and involves the esophagogastric junction). For those involving the esophagogastric junction, the distance of the tumor center from the esophagogastric junction was recorded as.
cm (for Siewert staging). Esophageal cancer is recommended for reporting in relation to the esophagogastric junction; adenocarcinoma of the esophagogastric junction is recommended for Siewert staging.
-
Taking: iodine coating (removed from fixative and rinsed for at least half an hour before iodine staining) if necessary to identify the lesion (iodine unstained area). For esophageal sampling, a piece of tissue can be taken from the center of the tumor from the lateral oral cut edge to the lateral anal cut edge (including the tumor, the mucosa adjacent to the tumor and the cut edge at both ends) and the orientation of the tissue block should be recorded (photos or diagrams with proper labeling are recommended). It is recommended to take the relationship between the two ends of the cut edge and the tumor longitudinally, and to take the two ends of the cut edge transversely if the tumor is far from the two ends of the cut edge. If the tumor is distant from the two margins, the two margins can also be taken transversely. The closed edges of the occluders should be removed for observation. The deepest tumor invasion and suspected circumferential margin involvement should be taken. The use of ink or carbon ink is recommended to mark the circumferential margins. For early-stage esophageal cancer or radical specimens with insignificant lesions after neoadjuvant therapy, it is recommended to take all the specimens from the suspicious lesions and the tumor bed. Areas with alterations such as surrounding mucosal erosions, roughness or iodine non-staining or surrounding esophageal/nodules in the gastric wall and tissue of the esophagogastric junction should be taken separately. . The grouped lymph nodes sent for examination should all be embedded for sampling. If other adjacent organs such as mediastinal pleura, lung and diaphragm are attached, they should be observed. The recommended tissue size is no larger than 2.0 cm × 1.5 cm × 0.3 cm. Standard second- or third-field clearing and radical surgery specimens without neoadjuvant therapy should detect 15 or more lymph nodes.
- style=”margin-left: 44pt”>
- Pathology Report Content and Guidelines
The pathology report of esophageal cancer should include everything relevant to the patient’s treatment and prognosis, such as specimen type, tumor site, gross staging, size and number, histologic type, subtype and grade, depth of infiltration, vascular and nerve invasion, intramural metastases, surrounding mucosa The tumor site, physical staging, size and number, histological type, subtype and grade, depth of infiltration, vascular and nerve invasion, intramural metastasis, surrounding mucosa, lymph nodes, circumferential and bilateral margins. (y)pTNM staging was noted at the end of the recommended report.
- Pathology Report Content and Guidelines
- style=”margin-left: 87pt”>
- Broad description. Including specimen type, tumor site, gross staging, size
(Tumor size should be measured in three dimensions) and number.
-
Subject tumor: histologic type, subtype and grading (see Appendix B), depth of infiltration (including intramucosal, myxomucosal, submucosal, superficial myxomucosal, deep myxomucosal, cilium, and surrounding tissues or organs. For submucosal invasive carcinoma, the depth of submucosal infiltration (μm) should be measured for endoscopically resected specimens, and it is recommended to differentiate between >SM1-depth of submucosal invasion
<200μm and SM2- Submucosal invasion depth >200μm; in case of radical surgical specimens, it is recommended to differentiate between SM1-mucosal The distinction between superior 1/3, SM2-mucosa in the submucosa 1/3 and SM3-submucosal lower 1/3 ), margins (endoscopic resection specimens include lateral and basal margins; radical resection specimens include oral and anal margins and circumferential margins) (the condition of the margins should be described, including: invasive carcinoma or intraepithelial neoplasia / heterogeneous hyperplasia or Barrett’s esophagus or Barrett’s esophagus with intraepithelial neoplasia /heterogeneous hyperplasia; distance from the incisional margin is recommended; radical resection specimens are recommended with 0, the
<0.1cm and ≥ 0.1cm indicating the distance from the circumferential margin), lymphatic / vessel infiltration (especially for endoscopically resected specimens, if lymphatic / vascular infiltration, immunohistochemistry for CD31, D2-40 is recommended. span>to determine the presence of lymphovascular /vascular infiltration; EVG staining to determine the presence of venous invasion), nerve invasion , intramural metastases.
- paraneoplastic: intraepithelial neoplasia/. span>Heteroplasia and extent, Barrett’s esophagus, with or without esophagitis, gastritis and type.
-
Lymph node metastasis: number of metastatic lymph nodes/Total number of lymph nodes. It is appropriate to report the number of metastatic cancers that invaded outside the lymph node tegument.
- style=”margin-left: 73pt”>
- Pathologic regression response (in cases of neoadjuvant therapy), following the College of American Pathologists
(College of American Pathologists, CAP) criteria, joint residual tumor cell ratio
- Pathologic regression response (in cases of neoadjuvant therapy), following the College of American Pathologists
(see Mandard, Becker, and the Japanese Society for Esophageal Diseases criteria for grading esophageal tumor regression) for pathologic evaluation of specimens after neoadjuvant therapy (Appendix H).
- style=”margin-left: 84pt”>
- Other lesions that are comorbid should be reported.
- For the proposed use ofpatients with esophageal squamous cell carcinoma to be treated with inhibitors, it is recommended that cancer tissue be evaluated for PD-L1 >expressionCPS score. PD-L1(Dako22C3) test has been approved for the indication of esophageal squamous cell carcinoma as a concomitant diagnosis to pabrolizumab therapy to CPS ≥10 as a positive criterion. Esophagogastric junction adenocarcinoma should have HER2 immunohistochemical testing and mismatch repair protein (MLH1, PMS2< span style="font-family:Arial">,MSH2,< span style="font-family:Times New Roman">MSH6
- Guidelines for specimen type and fixation
-
Remarked reports include significant relevant medical history (e.g., relevant tumor history and history of new adjuvant therapy).
(9)(y )pTNM staging.
(vi) Staging integrated treatment model. .
The following is the UICC/AJCC staging (p 8th edition).
1.0 Stage / Precancerous lesions: low-grade intraepithelial neoplasia is recommended for follow-up and may be treated with endoscopic radiofrequency ablation. Endoscopic resection (EMR/ESD/MBM etc.) is recommended for high-grade intraepithelial neoplasia, and endoscopic radiofrequency ablation and cryotherapy are also available depending on clinical conditions. family:Times New Roman”>3/4 cyclic circumference or more, and ESD may lead to recalcitrant stenosis after surgery may also be considered.
-
Stage I:T1a stage endoscopic mucosal resection or mucosal dissection is preferred. If the mucosal resection or mucosal dissection is preferred due to excessive lesion length or involvement of 3/4 circumference or more,ESD may lead to recalcitrant stenosis or suspicious lymph node metastasis after surgery and surgical treatment is recommended. T1b and above stage I preferred Surgical treatment
Treatment. Endoscopic ESD plus postoperative radiotherapy is feasible in cases of poor cardiopulmonary function or refusal of surgery. Completely resected stage I esophageal cancer is generally not treated postoperatively with adjuvant therapy.
-
Stage II: esophageal squamous carcinoma:cT2N0M0 Stage II: Esophageal squamous carcinoma:cT2 N1 M0 andcT3 N0 M0 stage recommended neoadjuvant therapy combined with surgery. Esophageal adenocarcinoma:cT2 N0 M0 stage surgery is preferred,stage family:Times New Roman”>cT1 N1 M0 stage neoadjuvant therapy combined with surgery is recommended. If poor cardiopulmonary function or refusal of surgery, radical radiotherapy is feasible. Preoperative neoadjuvant therapy includes concurrent radiotherapy and chemotherapy.
-
Stage III: Both squamous or adenocarcinoma of the esophagus Neoadjuvant therapy combined with surgery is recommended. For those who have poor cardiopulmonary function or refuse surgery, radical radiotherapy is feasible. For inoperable stage III patients, the current standard of care is concurrent radiotherapy.
- IVAstage squamous or adenocarcinoma:T4a T4astage neoadjuvant therapy combined with surgery is recommended; radical radiotherapy is also feasible for those with poor cardiopulmonary function or who refuse surgery. T4b stage radical radiotherapy is recommended, or chemotherapy alone (invasion of the vertebral body, trachea, aorta, heart and other vital organs).
-
IVBStage IV: Systemic systemic therapy and palliative care are the main focus. For those with good general condition, systemic systemic drug therapy is recommended, combined with local treatment if necessary; for those whose general condition cannot tolerate the above treatment, palliative and supportive treatment is the main means. The aim of treatment is to prolong life and improve the quality of life. Palliative care mainly includes endoscopic treatment (including esophageal dilatation, esophageal stenting and other treatments), pain relief and symptomatic treatment, and nutritional support therapy.
(vii) Treatment guideline chart. .

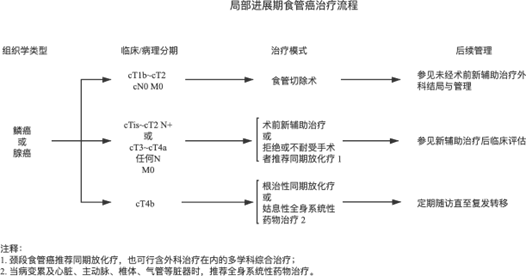
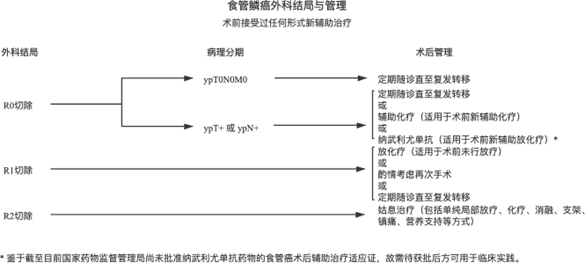
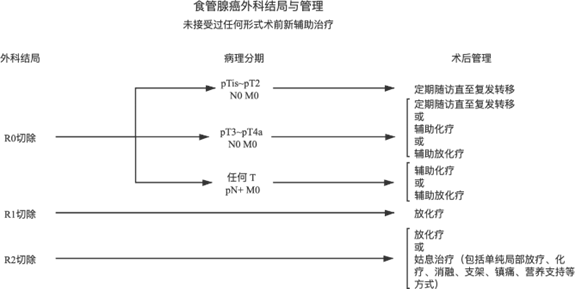
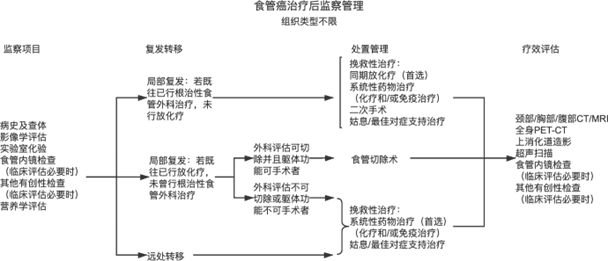
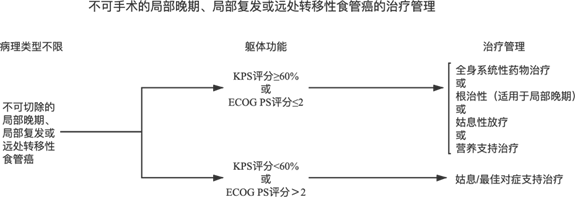
(viii) Nutritional support. .
For those at nutritional risk, a nutritional support program should be developed in a timely manner. Nutrition support is a method of providing appropriate nutrients via enteral or parenteral routes to patients who cannot eat normally. The standardized nutrition support should include elements such as the timing of initiation of nutrition support, route selection, nutrition support target, nutrient selection and monitoring plan. Surgery for esophageal cancer involves upper gastrointestinal tract reconstruction and diminished or lost gastric acid secretion, which has special requirements for postoperative nutritional support therapy.
- style=”margin-left: 60pt”>
-
Indications for nutritional support
(1) Decrease in body mass within 6 months prior to assessment; (> 10%; (2)BMI<18.5 kg/m2.
(3)NRS2002 ≥5 score; (4)SGA rated C grade.
- style=”margin-left: 60pt”>
-
Requirements and pathways for nutritional support therapy
Most patients with nutritional risk for esophageal cancer are well served by nutritional support through fortified diets and oral nutritional supplementation. For NRS2002 scores ≥5 or those with severe malnutrition, if the target amount cannot be met by the oral route Enteral nutrition –tube feeding, supplemental parenteral nutrition or even total parenteral nutrition to improve the patient’s pre-treatment nutritional status and the body’s ability to adapt to stress after treatment.
Indirect calorimetry is recommended for individualized measurement of energy expenditure in oncology patients to guide energy supply when developing nutrition support plans for oncology patients, so that energy intake is as close as possible to the body’s energy expenditure values to maintain energy balance and avoid over- or under-intake. If the actual energy consumption cannot be measured directly to guide nutrition supply, the target energy requirement can be estimated by using the weight formula calculation method, according to 25-30kcal/(kg-d) is provided. Recommended protein supplementation
The amount given should be >1.2 g/(kg-d), which can be increased to 2.0 g/ if the patient has normal renal function.
(kg-d).
There is insufficient evidence on which surgical approach is superior in terms of improving nutritional status and nutritional management, and the impact of the surgical approach depends on the clinical experience of the operator. The preferred postoperative nutritional support therapy is the transgastrointestinal route, either tube feeding and / or transoral. For patients with an intraoperative nutrition line, enteral nutrition can be started within 24 hours after surgery. The enteral nutrition infusion is started at a low rate and increased in moderate increments to the daily target amount as tolerated by the patient.
Postoperative anastomotic fistula requires individualized nutrition support based on the severity of the anastomotic fistula, the patient’s general status, and nutritional needs. In the case of postoperative anastomotic fistula, enteral tube feeding or combined parenteral nutrition via any route can be considered.
- style=”margin-left: 60pt”>
-
Post-discharge home nutritional support therapy
Patients with esophageal cancer still need regular nutritional risk assessment after discharge, and nutritional support is recommended for those with persistent severe malnutrition. The patient’s first choice for post-discharge nutritional support is dietary guidance combined with oral nutritional preparations. For patients with intraoperative indwelling nutritional tubes, the tubes can be retained at discharge for home enteral nutrition. Home nutrition support therapy needs to be done with an experienced nutrition support team
(including physicians, dietitians, pharmacists, nurses, etc.) and is continuously improved.
(ix) Palliative care. .
Palliative care, also known as optimal symptomatic support, is a multidimensional and comprehensive management oriented to improve symptoms and quality of life, and requires, in particular, multidisciplinary collaboration to develop a treatment plan.
- style=”margin-left: 62pt”>
- Eating difficulties
Difficulty eating symptoms often originate from incomplete upper gastrointestinal obstruction, or dysmotility of the GI tract due to esophageal cancer disease itself. There is a lack of standardized swallowing symptom assessment scales to refer to
Guiding clinical practice. Transnasal or gastric / jejunostomy placement may be considered for temporary tube feeding nutritional support or, if no radical esophageal cancer treatment is planned in the future, esophageal stenting may be considered after multidisciplinary discussion.
- style=”margin-left: 62pt”>
-
Complete obstruction
Palliative care for patients with complete upper gastrointestinal obstruction aims to maintain the patient’s daily nutritional intake, based on the creation of an upper gastrointestinal bypass of the gastric Jejunostomy placement is the preferred approach, and experienced endoscopy centers may consider endoscopic balloon dilation of the esophagus, ablation therapy followed by stent placement with membranes, or combined radiotherapy.
- style=”margin-left: 62pt”>
-
Upper gastrointestinal bleeding
Once symptoms of upper gastrointestinal bleeding such as vomiting blood and black stool occur, it indicates that the esophageal cancer disease is nearing the end stage and primary tumor rupture or secondary esophageal –aortic fistula occurs. Endoscopic, interventional, and surgical interventions may be considered as appropriate depending on the medical condition and the patient’s condition. Close monitoring of hemoglobin levels, hemostatic and acid-suppressive drug interventions to prevent severe anemia and hemorrhagic shock.
Appendix A
Recommended Paris staging for early-stage / superficial esophageal cancer (same as early-stage / superficial esophageal cancer Japanese gross staging, i.e. 0 type).
- style=”margin-left: 56pt”>
- Ruminal type (0-Ⅰ): It can also be divided into the tipped augmentation type (0-Ip) and aphthous augmentation ()
(0-Ⅰs).
- style=”margin-left: 56pt”>
- Superficial phenotype (0-II): It can be further divided into superficial elevated type (0-IIa), superficial flat type
(0-IIb) and superficially depressed type (0-IIc). Lesions with both superficial elevation and superficial depression were classified as superficially depressed / according to the ratio of superficial elevation /superficial depression + superficially elevated type (0-II c+II a type) and superficially elevated + superficially depressed (0- >IIa+IIc type).
-
Depressed (ulcerated) type (0-III): lesions with a combination of depressions and superficial depressions according to the depressions/the proportion of superficial depressions was divided into superficial depressions+concave type (0-IIc+Type III) and concave+Table Shallow depressed (0-III) span style=”font-family:Times New Roman”>+IIc type).
Appendix B
Histologic Types of Esophageal Cancer WHO (refer to 2019 edition of WHO Classification of Tumors of the Digestive System)

Histological Type ICD-O >Coding
 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0842_202211.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0842_202211.png" alt=""/>Specific subtypes of squamous cell carcinoma.
Wart-like carcinoma
Spindle cell squamous cell carcinoma Basal cell-like squamous cell carcinoma
Adenocarcinoma, non-specific (NOS) Adenosquamous carcinoma
Adenoid cystic carcinoma
8070/3
8051/3
8074/3
8083/3
8140/3
8560/3
8200/3
Mucinous epidermoid carcinoma 8430/3
Undifferentiated carcinoma, non-specific type ( NOS) Lymphoepithelioma-like carcinoma
Neuroendocrine tumors.
Neuroendocrine tumors (NET), non-specific type (< span style="font-family:Times New Roman">NOS)
NET G1 NET G2 NET G3
Neuroendocrine carcinoma (NEC) Small cell carcinoma
Large cell neuroendocrine carcinoma
Mixed neuroendocrine –non-neuroendocrine carcinoma Complex small cell – adenocarcinoma
Compound small cell –squamous cell carcinoma
8020/3
8082/3
8240/3
8240/3
8249/3
8249/3
8246/3
8041/3
8013/3
8154/3
8045/3
8045/3
 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0842_202213.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0842_202213.png" alt=""/>Appendix C
TNM Staging of Esophageal Cancer (8th Edition UICC/AJCC 2017)


 Esophageal cancer staging in T, N, M of defined primary tumors (T)
Esophageal cancer staging in T, N, M of defined primary tumors (T)TX Primary tumor cannot be evaluated
T0 No evidence of primary tumor
Tis high-grade intraepithelial neoplasia style=”font-family:Times New Roman”>/Heteroplasia
T1 Tumor invading mucosal lamina propria, mucosal muscle layer or mucosa submucosa
T1a Tumor invasion of mucosal lamina propria or mucosal muscle layer
T1b Tumor invasion of the submucosaTumor invasion of the submucosa style=”font-family:Times New Roman”>T2 Tumor invading the lamina propriaT3 Tumor invading the esophageal fibrous membraneT4 Tumor invasion of adjacent structures
T4a Tumor invading pleura, pericardium, odd vein, diaphragm muscle or peritoneum
T4b Tumor invades other adjacent structures such as the aorta, the vertebral body or lymph nodes in the airway region (N)
NX Regional lymph nodes cannot be evaluated
N0 No regional lymph node metastasis
N1 1 to 2 regional lymph node metastasesN2 3 to 6 regional lymph node metastases N3 ≥7 regional lymph node metastases distant metastases (M)
M0 No distant metastases
M1 with distant metastasis
 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0842_202218.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0842_202218.png" alt=""/>Clinical staging (cTNM) prognostic grouping.

Clinical Staging c T N M

Squamous carcinoma

0 TisN0 M0
Ⅰ T1 N0~1 M0
II T2 N0 to 1 M0
T3 N0 M0
III T3 N1 M0
T1~3 N2 M0
IVA T4 N0 ~< span style="font-family:Times New Roman">A T4 N0 ~< span style="font-family:Times New Roman">2 M0
any T N3 M0
IVB anyT Any N M1

Adenocarcinoma

0 TisN0 M0
Ⅰ T1 N0 M0
II A T1 N1 M0
IIB T2 N0 M0
III T2 N1 M0
T3~4a N0 to 1 M0
IVA T1 ~ 4a N2 M0
T4b N0 ~ 2 M0
any T N3 M0
IVB anyT Any N M1

Pathological staging (pTNM) Prognostic grouping.
Pathological staging
p T N M
Histological differentiation
Tumor location
Squamous carcinoma
Squamous carcinoma “border-top: none; border-bottom: solid black 1.5pt”>
0
TisN0 M0
Not applicable
I A
T1a N0 M0
Highly differentiated/Uncertain
any ⅠB
T1b N0 M0
T1 N0 M0 T2 N0 M0
Highly differentiated/Uncertain Medium/ Low differentiation
Highly differentiated
any
any
< td> IIA
>
T2 N0 M0
T3 N0 M0
Mid/ >Low differentiation/Uncertain
any
any
Next paragraph
IIB
T3 N0 M0
T3 N0 M0 T3 N0 M0
Highly differentiated
Mid/Low differentiation uncertain
upper/middle
OnTop/middle section any
T1 N1 M0 any
any
IIIA
T1 N2 M0
T2 N1 M0
any
any
any
any
< td> IIIB
>
T4a N0~1 M0
T3 N1 M0
any
any
any
any
< td> IVA
T2~3 N2 M0
T4a N2 M0
any
any
any
any
< td> T4b N0~2 M0
any
any
anyT N3 M0
< span style="font-family:Arial; font-size:14pt">any
any
< span style="font-family:Arial">IVB
anyT anyN M1
td style=”border-bottom: solid black 1.5pt”>
any
any
>
cancer
0
TisN0 M0
Not applicable
ⅠA
T1a N0 M0
Highly differentiated/uncertain
< span style="font-size:14pt">ⅠB
ⅠC
IIA
T1a N0 M0 T1b N0 M0 T1 N0 M0 T2 N0 M0
T2 N0 M0
Medium differentiation
High/Medium Divergence/uncertain low differentiation
High/Medium Divergence
Low differentiation/uncertain
IIB
T1 N1 M0
T3 N0 M0
any
any
< td> IIIA
>
T1 N2 M0
T2 N1 M0
any
any
< td> IIIB
>
T4a N0~1 M0
T3 N1 M0
any
any
< td> IVA
T2~3 N2 M0
T4a N2 M0
any
any
< td> T4b N0~2 M0
any
< span style="font-size:14pt">anyT N3 M0
<
any
IVB
anyT AnyN M1
td>
any
Notes.
-
To achieve accurate staging, the number of regional lymph nodes should≥15 .
- Tumor site was segmented according to the location of the tumor center (divided into upper, middle and lower segments, upper segment) =”font-family:Times New Roman”>=cervical segment+
- Tumor site was segmented according to the location of the tumor center (divided into upper, middle and lower segments, upper segment) =”font-family:Times New Roman”>=cervical segment+
Upper thoracic segment, middle = middle thoracic segment; lower = lower thoracic + ventral segment).
-
If the tumor involves the esophagogastric junction, the tumor center is on the esophageal side of the esophagogastric junction or 2cmon the gastric side (Siewert I type and II type and II type and type. family:Arial”>type), as per esophageal cancer staging; tumor centered in the proximal stomach 2 cm outside (< span style="font-family:Arial span style="font-family:Times New Roman">Siewert III type) were staged as gastric cancer. If the tumor center is within the proximal gastric 2 cm but does not involve the esophagogastric junction, it is staged as gastric cancer.
-
Basal cell-like squamous cell carcinoma, spindle cell squamous cell carcinoma, small cell The staging of basal cell-like squamous cell carcinoma, spindle cell squamous cell carcinoma, small cell carcinoma, large cell neuroendocrine carcinoma and undifferentiated carcinoma was based on the stage of low differentiated squamous cell carcinoma. Mixed carcinoma with squamous cell carcinoma components (e.g., adenosquamous carcinoma) or those with unclear histologic type are staged as squamous cell carcinoma.
-
Neuroendocrine tumors of the esophagus (<) span style="font-family:Times New Roman">NET) is very rare and its staging is based on that of gastrointestinal neuroendocrine tumorsTNMstaging.
- This staging does not apply to non-epithelial tumors such as lymphoma, sarcoma, gastrointestinal mesenchymal tumors, and melanoma.
-
There are two major international esophageal cancerstages. style=”font-family:Times New Roman”>TNMstaging system. The Western-dominated UICC/AJCC staging considers supraclavicular lymph node metastases to be M1, and the abdominal trunk lymph nodes remain as regional lymph nodes. The Japanese Esophageal Society (JES), on the other hand, considers the supraclavicular lymph node as the regional lymph node for thoracic esophageal cancer, while the trunk lymph node is not the regional lymph node for upper thoracic esophageal cancer. The supraclavicular lymph node is still the regional lymph node of thoracic esophageal cancer, while the trunk lymph node is not the regional lymph node of suprasternal esophageal cancer.
Pathologic staging after neoadjuvant therapy (ypTNM) prognostic subgroups.

Pathological staging after neoadjuvant therapy yp T N M

Ⅰ T0~2 N0 M0
II T3 N0 M0
III A T0~2 N1 M0
IIIB T4a N0 M0
T3 N1 to 2 M0 T0 to 3 N2 M0
IVA T4a N1 ~< span style="font-family:Times New Roman">A T4a N1 ~< span style="font-family:Times New Roman">2, X M0
T4b N0 ~ 2 M0
Any T N3 M0
Any T N3 M0
IVB anyB style=”font-family:Times New Roman”>T Any N M1

Appendix D
Nutritional Risk Screening 2002

- Nutritional status impairment score (highest score)

- min Normal nutritional status
- score (any one) Decrease in body mass in the last 3 months >5%
Decrease in food intake in the last 1 week 25% to 50% 2 score (either) Decrease in body mass >5% in the last 2 months
Decrease in food intake in the last 1 week 50% > to 75% 3 points (any one) Decrease in body mass > 5% in the last 1 month
Decrease in food intake in the last 1 week >75%
Body mass index <18.5kg/m2 with poor general condition

- Disease severity score (increase in nutritional requirements) (highest score possible)

- min Normal Nutritional Requirements
-
score (any one) General malignancy, hip fracture, long-term hemodialysis, diabetes mellitus
Chronic diseases (e.g. cirrhosis, chronic obstructive pulmonary disease)
- Points (any one) Hematologic malignancy, severe pneumonia, major abdominal surgery, stroke
-
score (any one) Critical head injury, bone marrow transplant, critically ill patientAPACHEII score
10 out of 10 span style=”font-family:Times New Roman”>ICU patients

Age Rating

1 min Age ≥70 years

Total Score (A+B+C)

Note: APACHE II is an acute physiology and Chronic Conditions Scoring System II.
Appendix E
Diagnostic Criteria for Malnutrition Initiated by Global (Nutrition) Leaders

- Performance Metrics

Decline in body quality >5% in the last 6 months
or more than 6 months>10%
Low Body Mass Index <70 years. <20 kg/m2, <18.5 kg/m2 (Asian)
≥70 years: <22 kg/m2, <, <20 kg/m2 (Asian) Muscle mass reduction Muscle by validated measurements Reduction results


- Etiology Indicators
 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0842_202242.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_0842_202242.png" alt=""/>Decreased food intake or impaired absorption
Energy intake ≤50% of requirement> 1 week or any degree of intake reduction > 2 weeks
or any digestive disorder that affects the digestion and absorption of food
Inflammatory response Acute illness and trauma
or inflammatory response associated with chronic disease

A and B at least 1 can be diagnosed as malnutrition

Appendix F
Radiotherapy and Chemotherapy Efficacy Determination Criteria
- WHO Solid Tumors Efficacy evaluation criteria.
Complete remission with complete tumor disappearance for more than 1 month.
Partial remission, reduction of the product of the largest diameter of the tumor and the largest vertical diameter up to 50% and no other lesions increasing in size for more than 1 month.
The lesion is stable and the product of the two diameters of the lesion does not decrease by more than 50% >, enlargement of not more than 25% for more than 1 month. Lesion progression with an increase in the product of the two diameter of the lesion by more than 25%.
-
RECISTEfficacy Evaluation criteria.
- Evaluation of target lesions
- Evaluation of target lesions
Complete remission, all target lesions disappeared.
Partial remission with at least a 30% reduction in the sum of the longest diameter of the target lesions compared to baseline status. 30%.
Progression of the lesion with an increase in the sum of the longest diameter of the target lesion compared to the sum of the longest diameter of the smallest target lesion recorded after the start of treatment 20%, or the appearance of one or more new lesions.
Stable lesions, between partial remission and disease progression.
- Evaluation of non-target lesions
Complete remission, disappearance of all non-target lesions and normalization of tumor markers.
Not in complete remission /Stable, with the presence of 1 or more non-target lesions and / or tumor markers persistently above normal.
Progression of lesions with 1 or more new lesions and < span style="font-family:Times New Roman">/ or clear progression of existing non-target lesions.
- Evaluation of best overall outcome
The evaluation of best overall outcome is the smallest value measured between the start of treatment and disease progression or relapse. Typically, the classification of a patient’s best outcome consists of lesion measurement and confirmation.
Appendix G
Patient Condition Score
- style=”margin-left: 48pt”>
- KarnofskyScore (KPS, percent method )

100 normal, no signs and symptoms, no evidence of disease
90 Normal activity with mild signs and symptoms
80 Very barely able to perform normal activities with some symptoms or signs and symptoms
70 can take care of themselves, but cannot maintain a normal life or work
60 Mostly able to take care of themselves, but occasionally need help from others unable to perform normal tasks
50 Needs some help and care, and medication treatment
40 Not able to take care of themselves and need special care and treatment
30 Severely unable to care for themselves, with indications for hospitalization, not yet not yet seriously ill
20 Severe, total loss of self-care, requiring hospitalization and aggressive supportive care
10 Seriously ill, near death
0 Death

- style=”margin-left: 48pt”>
- Zubrod-ECOG-WHO Scoring (ZPS,5 divisions)

- style=”margin-left: 69pt”>
- Normal Activity
- Mild symptoms, self-care, able to perform light physical activities
- Tolerate symptoms of tumor, self-care, but not more than 50%
- Severe tumor symptoms, daytime bed rest more than 50%, but still able to get up and stand, partially self-care
- Seriously ill and bedridden
- Death

Appendix H
Pathologic evaluation after neoadjuvant therapy.
The degree of response to preoperative neoadjuvant radiotherapy/ chemotherapy treatment is closely related to prognosis is closely related.
CAP/NCCN guidelines for post-neoadjuvant Pathology assessment criteria.

Diagnostic criteria Tumor regression grading

No surviving cancer cells 0 (complete response)
Single or small cluster of cancer cells remaining 1 (moderate response)
Residual cancer foci with interstitial fibrosis 2 (mild response) Few or no tumor cells regress; large number of cancer cells remain 3 (poor response)


Notes:1) tumor regression grading can only be assessed in the primary tumor and is not applicable to the assessment of metastatic lesions;2) efficacy assessment is determined based on surviving tumor cells, and keratinized material or mucus lakes without tumor cells that appear after neoadjuvant therapy cannot be considered as tumor residual. The presence of keratinized material or mucus lakes without tumor cells in the lymph nodes cannot be considered as tumor metastasis.
Appendix I:
Terms and Definitions (for this guide)
(a) Esophageal cancer
Cancer of epithelial origin of the esophagus between the beginning of the hypopharyngeal esophagus and the esophagogastric junction. These include the two major types of esophageal squamous carcinoma and esophageal adenocarcinoma, as well as other rare types of malignancies.
- style=”margin-left: 56pt”>
- Squamous cell carcinoma of the esophagus
A malignant epithelial cell tumor originating from the esophageal epithelium and having squamous cell differentiation.
- style=”margin-left: 56pt”>
- Esophageal adenocarcinoma
Malignant epithelial cell tumors with adenoid differentiation mainly originating from the barrette mucosa of the lower 1/3 of the esophagus, and occasionally from the ectopic gastric mucosa of the upper esophagus, or from the intrinsic glands of the esophagus.
(ii) Barrett’s esophagus
Refers to the replacement of the compound squamous epithelium of the lower esophagus by a single layer of columnar epithelium.
(iii) Precancerous disease and precancerous lesions of the esophagus
Pre-cancerous diseases include chronic esophagitis, Barrett’s esophagitis, esophageal leukoplakia, esophageal diverticulum, cardia failure, esophageal ductal pattern, reflux esophagitis, and benign esophageal strictures.
Precancerous lesions are precancerous lesions characterized by heterogeneous squamous cells at different levels within the squamous epithelium of the esophageal mucosa and are classified as low-grade intraepithelial neoplasia according to the level of lesion involvement / heterogeneous hyperplasia (confined to subsquamous epithelium 1/2), high-grade intraepithelial neoplasia / heterogeneous hyperplasia (involving more than lower 1/2 of the esophageal squamous epithelium, previously known as carcinoma in situ).
Appendix J:
Abbreviations (for this guideline)
PET-CT : Positron emission computer tomography (Positron Emission Tomography-Computed Tomography, PET-CT)
IPCL: Intraepithelial Capillary Collaterals of the Esophagus (Intrapapillary Capillary Loops) CLE: Confocal Laser Endomicroscopy (Confocal Laser Endomicroscopy) EUS: Ultrasound Endoscopy (Endoscopic Ultrasonography)
EBUS: Ultrasound Bronchoscopy (endobronchial ultrasound, EBUS) UICC: The International Union for International Cancer Control AJCC: American Joint Committee on Cancer JES: Japanese Esophageal Society
NRS2002: Nutritional Risk Screening 2002 (Nutritional Risk Screening 2002) SGA: Subjective Global Assessment (Subjective Global Assessment)
PG-SGA: Subjective Global Assessment with Patient Participation (Patient Generated Subjective Global Assessment)
GTV: Tumor Target Zone (Gross Tumor Volume)
GTVnd: Lymph node target area (Gross Tumor Volume LymphNode) CTV: Clinical Target Volume (Clinical Target Volume)
PTV: Planning Target Volume (Planning Target Volume)
AUC: Concentration – Area Under The Concentration-Time Curve
CAP: College of American Pathologists CPS: Combined Positivity Score (Combined Positivity Score)
EMR: Endoscopic Mucosal Resection (Endoscopic Mucosal Resection)
MBM: Multi-band mucosal resection (multi-band mucosectomy) ESD: Endoscopic Submucosal Dissection (Endoscopic Submucosal Dissection) RFA: Radiofrequency Ablation (Radiofrequency Ablation)
PDT: Photodynamic Therapy (Photodynamic Therapy) APC: Argon Ion Coagulation (Argon Plasma Coagulation)
Attachments
Esophageal Cancer Treatment Guidelines (2022 Edition) Development and Validation Expert Group
(in order of surname stroke)
Team leader: Greening Wang
Deputy team leader: Yu Jinming, Yu Zhentao, Li Yin
Members: Wang Jun, Wang Guiqi, Wang Feng, Wang Zhen, Wang Xin, Liu Junfeng, Sun Yongkun, Li Zhigang, Li Yong, Chen Kernen, Zhao Xinming, Liu Shuoyan, Jiang Hongjing, Qin Jianjun, Huang Jing
Kang Xiaozheng, Han Yongtao, Hui Zhouguang, Fu Jianhua, Tan Lijie, Xue Liyan
- Guidelines for follow-up after endoscopic treatment

