Lymphoma Treatment Guidelines
(2022 Edition)
Lymphoma is one of the most common malignant tumors in China. According to the World Health Organization GLOBOCAN 2020, the number of new Hodgkin’s lymphoma cases in China in 2020 will be approximately 1.5 million.
(Hodgkin lymphoma, HL) 6829 cases, including 4506 males and 2323 females; 2807 deaths, including 1865 males and 942 females. In 2020, 92,834 cases of non-Hodgkin lymphoma (NHL) were reported in China, including 50,125 cases in men and 42,709 cases in women.
54,351 cases, including 29,721 men and 24,630 women; the incidence and mortality rate of NHL in men ranked 10th among all malignant tumors; the incidence and mortality rate of NHL in women did not rank in the top 10 among all malignant tumors. The incidence and mortality of NHL in women are not among the top 10 malignancies. The lymphoma treatment guidelines have been revised and updated to further improve the diagnosis and treatment of lymphoma and to standardize their implementation, to align with policy adjustments related to antitumor drug supply security, and to ensure medical quality and safety.
The diagnosis should be made in the context of the patient’s clinical presentation, physical examination, laboratory tests, imaging and pathological findings.
The symptoms of lymphoma include systemic and local symptoms. Systemic symptoms include unexplained fever, night sweats, weight loss, itchy skin, and fatigue. Local symptoms depend on the different primary and invasive sites of the lesion, and lymphoma can originate in the body
any organ and tissue of the body, usually divided into two main categories: primary in the lymph nodes and extra-lymph nodes. It most often presents as a painless progressive lymph node enlargement.
Particular attention should be paid to the enlargement of lymph nodes in different areas, the size of the liver and spleen, accompanying signs and general condition.
Laboratory tests to be completed include routine blood work, liver and kidney function, lactate dehydrogenase (LDH), β2 microglobulin , erythrocyte sedimentation rate, hepatitis B virus (HBV), hepatitis C virus, and human immunodeficiency virus testing, and bone marrow aspiration cytology and/or biopsy if necessary. Patients at risk for CNS involvement should undergo lumbar puncture, and cerebrospinal fluid biochemistry, routine and cytology. Peripheral blood EBV DNA titers should be performed for NK/T-cell lymphoma and other EBV-associated lymphomas, such as EBV-positive diffuse large B-cell lymphoma and lymphoma-like granuloma. H. pylori (Hp) testing should be routinely performed for mucosa-associated marginal zone B-cell lymphoma of the primary stomach.
Common imaging methods: CT, MRI, positron emission tomography-computed tomography (PET-CT), ultrasound, and endoscopy.
Staging, restaging, efficacy evaluation and follow-up of lymphoma are still the most
common imaging method, and enhanced CT should be used whenever possible for patients without contraindications to iodine contrast.
MRI is preferred for lesions in the central nervous system, bone marrow, and muscle areas; MRI is optional or preferred for parenchymal organ lesions such as liver, spleen, kidney, and uterus, especially if enhanced CT scan is not indicated or as a further examination after suspicious lesions are detected by CT. The results of this study are not available.
PET-CT is the best test for staging and restaging, outcome evaluation, and prognosis prediction for most lymphomas, but it is not recommended for follow-up during long-term follow-up after disease remission.
It can be used for the diagnosis and follow-up of superficial lymph nodes and superficial organs (testis, thyroid, breast, etc.) lesions, but is not generally used for the staging of lymphoma. For the diagnosis and post-treatment follow-up of superficial lymph node and superficial organ (e.g. testis, breast) lesions, it is advantageous and can be used routinely; for abdominal and pelvic lymph node examination, it can be used selectively; for the evaluation of substantial abdominopelvic organs such as liver, spleen, kidney and uterus, it can be used as a supplement to CT and MRI, especially when enhanced CT examination is not available. During superficial lymph node dissection biopsy, selecting lymph nodes with abnormal sonograms by ultrasound detection can help improve the accuracy of biopsy. Ultrasound-guided puncture biopsy is also used to diagnose lesions in deep lymph nodes, the liver, and the mediastinum.
The lack of characteristic changes in systemic bone imaging in patients with lymphoma bone invasion makes it difficult to differentiate from bone metastases, multiple myeloma, bone tuberculosis, osteofibrodysplasia, hyperparathyroidism, infectious diseases, etc. Infectious diseases need to be differentiated in conjunction with the patient’s history, laboratory tests, and other imaging studies.
Conventional bone scans (99mTc-MDP) have limited clinical value in patients with primary HL, but bone scans need to be combined with CT for post-treatment follow-up and prognostic evaluation of primary bone lymphoma.
It is indicated for patients with suspected gastrointestinal tract invasion, while biopsy can be completed to clarify the pathology.
Pathologic examination is the main tool in the diagnosis of lymphoma. For lymph node lesions, the complete lymph node should be removed if possible. If the lymph node lesion is superficial, the cervical, supraclavicular, and axillary lymph nodes should be selected as much as possible. Coarse needle aspiration should only be used in patients in whom resection or excision of the lesion cannot be obtained effectively and safely. For initial diagnosis, resection or excision of the lesion should be preferred; for recurrent patients, if resected or excised specimens are not available, the diagnosis can be made with lesions obtained by coarse needle aspiration.
The pathologic diagnosis of lymphoma requires a combination of morphology, immunohistochemistry, and a variety of other methods.
(immunohistochemistry, IHC), flow cytometry, and genetic and molecular biology techniques. Also clinical features are very important.
Important in the pathological diagnosis of lymphoma, different types of lymphoma have
characteristic and diagnostic morphologic features. 2.
IHC is used to identify the immunophenotype of lymphoma cells, such as B or T/NK cells, differentiation and maturation of tumor cells. The combination of relevant IHC markers allows for differential diagnosis of different pathological subtypes.
Fluorescence in situ hybridization (FISH) can detect specific chromosomal breaks, translocations, and deletions or amplifications, which can guide the diagnosis of lymphomas associated with specific chromosomal abnormalities, such as t(8. 14) translocations and t(2. 14) translocations associated with Burkitt’s lymphoma; 14) translocations and t(2;8) or t(8;22) translocations associated with Burkitt’s lymphoma, t(14;18) translocations associated with follicular lymphoma, t(11;18) translocations associated with mucosa-associated lymphoid tissue extra-nodal marginal zone lymphoma, t(11;14) translocations associated with mantle cell lymphoma (MCL), and two- or three-strike high-grade B cell lymphoma-associated MYC
(8q24), BCL2 (18q21), and BCL6 (3q27) rearrangements.
Monoclonal rearrangements of lymphocyte receptor genes are a key feature of lymphoma cells and can be used to help distinguish between monoclonal and polyclonal lymphocyte proliferation and lymphomas that cannot be diagnosed by IHC, and are an important complement to morphology and IHC testing.
Including second-generation sequencing, flow cytometry, etc., which are useful supplements to conventional pathology diagnostic methods.
The Ann-Arbor staging (revised at the Cotswolds meeting) is the current common staging system for describing HL and NHL, and is more applicable to HL and NHL in the primary lymph nodes, whereas for some NHL outside the primary lymph nodes, such as chronic lymphocytic leukemia, cutaneous The staging system is difficult to apply to certain NHLs outside the lymph nodes, such as chronic lymphocytic leukemia, cutaneous T-cell lymphoma, and primary gastrointestinal and central nervous system lymphomas, which usually have their own staging systems for NHLs originating in specific extra-nodal organs and sites. In addition, based on data from patients with extranodal NK/T-cell lymphoma in Asia and China, a staging system for extranodal NK/T-cell lymphoma was established, named the Chinese Southwest Oncology Group (CSWOG) and the Asian Lymphoma Collaborative Group
(Asian Lymphoma Study Group (ALSG) staging system, or CA staging. See Annex 2 (Annex 2.1 to Annex 2.5).
Radiation therapy is an important part of comprehensive lymphoma treatment. The choice of radiation beam, radiation field and dose for implementation depends on the treatment purpose and treatment conditions of the specific case. The choice of radiation beam, radiation field and dose is determined by the treatment purpose and treatment conditions of each case. Photon, electron and proton beams can be used to achieve reasonable coverage of the target area and maximum protection of normal tissues. Advanced radiotherapy techniques such as conformal intensity-modulated radiotherapy, breath-holding and breath-gating, image-guided, and proton therapy can significantly reduce the loss of normal tissue while ensuring tumor control.
The indications for radiation therapy for lymphoma can be classified according to the purpose and role of radiation therapy.
① radical treatment; ② consolidation radiotherapy after chemotherapy; ③ relief treatment of chemotherapy intolerant or resistant, residual lesions; and ④ palliative radiotherapy.
Radiotherapy settings are divided into: total lymphatic irradiation and subtotal lymphatic irradiation. Total lymphatic irradiation usually includes the cape field + hoe field + pelvic field (splenic irradiation is also required in cases without splenectomy), while subtotal lymphatic irradiation can omit some of the irradiated areas. Involved-field radiotherapy (IFRT) irradiates only the entire area of the lymph nodes involved prior to chemotherapy, including all known tumor sites and adjacent areas; with the development of diagnostic imaging and conformal radiotherapy techniques, IFRT is being used in HL and aggressive lymphomas to irradiate more precisely the involved lymph nodes or sites of involvement. The IFRT was replaced by more precise irradiation of the involved lymph nodes or involved site radiotherapy (ISRT) in HL and aggressive lymphoma.
ISRT target area definition and outlining.
ISRT Intranodal lesions: ISRT is currently the standard radiation field setting for chemotherapy-sensitive HL and NHL. The target area for ISRT mainly includes lymph nodes involved at the time of initial diagnosis and all areas of suspected tumor involvement before chemotherapy or biopsy procedures, but should exclude adjacent normal tissues that are not invaded, such as lung, bone, muscle, kidney, etc. The pre-chemotherapy or pre-biopsy bulk tumor volume is the basis for outlining the clinical target volume (CTV). Considering the uncertainty of subclinical lesions and the possible lack of accuracy of the original tumor images, the boundaries can be appropriately expanded based on clinical judgment when setting the CTV. When inert lymphomas are treated with radiotherapy alone, a larger field is preferred. For example, follicular lymphoma should be treated with a larger field than diffuse large B-cell lymphoma treated with chemotherapy at the same time of involvement. In the thoracic and abdominal regions, organ motion should be considered to determine the inner target area, on which the planned target area is formed by outward expansion.
ISRT for extra-nodal lesions: The principles of radiation field setting for extra-nodal lesions are similar to those for intra-nodal lesions. However, in some primary lesions of extra-nodal organs, CTV needs to include the entire organ, such as the stomach, salivary glands, and thyroid. In other extra-nodal organs, such as the eye, breast, lung, bone, and skin, partial organ irradiation may be considered. In most cases, prophylactic irradiation of uninvolved lymph nodes is not required.
Radiotherapy dose: 20-30 Gy after complete response (CR) and 36-40 Gy after partial response (PR) for HL chemotherapy. radical for inert lymphoma The dose of irradiation after chemotherapy for diffuse large B-cell lymphoma is 30-36 Gy. The dose of irradiation after PR can be chosen from 36-50 Gy depending on individual factors such as risk stratification and response to chemotherapy and radiotherapy. The radical irradiation dose for extranodal NK/T-cell lymphoma is 50 to 56 Gy.
V. Comprehensive treatment of lymphoma
Integrated multidisciplinary therapy is the principle of treatment for lymphoma. As a group of malignant tumors with different clinical characteristics and different diagnostic criteria and treatment modalities, at the time of diagnosis, the pathological type and molecular pathological features of poor prognosis of lymphoma patients need to be clarified, the disease stage should be clarified by relevant diagnostic imaging techniques, the clinical manifestations and laboratory test results should be integrated, and the prognosis should be judged according to the criteria of respective prognostic risks; the integrated treatment including medical treatment, radiotherapy and necessary surgical treatment should be selected. The choice of comprehensive treatment including medical therapy, radiotherapy and surgery as necessary.
TCM classifies lymphoma into the categories of stone gangrene, malignant nucleus, loss of glory, and phlegm nucleus, and Chinese medicine adopts a combination of disease identification and evidence identification to treat lymphoma.
Qi depression and phlegm blockage, spleen deficiency and phlegm-dampness, qi and blood deficiency, liver and kidney yin deficiency, etc. TCM treatment is based on the principle of holistic concept and evidence-based treatment, taking into account the balance of yin and yang of the whole body as well as tumor reduction and elimination of evil, i.e. “balanced blockage” anti-tumor based on the Jing formula. The combination of chemotherapy and radiotherapy with TCM treatment can reduce the toxicity and increase the effectiveness, reduce the adverse effects of chemotherapy and radiotherapy such as gastrointestinal reaction, bone marrow suppression and peripheral neuritis, and increase the therapeutic effect. For patients who have finished chemotherapy or radiotherapy, Chinese medicine can improve their physical condition and immune function by adjusting the balance of yin and yang in their bodies, thus facilitating their recovery.
Population: patients during chemotherapy and radiotherapy, recovering from antitumor therapy and advanced palliative care.
Treatment: oral tonics, Chinese patent medicines and other Chinese medical treatments (external application, acupuncture, etc.).
HL is a unique malignant disease of the lymphatic system that affects more men than women, with a male-to-female ratio of 1.3:1 to 1.4:1. The age of onset is more typically bimodal in developed countries in Europe and the United States, between 15 and 39 years of age and after 50 years of age, respectively. The age of onset is more typical of a bimodal distribution in developed countries in Europe and the United States, between 15 and 39 years of age and after 50 years of age, while in East Asia, including China, the age of onset is mostly between 30 and 40 years of age, with a unimodal distribution.
- style=”margin-left: 59pt”>
- 90
 of HL has lymph node enlargement as the first symptom, mostly starting from a group of involved lymph nodes, with the cervical and mediastinal lymph nodes being the most common, and gradually spreading to other lymph node areas as the disease progresses, and may involve the spleen, liver, and bone marrow in advanced stages. Patients mostly have no obvious systemic symptoms at the initial diagnosis, and 20
of HL has lymph node enlargement as the first symptom, mostly starting from a group of involved lymph nodes, with the cervical and mediastinal lymph nodes being the most common, and gradually spreading to other lymph node areas as the disease progresses, and may involve the spleen, liver, and bone marrow in advanced stages. Patients mostly have no obvious systemic symptoms at the initial diagnosis, and 20 to 30
to 30 of patients may have B symptoms.
of patients may have B symptoms.
Including unexplained fever, night sweats, and weight loss, there can also be rash, itchy skin, and malaise.
According to the 2017 edition of the WHO Classification of Hematopoietic and Lymphoid Tissue Neoplasms, HL is classified as classical Hodgkin lymphoma (cHL) and nodular lymphocyte predominant type (nodular). The classical type can be divided into four histological subtypes, namely nodular sclerosis, lymphocyte-rich, mixed-cell and lymphocyte-ablative; the nodular lymphocyte-predominant type is rare and accounts for about 10 percent of HL
 .
.HL is a B-lymphocytic tumor of germinal center origin, characterized morphologically by disruption of normal tissue architecture and scattered heterogeneous large cells such as Reed-Sternberg (R-S) cells and variant R-S cells in an inflammatory cell background. Typical R-S cells are binucleated or multinucleated giant cells with eosinophilic, large and distinct nuclei and abundant cytoplasm; if the cells are symmetrically binucleated, they are called mirror cells. LP tumor cells are programmed to die by the protein 1
(programmed death-1, PD-1)-positive T cells. Increasing evidence suggests an overlap between fully diffuse growing NLPHL and large B-cell lymphoma enriched in T cells/histiocytes.
IHC markers that should be routinely tested to diagnose HL include CD45 (LCA), CD20, CD15, CD30, PAX5, CD3, MUM1, Ki-67 index, and EBER. cHL is often
expressed as CD30 (+), CD15 (+) or (-), PAX5 weak (+), MUM1
(+), CD45(-), CD20(-) or weak(+), CD3(-), and in some cases EBER(+) for NLPHL CD20(+), CD79a(+), BCL6(+), CD45
(+), CD3 (-), CD15 (-), CD30 (-), BOB1 (+), OCT2 (+), EBER (-). Additional markers are required for differential diagnosis to identify, for example, mesenchymal large cell lymphoma or diffuse large B-cell lymphoma.
Bone marrow cytology: active or markedly active proliferation of nucleated cells in the bone marrow, with eosinophilia in some cases. If the tumor cells infiltrate the bone marrow, R-S cells characteristic of the disease can be found. The rate of positive R-S cells found on bone marrow aspiration smear is low, only about 3
 ; bone marrow biopsy can increase to 9
; bone marrow biopsy can increase to 9  to 22
to 22 .
.-
NLPHL: Non-cHL with an inert course and occasional late relapses that differ from cHL in terms of natural course and treatment outcome. Most patients have early stage without B symptoms, mediastinal or extra-nodal invasion and large masses. It has the potential to transform into a large B-cell lymphoma. Early stage patients have a good prognosis, while late stage, age ≥45 years, low hemoglobin and B symptoms are associated with a poor prognosis. Because the tumor cells express CD20 antigen, rituximab therapy is effective.
1) Treatment principles for primary patients: early stage, no large mass, no B symptoms with radiotherapy; early stage, large mass or B symptoms with a combination of immunochemotherapy combined with radiotherapy; and late stage with immunochemotherapy. Because of the inert disease course, some advanced patients can choose to be observed and followed up. The first choice is ISRT for stage IA/limited stage IIA without large masses; observation is an option for stage IA patients with complete surgical resection of isolated lymph node lesions.
Large masses, and stage IB/IIB: chemotherapy + rituximab + ISRT recommended. iii
/Stage IV: chemotherapy + rituximab ± ISRT, rituximab alone, palliative radiotherapy for symptomatic localized lesions, or observational follow-up for asymptomatic patients, depending on the patient’s clinical characteristics.
② Treatment options: First-line treatment options: ABVD (adriamycin + bleomycin + vincristine + dacarbazine) + R (rituximab), CHOP (cyclophosphamide + adriamycin + vincristine + prednisone) + R, CVP (cyclophosphamide + vincristine + prednisone) + R, or rituximab rituximab monotherapy. Second-line regimens for relapsed refractory patients may include: R+DHAP (dexamethasone, high-dose cytarabine, cisplatin), R+ICE (isocyclophosphamide, carboplatin, etoposide), R+IGEV (isocyclophosphamide, gemcitabine, vincristine), R+bendamustine; R-CHOP, R-ABVD, R-CVP regimens may also be used if not previously used.
- style=”margin-left: 83pt”>
- cHL.
1) Treatment principles for primary patients: early-stage patients are treated with a combination of chemoradiotherapy and late-stage patients are treated with chemotherapy. The number of chemotherapy cycles, the presence or absence of radiotherapy and the dose of radiotherapy are determined in early stage patients according to factors such as good prognosis, poor prognosis, the presence or absence of large masses and the results of mid-term PET-CT efficacy evaluation. The decision to change the chemotherapy regimen or to reduce the intensity of chemotherapy can be made in patients with advanced disease based on the results of the midterm PET-CT evaluation.
Stage I/IIA, good prognosis, no large masses: The overall recommended treatment strategy is 3 to 4 cycles of ABVD regimen chemotherapy ± ISRT 20 to 30 Gy. If PET-CT is chosen for early efficacy evaluation, the results of 2 cycles of chemotherapy will be used if If PET-CT is chosen for early efficacy evaluation, after 2 weeks of chemotherapy, if the PET-CT efficacy evaluation results in a Deauville score of 1 to 3, it is recommended to continue the ABVD regimen.
1 to 2 weeks ± ISRT 20-30Gy; if Deauville score is 4, continue ABVD regimen with 2 weeks of chemotherapy + If Deauville score is 5, biopsy is required and treatment is based on Deauville score 4 for negative biopsy results and on the treatment strategy for relapsed refractory cHL patients for positive results.
Stage I/IIB, poor prognosis, or large mass: The overall recommended treatment strategy is 4-6 weeks of ABVD regimen chemotherapy ± 30Gy ISRT. If PET-CT is selected for early efficacy evaluation, after 2 weeks of chemotherapy, if the PET-CT efficacy evaluation results in a Deauville score of 1 to 3, it is recommended to continue the ABVD regimen for 2 weeks + ISRT 30Gy or to change to AVD (Adriamycin, Vincristine, Azulfiram) regimen for 4 weeks without radiotherapy; if the Deauville score is 4 to 5, it is recommended to change to intensive BEACOPP (Bleomycin, Etoposide, Adriamycin, Cyclophosphamide, Longitudin). Adriamycin, cyclophosphamide, vincristine, methylphenidate, prednisone) regimen for 2 to 4 weeks ± ISRT 30Gy.
The overall recommended treatment strategy for stage III/IV patients is 6 weeks of ABVD regimen chemotherapy. If PET-CT is selected for early efficacy evaluation, after 2 weeks of chemotherapy, if the PET-CT efficacy evaluation results in a Deauville score of 1 to 3, it is recommended to change to the AVD regimen for 4 weeks; if the Deauville score is 4 to 5, it is recommended to change to the intensive BEACOPP regimen for 3 weeks of chemotherapy, and then to repeat the PET-CT efficacy evaluation, if the Deauville score is still 4 to 3. If the Deauville score is still 4-5, biopsy is required, and those with a negative biopsy continue to complete 1 week of chemotherapy with the BEACOPP regimen, and those with a positive biopsy follow the treatment strategy for patients with relapsed refractory cHL.
First-line treatment options: Recommended treatment options include ABVD, incremental BEACOPP [age <60 years, early PET-CT evaluation of ABVD without CR, advanced HL international prognostic score (IPS) international prognostic score (IPS)
≥4 points].
(3) Treatment strategy and rescue regimen for relapsed refractory patients: The overall treatment strategy for relapsed refractory patients is to select an appropriate second-line regimen for rescue chemotherapy, and after chemotherapy remission, high-dose chemotherapy combined with autologous hematopoietic stem cell transplantation is appropriate
(high dose chemotherapy and autologous stem cell transplantation (HDT/ASCT)) for patients in remission with HDT/ASCT for consolidation ± radiotherapy; patients who are not suitable for transplantation may choose to change their drug regimen, radiotherapy, or observation follow-up depending on the efficacy of the rescue chemotherapy.
Optional second- and later-line regimens include DHAP, ESHAP (etoposide, methylprednisolone, high-dose cytarabine, cisplatin), GVD (gemcitabine, vincristine, liposomal adriamycin), ICE, IGEV MINE (etoposide, isocyclophosphamide, mesylate sodium, mitoxantrone), etc.
The National Medical Products Administration (NMPA) approved vibutuximab on May 14, 2020, for the treatment of relapsed/ The NMPA approved sindilizumab, carrilizumab, and tirelizumab on December 27, 2018, May 29, 2019, and December 27, 2019, respectively, for the treatment of relapsed/refractory cHL after second-line systemic chemotherapy.
- style=”margin-left: 59pt”>
-
-
Adverse prognostic factors in early primary HL: different study groups on early
-
Adverse prognostic factors for early-stage HL vary slightly across study groups.
- style=”margin-left: 83pt”>
-
Adverse prognostic factors for late stage HL: IPS: ① Albumin < 40g/L.
② Hemoglobin < 105g/L; ③ Male; ④ Age ≥ 45 years; ⑤ Stage IV lesions.
⑥White blood cells ≥15×109/L; ⑦Lymphocytes to white blood cells ratio <8
 and/or counts <0.6×109/L.
and/or counts <0.6×109/L.-
Early PET-CT evaluation results: regardless of the early or late staging at diagnosis, PET-CT evaluation after 2 to 3 weeks of chemotherapy with negative results The prognosis of patients with negative results was significantly better than that of positive patients.
Diffuse large B-cell lymphoma (DLBCL) is the most common type of NHL, and accounts for about 60% of adult NHL in Europe and the United States.
30
 to 40
to 40  , with China accounting for 35
, with China accounting for 35  ~50
~50 . The median age of onset of DLBCL is 50 to 70 years, with slightly more men than women.
. The median age of onset of DLBCL is 50 to 70 years, with slightly more men than women. -
Clinical manifestations: The clinical manifestations of DLBCL are varied, depending on the tissues, organs, and tumor load involved. The initial stage of the disease is mostly painless lymph node enlargement, but DLBCL can involve any tissues and organs, and the proportion of extra-lymph node lesions can reach 40
 to 60
to 60 . The clinical course is aggressive and presents as a rapidly enlarging mass. About 1/3 of patients have B symptoms, and LDH is elevated in more than half.
. The clinical course is aggressive and presents as a rapidly enlarging mass. About 1/3 of patients have B symptoms, and LDH is elevated in more than half. -
Pathologic diagnosis and classification: The main pathologic features of DLBCL are large abnormal lymphocytes The main pathological feature of DLBCL is the diffuse growth of large abnormal lymphocytes, which destroy the normal lymph node structure. DLBCL includes multiple variants, subgroups, and subtypes (Appendix 1).
Conventional IHC markers for the diagnosis of DLBCL include CD19, CD20, PAX5, and CD20.
CD3, CD5, CyclinD1, Ki-67; usually manifested as CD19(+), CD20
(+), PAX5(+), CD3(-). After DLBCL diagnosis, to further explore the origin of tumor cells (germinal or non-germinal centers), the Hans model can be chosen
(CD10, BCL6, MUM-1) or Choi model (GCET1, FOXP1, CD10, BCL6, MUM-1), with the addition of CD30, CD138, ALK, etc. for differential diagnosis; routine testing of EBER is recommended for all DLBCL patients to identify EBV EBER to identify EB virus-positive large B-cell lymphoma (non-specific type). IHC testing for C-MYC, BCL2 is recommended routinely for all DLBCL patients, and if C-MYC positivity is ≥40
, BCL2 positivity ≥ 50
 , Ki-67 index > 80 , and IHC testing for C-MYC and BCL2 is recommended for all DLBCL patients. 80
, Ki-67 index > 80 , and IHC testing for C-MYC and BCL2 is recommended for all DLBCL patients. 80  positive, especially for the germinal center cell type, the corresponding FISH test should be added to identify High-grade B-cell lymphoma with MYC, BCL2, and/or BCL6 rearrangements, i.e., “double-hit” or “triple-hit” lymphoma, suggesting a poor prognosis. If FISH is not available, MYC, BCL2, and BCL6 translocations should be evaluated by IHC (cut-off value of ≥40
positive, especially for the germinal center cell type, the corresponding FISH test should be added to identify High-grade B-cell lymphoma with MYC, BCL2, and/or BCL6 rearrangements, i.e., “double-hit” or “triple-hit” lymphoma, suggesting a poor prognosis. If FISH is not available, MYC, BCL2, and BCL6 translocations should be evaluated by IHC (cut-off value of ≥40 ), BCL2 (with a cut-off value of ≥50
), BCL2 (with a cut-off value of ≥50), called “double-expressing” lymphoma, suggests a poor prognosis.
Bone marrow cytology: When DLBCL is infiltrated in the bone marrow, large cytosomes with coarse chromatin, multiple but inconspicuous nucleoli, and gray-blue cytoplasm with a few vacuoles can be seen.
-
Treatment principles: The treatment paradigm for DLBCL is a multidisciplinary and comprehensive treatment based on internal medicine. The treatment strategy should be stratified according to the patient’s age, general status, international prognostic index (IPI) score, clinical stage, presence of large masses and variant subtypes. For patients with high tumor load, they can be given before the start of regular chemotherapy
1 low-dose induction therapy with agents including prednisone±vincristine to avoid tumor lysis syndrome. In patients with HBV carriage or infection, peripheral blood HBV-DNA titers should be closely monitored and antiviral therapy such as entecavir should be selected.
1) First-line treatment for stage I and II DLBCL: for stage I/II patients without large masses, the recommended options are: 3-4 cycles of R-CHOP regimen + ISRT or 6 cycles of R-CHOP regimen ± ISRT; for patients with IPI=0 score, 4 cycles of R-CHOP regimen or 4 cycles of R-CHOP regimen ± ISRT. -CHOP regimen 4 cycles sequential rituximab 2 cycles. The R-CHOP regimen of 6 cycles ± ISRT is recommended for those with large masses in stage I/II.
②First-line therapy for patients with stages III and IV: first recommendation is participation in a clinical trial or 6 to 8 cycles of chemotherapy with the R-CHOP regimen. PET-CT can be performed before, during or at the end of treatment, and the original treatment regimen can be continued or adjusted according to the results. To avoid the impact of false-positive PET-CT, especially mid-treatment PET-CT results, on the determination of efficacy, a repeat biopsy is recommended before changing the treatment regimen.
(3) First-line therapy for patients older than 80 years or frail patients may include the R-miniCHOP regimen, R-CDOP (rituximab, cyclophosphamide, liposomal adriamycin, vincristine, prednisone), R-GemOx (rituximab, gemcitabine, prednisone) monoclonal, gemcitabine, oxaliplatin) or R-GCVP (rituximab, gemcitabine, cyclophosphamide, vincristine, prednisone) regimens. Patients with left ventricular insufficiency may choose the R-CDOP regimen, the dose-adjusted (DA) EPOCH-R regimen (etoposide, prednisone, vincristine, cyclophosphamide, adriamycin, rituximab), the R-CEOP regimen (rituximab, cyclophosphamide, etoposide, vincristine, prednisone), or the R-GCVP regimen.
4) In patients with concurrent CNS invasion, high dose methotrexate (HdMTX) (≥3g/m
) is recommended if the brain parenchyma is involved. (≥3g/m2, administered on day 15 of the 21-day R-CHOP cycle regimen); for meningeal invasion, intrathecal methotrexate/cytarabine is recommended. HdMTX (3 to 3.5 g/m2) can be administered in the same cycle as the R-CHOP regimen or asConsolidation therapy after R-CHOP regimen combined with intrathecal injection therapy.
5 First-line consolidation therapy (elective): Lenalidomide may be considered for maintenance therapy in older patients aged 60 to 80 years.
⑥Rescuing therapy: Rescuing chemotherapy regimens available for patients suitable for HDT/ASCT include: ICE±R, DHAP (dexamethasone, cisplatin, cytarabine)
±R, ESHAP±R, GDP±R, DHAX (dexamethasone, cytarabine, oxaliplatin)±R, GemOx (gemcitabine, oxaliplatin)±R, and MINE± R. For patients who are not candidates for HDT/ASCT For patients not suitable for HDT/ASCT, recommended palliative treatment options include GemOx±R, CEOP±R, DA-EPOCH±R, GDP±R, gemcitabine + vincristine±R, and rituximab alone. Palliative radiotherapy is also a treatment option. Some patients can receive only best supportive care. Allogeneic hematopoietic stem cell transplantation may also be considered in appropriate patients. Patients who have failed second-line or higher rescue therapy may be treated with anti-CD19 Chimeric Antigen Receptor T-Cells (CAR-T).
-
Prognostic indicators: IPI is an internationally used prognostic scoring system for DLBCL. This system is based on 5 independent poor prognostic factors, namely age > 60 years, stage III-IV, number of extra-nodal involvement sites > 1, Eastern Cooperative Oncology Group (ECOG) behavioral status
performance status (PS) score ≥2, and Serum LDH levels > upper limit of normal, 1 point for each adverse prognostic factor. A score of 0 to 1 was considered low risk; a score of 2 was considered low to moderate risk; a score of 3 was considered high to moderate risk; and a score of 4 to 5 was considered high risk. For patients treated with a rituximab-containing regimen, a modified IPI prognostic index can be used. For patients aged ≤60 years, an age-adjusted IPI prognostic index can be used (Appendix 4.2).
In addition to clinical factors, recent advances in molecular genetic studies have shown that “double- or triple-hit” lymphomas with MYC, BCL2, and/or BCL6 rearrangements and TP53 mutations are associated with poor prognosis in DLBCL.
- style=”margin-left: 83pt”>
- Specific primary sites and pathological types of DLBCL.
① Primary CNS DLBCL: One of the subtypes of DLBCL, it refers to DLBCL with intracranial or intraocular origin, excluding dural lymphoma, intravascular large B-cell lymphoma, lymphoma secondary to CNS invasion, and immunodeficiency related lymphomas. Primary CNS DLBCL accounts for less than 1
 of NHL and 2 of primary brain tumors. img src=”https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_202221.png” alt=””/> to 3
of NHL and 2 of primary brain tumors. img src=”https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_202221.png” alt=””/> to 3  . The median age of onset is about 60 years, with slightly more men than women.
. The median age of onset is about 60 years, with slightly more men than women.Clinical presentation: 50
 to 80
to 80 of patients Present with focal symptoms, often with altered mental and response levels; can cause nausea, vomiting, and headache due to increased intracranial pressure. Soft meningeal lesions can cause headaches and asymmetric cranial nerve function abnormalities. Intraocular lymphoma manifests as blurred vision and visual field defects.
of patients Present with focal symptoms, often with altered mental and response levels; can cause nausea, vomiting, and headache due to increased intracranial pressure. Soft meningeal lesions can cause headaches and asymmetric cranial nerve function abnormalities. Intraocular lymphoma manifests as blurred vision and visual field defects.Diagnosis: The imaging presentation is a nodule or mass in the central nervous system. MRI is the examination of choice and reveals a lesion with low or isosignal on T1-weighted images and high signal on T2-weighted images, often with edema. Pathological examination is required to confirm the diagnosis of this
necessary for the diagnosis of this disease, which can be obtained by stereotactic puncture biopsy or cranial biopsy. When tumor biopsy is not available, a positive cerebrospinal fluid cytology is acceptable, and cerebrospinal fluid flow cytometry can be used as an adjunctive diagnostic tool. Differentiating diseases include demyelinating diseases, subacute infarcts and intracranial occupying lesions due to infection, gliomas and metastases. Particular attention should be paid to identifying diseases with similar imaging findings and effective hormonal therapy, such as multiple sclerosis and neurologic nodal disease.
The perivascular infiltrate is more pronounced in primary CNS DLBCL, with tumor cell morphology resembling germinal center mother cells or immunoblasts, essentially originating from non-germinal center B cells, and the proportion of Ki-67-positive cells often exceeding 90< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_202225.png" alt=""/>. IHC markers are the same as for DLBCL.
Treatment: A combination of medical therapy is the mainstay. Corticosteroids provide rapid relief, but without chemotherapy or radiotherapy, the tumor often recurs within a short period of time. Corticosteroids are not recommended before biopsy of tumor tissue, except in cases of life-threatening intracranial hypertension. The principle of chemotherapy is to cross the blood-brain barrier, and HdMTX is preferred. Patients who achieve CR/CRu with first-line therapy may undergo consolidation therapy including HDT/ASCT, HdAra-C ± etoposide or whole brain radiotherapy. Patients with relapse resistance may be treated with single or combination regimens of HdMTX or HdAra-C, temozolomide, topotecan, pemetrexed, ibrutinib, and lenalidomide. HDT/ASCT may be considered for patients with effective rescue therapy, and for primary CNS lymphoma, a combination regimen with tiotipine is recommended for pretreatment with autologous hematopoietic stem cell transplantation.
Combination of whole-brain radiotherapy after chemotherapy may prolong progression-free survival in patients
(progression free survival, PFS). However, the neurotoxicity of whole-brain radiotherapy is more pronounced in patients >60 years of age, so it is recommended that radiotherapy be deferred in patients >60 years of age after remission from chemotherapy. The role of surgery is limited to biopsy, and complete removal of the tumor is not beneficial.
Prognosis: The disease is highly malignant, with a median survival time of only 2 to 3 months with supportive therapy, 3 to 5 months with surgery alone, approximately 12 to 16 months with radiotherapy alone, and 25 to 84 months with HdMTX-containing regimens of chemotherapy. The most important prognostic factors are age and behavioral status.
②Primary testicular DLBCL: Primary testicular DLBCL accounts for 3
 ~
~9
 , accounting for 1
, accounting for 1 to 2
to 2  . DLBCL is the most common pathological type of primary testicular lymphoma, accounting for 80. https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_202230.png” alt=””/> to 90
. DLBCL is the most common pathological type of primary testicular lymphoma, accounting for 80. https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_202230.png” alt=””/> to 90 . It is the most common testicular malignancy in men over 50 years of age, with a median age of onset of approximately 65 years.
. It is the most common testicular malignancy in men over 50 years of age, with a median age of onset of approximately 65 years.Clinical presentation: mostly painless swelling or swelling of the testes, with a few presenting as scrotal pain. Bilateral testicular involvement at the time of diagnosis accounts for about 20
 and up to 35
and up to 35of patients have invasion of the contralateral testis during the course of the disease. Those with enlarged retroperitoneal lymph nodes may present with abdominal pain and peritoneal effusion. b Symptoms are usually seen only in patients with advanced disease. The disease is associated with extra-nodal organ involvement, including the central nervous system, skin, subcutaneous tissues, lungs and pleura. The ultrasound findings are: an enlarged testis with a well-defined shape and a limited or diffuse hypoechoic area in the testis with clear or indistinct borders, with a rich blood supply on ultrasound and normal testicular vascular penetration within the lesion.
Treatment principles: Primary testicular DLBCL should be treated with a combination of surgery, radiotherapy, and immunochemotherapy. Patients should undergo orchiectomy and high spermatic cord node
Ligation, which should be followed by immunochemotherapy. Because of the high rate of contralateral testicular and CNS invasion, prophylactic radiotherapy of the contralateral testis and prophylactic treatment of the CNS with HdMTX are recommended. ISRT may be performed in stage II patients.
Prognosis: Poor prognostic factors for this disease include advanced age, advanced stage, elevated LDH, B symptoms, high IPI, and absence of surgery or radiotherapy.
(3) Primary mediastinal large B-cell lymphoma: Most often seen in young adults, with a median age of onset around 35 years and slightly more women than men. The tumor cells originate from thymic B cells and have their own unique gene expression profile, which is more similar to that of cHL. Clinical manifestations: clinical symptoms and signs are mostly associated with rapidly enlarging mediastinal masses.
These are associated with superior vena cava compression syndrome, pericardial effusion, and pleural effusion. The lesions are often limited at initial diagnosis, mainly in the anterosuperior mediastinum, and may be associated with supraclavicular, cervical, and hilar lymph node involvement; recurrence is often associated with extensive extra-nodal organ or tissue invasion.
Treatment principles: The choice of first-line chemotherapy regimen is controversial. The options include DA-EPOCH-R, R-CHOP, or R-CHOP sequential R-ICE. chemotherapy
Consolidation radiotherapy is feasible after chemotherapy and may be considered without radiotherapy for those with negative PET-CT evaluation. The nature of the residual mass cannot be accurately determined by CT examination because of the residual mass in the anterior mediastinum after chemotherapy, so PET-CT is recommended for evaluation at the end of chemotherapy. However, the false-positive rate of PET-CT is high, and a repeat biopsy is recommended if a change in chemotherapy regimen is considered based on PET-CT results. The treatment of relapsed refractory patients can be based on the treatment strategy for relapsed refractory DLBCL.
Prognosis: The prognosis is better than that of non-specific DLBCL, with a 5-year PFS of
80
 to 95
to 95  . Adverse prognostic factors refer to DLBCL.
. Adverse prognostic factors refer to DLBCL.④ High-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 translocations (double/triple whammy lymphoma): defined as high-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 translocations detected by FISH, containing MYC translocations and BCL2 or The lymphomas with MYC translocation and BCL2 or BCL6 translocation were double-hit, and those with all three translocations were triple-hit lymphomas. It accounts for about 2
 to 11 of DLBCL
to 11 of DLBCL  , most of which are of germinal center B-cell origin.
, most of which are of germinal center B-cell origin.Clinical features: highly aggressive features, commonly elevated LDH, bone marrow invasion, CNS invasion, and high IPI scores.
Treatment principles: There is no recommended standard of care, and participation in clinical trials is recommended first. Recommended regimens include DA-EPOCH-R, R-HyperCVAD/HdMA (rituximab, cyclophosphamide, vincristine, adriamycin, and dexamethasone alternating with HdMTX and HdAra-C) and R-CODOX-M/IVAC (rituximab, cyclophosphamide, vincristine, adriamycin and methotrexate, isocyclophosphamide, etoposide, and cytarabine). , and cytarabine). For patients with limited stage, consolidation radiotherapy is recommended. High rate of CNS invasion and CNS prophylaxis is recommended.
Prognosis: The prognosis is poor. In a retrospective study with long follow-up and treatment with the R-CHOP regimen, the 5-year progression-free survival and overall survival rates were 18
 and 27
and 27 , respectively. In another meta study comparing the efficacy of R-CHOP, R-HyperCVAD or R-CODOX-M/IVAC and DA-EPOCH-R regimens as first-line therapy, the median PFS was 12, 19 and 22 months in the three groups, respectively. The DA-EPOCH-R regimen significantly prolonged the PFS of patients compared with the R-CHOP regimen.
, respectively. In another meta study comparing the efficacy of R-CHOP, R-HyperCVAD or R-CODOX-M/IVAC and DA-EPOCH-R regimens as first-line therapy, the median PFS was 12, 19 and 22 months in the three groups, respectively. The DA-EPOCH-R regimen significantly prolonged the PFS of patients compared with the R-CHOP regimen.Follicular lymphoma (FL) is the most common inert lymphoma in Europe and the United States, accounting for approximately 20 percent of NHL
 ~30
~30  , the prevalence in Asia, including China, is low, less than 10 percent of NHL
, the prevalence in Asia, including China, is low, less than 10 percent of NHL . The median age of onset is about 60 years.
. The median age of onset is about 60 years.-
Clinical manifestations: mainly multiple lymph node enlargement, also involving bone marrow, peripheral blood, spleen, pharyngeal lymphatic ring, gastrointestinal tract, and soft tissue. The primary nodes are rare. It is more common in patients with advanced disease, accounting for about 70
 .
. -
Pathologic diagnosis: morphologically, there is a proliferation of follicular center cells and center mother cells, mostly follicle-like nodular growth. According to the number of centroblasts, FL is classified into 3 levels: 0-5 centroblasts per high-powered view is level 1, 6-15 is level 2, and more than 15 is level 3. FL level 3 can be further divided into level 3a and level 3b, where 3b shows a lamellar distribution of centroblasts and lack of centroblasts. IHC markers that should be routinely tested for the diagnosis of FL include CD19, CD20, PAX5, CD3, CD10, BCL2, BCL6, LMO2, CD21
and Ki-67, but also markers needed for differential diagnosis, such as CD23, CD5, and cyclin D1 for chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) and MCL. FL often has t(14;18) translocations and resulting Bcl2 protein overexpression, but there is varying degrees of loss with increasing grade, making it difficult to confirm the diagnosis, and FISH BCL2 testing can be performed when necessary.
Pediatric-type follicular lymphoma (PTFL) is a type of lymph node disorder that occurs primarily in children and young adults.
The 2017 edition of the WHO Classification of Tumors of the Hematopoietic and Lymphoid Tissues newly introduced “duodenal follicular lymphoma,” which has a good prognosis and needs to be distinguished from FL in other gastrointestinal anatomic sites; the newly introduced “large B-cell lymphoma with IRF4 gene rearrangement,” which occurs in the pharyngeal lymphatic ring and cervical lymph nodes and is common in children and young adults. The newly proposed “large B-cell lymphoma with IRF4 gene rearrangement”, which occurs in the pharyngeal lymphatic ring and cervical lymph nodes, is more common in children and young adults, and has a histologic presentation consistent with classic high-grade FL, with IHC showing IRF4+/CD10+/BCL6+ and FISH showing IRF4 rearrangement. In addition, the previous in situ follicular lymphoma was changed to in situ follicular neoplasm. Bone marrow cytology: When the tumor cells involve the bone marrow, nucleated cell proliferation can be significantly active, mainly with an increase in FL cells, which are larger than normal lymphocytes, with round or irregular nuclei, fine nuclear chromatin, faintly visible nucleoli, abundant cytoplasm and light blue color, and some FL cells with vacuolar degeneration. The diagnosis of FL is based on pathologic histology.
-
Treatment: Grade 1 to 2 FL is an inert lymphoma, and depending on the stage, the treatment strategy is as follows. Grade 3 FL is treated as DLBCL.
Stage I/II FL: Patients with stage I/II have a potential cure with radiotherapy. In stage I and stage II patients with limited lesions and no large masses, radiotherapy is the mainstay. Treatment is preferred to ISRT, or ISRT + CD20 monoclonal antibody ± chemotherapy; in special cases where radiotherapy is not possible, CD20 monoclonal antibody ± chemotherapy can be chosen. Stage I with a large mass or
Stage II patients with extensive lesions, refer to the treatment strategy of stage III/IV, and recommend mainly medical treatment with CD20 monoclonal antibody±chemotherapy±palliative ISRT, or in the absence of treatment indications observational follow-up.
②Stage III/IV FL: Stage III/IV FL is considered to be an incurable disease. In stage III/IV FL with low tumor load, there is no difference in patient OS when treated immediately after diagnosis versus observational follow-up and treatment when indicated.
Patients without indication for treatment may have a physical or laboratory examination every 3 to 6 months for 5 years and once a year after 5 years, and a CT examination ≥6 months for 2 years and ≥1 year after 2 years.
Patients with indications for treatment need to be treated. Indications for treatment include availability for appropriate clinical trials, high tumor load, symptomatic, organ function threatening, secondary hematocrit, large masses, and persistent lesion progression.
FL’s recommended first-line regimens include R-B (rituximab, bendamustine), R-CHOP or G-CHOP (otuzumab, cyclophosphamide, adriamycin, vincristine, prednisone), R-CVP (rituximab, cyclophosphamide, vincristine, prednisone) monoclonal, cyclophosphamide, vincristine, prednisone) or G-CVP (otuzumab, cyclophosphamide, vincristine, prednisone) and R-R (rituximab, lenalidomide). Rituximab monotherapy is an option for some patients with low tumor load. In elderly and frail patients, single agent rituximab, or single agent alkylating agents (e.g., nitrogen mustard phenylbutyrate, cyclophosphamide) ± rituximab, etc. are recommended. In patients with primary, high tumor load, rituximab maintenance therapy may prolong PFS after induction chemotherapy to achieve CR or PR.
③ Treatment of relapsed refractory FL: Watchful follow-up remains preferred for relapsed FL when
Treatment is indicated before starting rescue therapy. The histologic transformation should be highly suspected when the standard uptake values on PET-CT are significantly higher.
Rituximab therapy can be continued if relapse progression occurs more than 6 months after the last dose of rituximab. Depending on the first-line regimen, recommended second-line regimens include R-B, R-CHOP, R-CVP, or R-R. For patients with progression of disease (POD) within 24 months of the start of first-line treatment with R-CHOP or R-CVP regimens, lenalidomide-based regimens, participation in clinical trials, or HDT/ASCT are recommended as consolidation therapy. Rituximab maintenance therapy is also an option after remission with second-line induction chemotherapy. Anti-CD19 CAR-T therapy is an option for patients who fail second-line and above.
About 15
 Histologic conversion to DLBCL can occur in about 15
Histologic conversion to DLBCL can occur in about 15 of FL, with an annual conversion rate of
of FL, with an annual conversion rate of2
 ~3
~3  . Risk factors associated with histologic transformation include late stage, high follicular lymphoma international prognostic index (FLIPI), increased LDH, and B symptoms. Active treatment and follow-up have no significant impact on the rate of conversion. The prognosis of transformed FL is usually poor, and factors such as staging at the time of transformation, whether the patient has received chemotherapy or rituximab prior to transformation, and whether the patient is transformed to double- or triple-hit DLBCL are associated with prognosis. Treatment of transformed FL is referenced to DLBCL.
. Risk factors associated with histologic transformation include late stage, high follicular lymphoma international prognostic index (FLIPI), increased LDH, and B symptoms. Active treatment and follow-up have no significant impact on the rate of conversion. The prognosis of transformed FL is usually poor, and factors such as staging at the time of transformation, whether the patient has received chemotherapy or rituximab prior to transformation, and whether the patient is transformed to double- or triple-hit DLBCL are associated with prognosis. Treatment of transformed FL is referenced to DLBCL.④Prognosis: FLIPI has two scoring systems, FLIPI1 and FLIPI2, with a score of
containing 5 independent poor prognostic factors, both of which classify patients into 3 risk groups.
The FLIPI1 scoring system score of 0 to 1 was the low risk group, 2 was the intermediate risk group, and ≥3 was the high risk group; the FLIPI2 scoring system score of 0 was the low risk group, 1 to 2 was the intermediate risk group, and 3 to 5 was the high risk group (Appendix 4.3). event-free survival after POD24 or first-line immunochemotherapy was An event-free survival time of ≤12 months after POD24 or first-line immunochemotherapy is indicative of a poor prognosis. In one study, the 5-year overall survival rate for POD24 and non-POD24 patients after first-line treatment with R-CHOP regimen was 50
 and 90
and 90 .
.Marginal zone lymphoma is a B-cell lymphoma that originates from the marginal zone and is an inert lymphoma. There are three subtypes according to the site of origin: extra-nodal marginal zone lymphoma [also known as mucosa-associated lymphoid tissue (MALT) lymphoma], lymph node marginal zone lymphoma, and splenic marginal zone lymphoma. Of these, MALT lymphoma is the most common.
The etiology of marginal zone lymphoma is associated with persistent immune stimulation due to chronic infection or inflammation. For example, gastric MALT lymphoma is associated with chronic infection with Hp, thyroid MALT lymphoma is associated with Hashimoto’s thyroiditis, parotid MALT lymphoma is associated with desiccation syndrome, and hepatitis C virus infection is associated with marginal zone lymphoma of the lymph nodes and splenic marginal zone lymphoma.
The pathologic diagnosis of marginal zone lymphoma is more of an exclusionary approach, with nonspecific immunomarkers that require the exclusion of other types of small B-cell lymphomas, and CD21 and CD23 often showing an expanded FDC network. The pathology often shows clonal proliferation of small lymphocytes, causing widening of the marginal zone, atrophy of the germinal center, follicular “implantation” and lymphoepithelial lesions.
- style=”margin-left: 83pt”>
-
MALT lymphoma: The most common primary site of MALT lymphoma is the stomach. primary site is the stomach
Intestinal tract, with gastric primary accounting for about 80
 ~85
~85  . About 2/3 of patients have limited stage, 1/3 have extensive stage, and the percentage of bone marrow invasion is about 10
. About 2/3 of patients have limited stage, 1/3 have extensive stage, and the percentage of bone marrow invasion is about 10 to 15
to 15  .
.1) Gastric primary MALT lymphoma: clinical features: symptoms include dyspepsia, acid reflux, abdominal pain and weight loss, B symptoms are uncommon, and gastric bleeding is about
20
 to 30
to 30  , perforation ratio of about 5
, perforation ratio of about 5  ~10
~10  . Stage I and II patients account for 80
. Stage I and II patients account for 80 to
to90
 , 90 , 90
, 90 , 90  of patients are Hp-positive. Gastroscopy may show erythema, erosion, and ulceration of the gastric mucosa.
of patients are Hp-positive. Gastroscopy may show erythema, erosion, and ulceration of the gastric mucosa.Pathologic diagnosis: Gastric MALT lymphoma requires gastroscopic biopsy for pathologic diagnosis and routine Hp staining. MALT lymphoma typically has a dense proliferation of small lymphocytes that in most cases infiltrate and disrupt the mucosal epithelium, forming a lymphoepithelial lesion. IHC markers include CD3, CD5 MALT lymphoma can be diagnosed after excluding FL, CLL/SLL and MCL, in combination with morphology and B-cell phenotype. In a few cases, PCR-Ig assay was required to obtain monoclonal evidence to confirm the diagnosis. To determine whether a gastric MALT lymphoma is Hp-dependent, t(11;18) translocations can be detected by FISH or PCR, and t(11;18) translocations are indicative of poor anti-Hp therapy. The diagnosis of DLBCL with MALT lymphoma should be made when bulky transformed lymphocytes show solid or sheet-like hyperplasia.
Treatment principles: Stage I/II: anti-Hp therapy is recommended for Hp-positive, t(11;18)-negative or unknown patients; anti-Hp therapy in combination with ISRT is preferred for Hp-positive, t(11;18)-positive patients; anti-Hp in combination with ISRT is also preferred if radiotherapy is contraindicated. Anti-Hp therapy in combination with rituximab is also an option if radiotherapy is contraindicated. For patients who are not responding to anti-Hp therapy or are Hp-negative, ISRT is recommended, and for patients who are not candidates for radiotherapy, rituximab alone may be chosen.
Drug therapy. After anti-Hp therapy, the first gastroscopy review can be done after 3 months, and if the gastroscopy suggests remission of the lesion, gastroscopy can be performed every 3-6 months thereafter. stage IIE, III/IV: Those without indications for treatment can opt for observation and follow-up, and those with indications for treatment refer to the principles of treatment for stage III/IV FL, and surgical treatment is limited to exceptional cases such as the occurrence of hemorrhage and perforation.
②Non-gastric primary MALT lymphoma: Clinical features: Non-gastric primary MALT lymphoma presents an inert course with a prognosis similar to that of gastric primary MALT lymphoma. Common sites of non-gastric primary MALT lymphoma include salivary glands, lung, head and neck, ocular appendages, skin, thyroid, and breast.
Treatment principles: ISRT or surgery is preferred for stage I/II. Those who may have serious complications due to treatment may also be treated with observational follow-up or rituximab monotherapy. For stage III/IV, refer to the treatment strategy for stage III/IV FL.
-
Lymphoma of the lymph node marginal zone: clinical features: 1.5 of all lymphomas
 ~1.8
~1.8  , with a median age at presentation of 60 years and similar proportions of men and women, and a prevalence of advanced lesions. It mainly involves the lymph nodes, but occasionally the bone marrow and peripheral blood. Most patients present with painless multiple lymph node enlargement, with the exception of patients with MALT lymphoma or splenic marginal zone lymphoma with lymph node involvement.
, with a median age at presentation of 60 years and similar proportions of men and women, and a prevalence of advanced lesions. It mainly involves the lymph nodes, but occasionally the bone marrow and peripheral blood. Most patients present with painless multiple lymph node enlargement, with the exception of patients with MALT lymphoma or splenic marginal zone lymphoma with lymph node involvement.Pathologic diagnosis: Similar structural features to splenic marginal zone lymphoma, non-specific immunophenotype, similar to other subtypes of marginal zone lymphoma.
Treatment principles: refer to the treatment principles of FL.
Prognosis: 5-year overall survival rate of 60
to 80
 , prognosis can be determined by referring to FLIPI.
, prognosis can be determined by referring to FLIPI.- style=”margin-left: 72pt”>
- Lymphoma of the splenic marginal zone: clinical features: accounts for 2
 , in
, in
The median age of onset is 50 years, with equal proportions of men and women. The spleen and splenic hilar lymph nodes are often involved.
- Lymphoma of the splenic marginal zone: clinical features: accounts for 2
It also frequently involves the bone marrow, peripheral blood, and liver. The main manifestation is splenomegaly, which may be accompanied by autoimmune thrombocytopenia, anemia, and hair cells seen in the peripheral blood. Laboratory tests must include testing for hepatitis C virus.
Pathologic diagnosis: The histology is similar to that of lymph node marginal zone lymphoma, and the immunophenotype is nonspecific. The diagnosis can be based on the presence of abnormal small lymphocytes in the bone marrow or peripheral blood with clinical manifestations of splenomegaly, after exclusion of FL, CLL/SLL, MCL, etc.
Treatment principles: Patients with asymptomatic, non-progressive hematocrit and no splenomegaly can be followed up. For patients with splenomegaly and positive hepatitis C virus, if there is no contraindication to treatment, anti-hepatitis C virus treatment can be given. Patients with splenomegaly and negative for hepatitis C virus may be followed up if they are asymptomatic; for patients with symptoms, rituximab monotherapy is preferred, and splenectomy is recommended for patients for whom rituximab therapy is not effective. For patients who progress after these treatments, refer to the treatment strategy for stage III/IV FL.
Prognosis: refer to the prognostic evaluation for FL. 4.
CLL/SLL are inert B-cell lymphomas, and CLL and SLL are different presentations of the same disease with the same treatment. The main difference between the two is that CLL presents with a large, abnormal number of lymphocytes in the peripheral blood, whereas in SLL the tumor load is mainly located in the lymph nodes. SLL is defined by the International Working Group on Chronic Lymphocytic Leukemia as having enlarged lymph nodes and/or splenomegaly, no hematocrit due to bone marrow invasion, and a peripheral blood clonal B-cell count <5×109/L. SLL requires histopathological confirmation by lymph node biopsy, whereas flow cytology is usually is sufficient to diagnose
Determination of CLL, with lymph node biopsy and bone marrow biopsy required when diagnosis is difficult. The diagnosis of CLL requires the following criteria: peripheral blood clonal B-cell count ≥5×109/L; clonal B-cell phenotype confirmed by flow cytometry; typical immunophenotype is CD19
(+), CD5(+), CD23(+), CD200(+), CD20(weak+), CD79b
(weak+), FMC-7 (-), CD10 (-), CyclinD1 (-). If the peripheral blood clonal B-cell count does not reach 5×109/L, but there is hematocrit due to bone marrow invasion, CLL is still diagnosed.
CLL/SLL accounts for approximately 7 percent of NHL in Europe and the United States
 to 10
to 10  , and is the most common type of adult leukemia. The incidence of CLL/SLL in Asia and China is low, accounting for about 1
, and is the most common type of adult leukemia. The incidence of CLL/SLL in Asia and China is low, accounting for about 1 to 3 of NHL src=”https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_202268.png” alt=””/>. The median age of onset is 65 years, and the male to female ratio is 1.5:1 to 2:1.
to 3 of NHL src=”https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_202268.png” alt=””/>. The median age of onset is 65 years, and the male to female ratio is 1.5:1 to 2:1.-
Clinical manifestations: The lesions usually involve peripheral blood, bone marrow, lymph nodes, and liver and spleen. The clinical manifestations are varied, with most patients being asymptomatic and some presenting with malaise, autoimmune anemia, infection, and hepatosplenomegaly and lymph node enlargement.
-
Pathologic diagnosis: typical CLL/SLL cells are monolithic, diffusely infiltrating with pseudofollicular formation (IHC phenotype: CD5(+), CD23(+), CD43
(+) or (-), CD10 (-), CD19 (+), CD20 (weakly +), LEF1 (+). When MCL needs to be identified, other markers such as Cyclin D1, SOX11 can be added. the presence of proliferative foci is easily misdiagnosed as reactive hyperplasia. All have monoclonal B-cell hyperplasia in the anterior phase.
Blood counts: persistently elevated white blood cells and lymphocytes, often >50 when classified as better differentiated CLL cells
and can reach 80
 to 90
to 90 , with a form similar to
Normal lymphocytes, but with irregularly shaped nuclei, deep cuts or nuclear fissures, irregularly aggregated nuclear chromatin, low cytosolic mass, and gray-blue color without granules. Ruptured cells (basket cells) are more common; a small number of naïve lymphocytes are seen, usually <
2
 . When peripheral blood naïve lymphocytes are >55
. When peripheral blood naïve lymphocytes are >55  , the diagnosis is B-CLL/juvenile lymphocytic leukemia. Thrombocytopenia is seen in advanced stages.
, the diagnosis is B-CLL/juvenile lymphocytic leukemia. Thrombocytopenia is seen in advanced stages.Bone marrow cytology: markedly active or extremely active proliferation of nucleated cells in the bone marrow. The lymphatic lineage is highly proliferative, with predominantly abnormal mature small lymphocytes accounting for 40

or more, even up to 90
 . The cells are basically the same size and morphology as the peripheral blood, with inconspicuous morphological abnormalities. The nuclei may have deep cuts or fissures, irregular aggregation of nuclear chromatin, no or inconspicuous nucleoli, a small amount of cytoplasm, and no granules. Some medium to large lymphocytes may also be interspersed. Primitive, naive lymphocytes are generally <5
. The cells are basically the same size and morphology as the peripheral blood, with inconspicuous morphological abnormalities. The nuclei may have deep cuts or fissures, irregular aggregation of nuclear chromatin, no or inconspicuous nucleoli, a small amount of cytoplasm, and no granules. Some medium to large lymphocytes may also be interspersed. Primitive, naive lymphocytes are generally <5  . Increased numbers of naïve lymphocytes correlate with disease progression. The triad of granulocytes, erythrocytes and megakaryocytes is significantly reduced. Nucleated erythrocytes may be significantly increased when the patient has concomitant hemolysis.
. Increased numbers of naïve lymphocytes correlate with disease progression. The triad of granulocytes, erythrocytes and megakaryocytes is significantly reduced. Nucleated erythrocytes may be significantly increased when the patient has concomitant hemolysis.-
Staging: SLL according to Ann-Arbor staging system, CLL according to Rai and Binet staging system (see Appendix 2.2).
- style=”margin-left: 72pt”>
- Treatment.
①SLL: Stage I patients are treated with local radiotherapy; Stage II-IV patients can be observed and followed up if no treatment is indicated, and the treatment principles of CLL are referred to when treatment is indicated.
②CLL: Low- and intermediate-risk patients in Rai 0-II can be followed up if no treatment is indicated; patients in Rai 0-II, patients with treatment indication, or patients in Rai III-IV with persistent hematocrit, according to del(17p) and/or TP53 mutation by FISH, immunoglobulin heavy chain mutable areas
(immunoglobulin heavy chain variable region, IGHV)
- Treatment.
Mutation status, patient’s general status and co-morbidities are factors that should be taken into account in selecting the appropriate treatment regimen. The treatment of supportive therapy for CLL, such as management of tumor lysis syndrome, infection, and autoimmune hemocytopenia, should be addressed.
③ Indications for treatment: suitability for clinical trials; significant disease-related symptoms, such as severe malaise, night sweats, weight loss, and noninfectious fever; threatening organ function; persistently enlarging large masses, such as splenomegaly more than 6 cm below the left costal margin and lymph nodes >10 cm in diameter; progressive anemia and progressive thrombocytopenia; failure of hormonal therapy. The patient’s condition is not a major one.
④ Choice of first-line treatment regimen.
-
No del(17p)/TP53 mutation: frail patients with severe concomitant disease (intolerant to purine analogs) or age ≥65 years and age <65 years with severe concomitant disease (creatinine clearance <Other recommended regimens include: bendamustine + CD20 monoclonal antibody (not recommended for frail patients), high-dose methylprednisolone + rituximab, azacitidine phenybutyrate, and rituximab.
Patients <65 years of age without severe co-morbidities, recommended regimens include: ibrutinib, bendamustine + CD20 monoclonal antibody, FCR (fludarabine, cyclophosphamide, rituximab) (preferable in patients with CLL with IGHV mutations), FR
(fludarabine, rituximab), high-dose methylprednisolone + rituximab, and ibrutinib + rituximab.
Maintenance therapy after first-line therapy: for high-risk patients (peripheral blood microscopic residual tumor cells ≥ 10-2 or IGHV non-mutant peripheral blood microscopic residual tumor cells ≥ 10-4 and <10-2) can be considered for lenalidomide maintenance therapy.
-
with del(17p)/TP53 mutation: Ibrutinib is the preferred recommendation. Other recommended regimens include: high-dose methylprednisolone + rituximab.
⑤ Treatment options for patients with relapsed drug resistance.
-
No del(17p)/TP53 mutation: frail patients with severe concomitant disease or age ≥65 years and age <65 Bruton's tyrosine kinase inhibitors (ibrutinib, zebutinib, obutinib) are recommended first for patients with severe concomitant disease (creatinine clearance <70 ml/mim), and veneclare
(venetoclax) + rituximab, other recommended regimens include: bendamustine + rituximab, reduced-dose FCR, high-dose methylprednisolone + rituximab, lenalidomide ± rituximab, venetoclax, increased-dose rituximab rituximab, bendamustine + rituximab + ibrutinib.
Patients <65 years of age without severe co-morbidities are first recommended for treatment with Bruton's tyrosine kinase inhibitors (ibrutinib, zebutinib, obutinib), and other recommended regimens include: bendamustine + rituximab, FCR, high-dose methylprednisolone + rituximab, lenalidomide ± rituximab, Vinecla, bendamustine + rituximab + ibrutinib.
Maintenance therapy after second-line therapy: Lenalidomide maintenance therapy may be considered for patients who have achieved CR or PR after second-line therapy.
-
with del(17p)/TP53 mutation: the preferred recommendation for second-line or higher treatment options: Bruton tyrosine kinase inhibitors ( Ibrutinib, Zebutinib, Obutinib), Vinecla + Rituximab, Vinecla; other recommended regimens include: high-dose methylprednisolone + Rituximab, Lenalidomide ± Rituximab.
- style=”margin-left: 83pt”>
- Prognosis: Adverse prognostic factors include: IGHV without mutation, del(17p)
/TP53 mutation, del (11q), complex karyotype (≥3 chromosomal abnormalities); flow cytometry detection of tumor cells positive for CD38 ≥30
 , ZAP-70 positive ≥20
, ZAP-70 positive ≥20 , CD49d positive ≥30
, CD49d positive ≥30 . Elevated β2 microglobulin and late staging, etc.
. Elevated β2 microglobulin and late staging, etc.MCL accounts for approximately 3
 to 10 percent of the NHL. 10
to 10 percent of the NHL. 10  , with a male-to-female ratio of 2:1 to 3:1 and a median age of onset of about 65 years. The natural course can be aggressive or inert, but most have aggressive growth characteristics. The response to treatment is similar to that of inert lymphoma and is not curable with conventional chemotherapy. The survival period of previous multidrug combination chemotherapy is about 3-5 years, but it has been significantly extended in recent years with the introduction of HDT/ASCT, cytarabine and targeted drugs. A small proportion of inert MCL, called leukemia-like non-lymphoid MCL, has a lesser molecular genetic variation, no del(17p)/TP53 mutations, and no or low expression of SOX11, with a course similar to inert lymphoma and a better prognosis.
, with a male-to-female ratio of 2:1 to 3:1 and a median age of onset of about 65 years. The natural course can be aggressive or inert, but most have aggressive growth characteristics. The response to treatment is similar to that of inert lymphoma and is not curable with conventional chemotherapy. The survival period of previous multidrug combination chemotherapy is about 3-5 years, but it has been significantly extended in recent years with the introduction of HDT/ASCT, cytarabine and targeted drugs. A small proportion of inert MCL, called leukemia-like non-lymphoid MCL, has a lesser molecular genetic variation, no del(17p)/TP53 mutations, and no or low expression of SOX11, with a course similar to inert lymphoma and a better prognosis.(1) Clinical features: Most often involves lymph nodes, bone marrow, gastrointestinal tract, spleen, and pharyngeal lymphatic rings, and at diagnosis 70
 for stage IV. Bone marrow invasion rate can be 50
for stage IV. Bone marrow invasion rate can be 50 to
to100
 , with a high rate of invasion of the lower gastrointestinal tract, often presenting endoscopically as multiple polypoid lesions.
, with a high rate of invasion of the lower gastrointestinal tract, often presenting endoscopically as multiple polypoid lesions.-
Pathologic diagnosis: The tumor cells of MCL are small to medium to large lymphocytes with a consistent morphology and a slightly irregular nuclear surface. The tumor cells in MCL are small to medium to large lymphocytes with uniform morphology, slightly irregular nuclei, and diverse growth patterns, including nodular, nodular and diffuse. IHC marker selection includes CD20, PAX5, CD3, Cyclin D1, CD10, CD23, and CD24.
MUM-1, CyclinD1, SOX11, and CD138. The typical immunophenotype is CD19
(+), CD5(+), CD23(-), CD200(weak+), CD20(+), CD79b
(+), FMC-7 (+), CD10 (-), CyclinD1 (+). Most patients have CD5(+), Cyclin D1(+) expression, and in the case of Cyclin D1(-), FISH for CCND2 and CCND3 and IHC for SOX11 can be added for a comprehensive diagnosis. Confirmation of the diagnosis is difficult and additional evidence needs to be sought, and the FISH test t(11;14) is highly sensitive and specific for the diagnosis of MCL. In addition, the 2017 WHO Classification of Hematopoietic and Lymphoid Tissue Neoplasms classifies MCL into two types: classical MCL, which presents with SOX11 positivity and no mutation in IGHV, and is clinically aggressive with a poor prognosis, and can also present with more aggressive variant maternal cell and polymorphic phenotypes, often with TP53 mutations; and leukemic extranodal MCL, which often involves peripheral blood, bone marrow and spleen, and presents with SOX11. The other is leukemic extranodal MCL, often involving peripheral blood, bone marrow, and spleen, which is SOX11-negative with IGHV mutations, clinically inert, and has a better prognosis.
Bone marrow cytology: When the tumor cells involve the bone marrow, a variable number of abnormal lymphocytes are seen in the bone marrow smear, with varying cell sizes and round or mildly irregular nuclei, mostly with a large, malformed nucleolus. The cytoplasm is abundant and pale blue in color.
-
Treatment: Patients with MCL should be examined thoroughly and staged accurately to guide the choice of treatment. For patients with maternal cell transformation or CNS symptoms, cerebrospinal fluid and brain MRI should be performed, and for patients with a proposed stage I or II diagnosis, endoscopy should be performed to exclude gastrointestinal invasion.
1) Treatment strategy: Stage I or limited Stage II without large masses is recommended for either ISRT alone or conventional dose-intensity immunochemotherapy ± ISRT.
For extensive stage II without a large mass, conventional-dose intensity immunochemotherapy is recommended. Some patients with inert clinical features, such as leukemia-like non-lymphoid MCL with splenomegaly, SOX11-negative [IGHV mutant], no TP53 mutation or deletion, and low tumor load, Ki-67 proliferation index <10
 , etc., can be observed for follow-up.
, etc., can be observed for follow-up.Patients with stage II with large masses and stage III/IV with aggressive clinical features are recommended for sequential HDT/ASCT after high-dose intensity induction chemotherapy if HDT/ASCT is appropriate; patients who are not suitable for HDT/ASCT are recommended to participate in clinical trials or conventional dose intensity. Patients with inert features who are asymptomatic or have no indication for treatment may be observed for follow-up. Those with symptoms or indications for treatment need to be selected accordingly based on the presence or absence of TP53 mutations.
First-line regimens: high-dose intensity regimens: R-DHA (rituximab, dexamethasone, cytarabine) + platinum (carboplatin, cisplatin, or oxaliplatin), alternating R-CHOP/R-DHAP, NORDIC (intensified dose of R-CHOP [maxi-CHOP] alternating with rituximab + high-dose cytarabine) regimen, HyperCVAD, rituximab, bendamustine sequential rituximab and high-dose cytarabine; other recommended regimens: bendamustine + rituximab.
Conventional dose-intensity regimens: recommended bendamustine + rituximab, VR-CAP (bortezomib, rituximab, cyclophosphamide, adriamycin, and prednisone), R-CHOP, lenalidomide + rituximab; other recommended regimens. Modified R-HyperCVAD regimen (for patients <60 years of age), RBAC500 (rituximab, bendamustine, adriamycin).
Consolidation therapy: HDT/ASCT can be considered.
Maintenance therapy: rituximab.
③ Second-line regimens: regimens or drugs not used in first-line regimens may be chosen. Recommended preferred regimens include: BTK inhibitors (ibrutinib, zebutinib, obrutinib); lenalidomide + rituximab; other recommended regimens include: bendamustine + rituximab, bendamustine + rituximab + cytarabine, bortezomib ± rituximab; R-DHAP, R-DHAX (dexamethasone, cytarabine, oxaliplatin), R-GemOx , BTK inhibitor + lenalidomide + rituximab, BTK inhibitor + vinecla, vinecla ± rituximab, etc.
Consolidation therapy after second-line therapy: allogeneic hematopoietic stem cell transplantation.
-
Prognosis: IPI is derived from survival data in aggressive lymphoma and can also be used as a prognostic indicator for MCL, but the prognostic efficacy is poor. The international prognostic index for mantle cell lymphoma (MIPI) is widely used as a good prognostic stratification for MCL. Other poor prognostic factors include Ki-67, TP53 mutation, and maternal cell transformation. Of these, Ki-67 >30
 is the most important biological prognostic indicator independent of MIPI. The International Prognostic Index of Set Cells combined with Ki-67
is the most important biological prognostic indicator independent of MIPI. The International Prognostic Index of Set Cells combined with Ki-67(combined mantle cell lymphoma international prognostic index (MIPIc)), which better distinguishes prognosis, is also recommended (see Appendix 4.4). The efficacy of conventional regimens and treatments such as HDT/ASCT in patients with TP53 mutations is poor, and TP53 mutations with Ki-67 >30
 and maternal cell-like cell morphology.
and maternal cell-like cell morphology.Burkitt’s lymphoma is a highly aggressive form of NHL that can be classified as endemic, endemic, and endemic.
Sporadic and immunodeficiency-associated variants. Burkitt’s lymphoma accounts for approximately 3
 to 5
to 5  and accounts for about 40 percent of childhood NHL
and accounts for about 40 percent of childhood NHL .
.- style=”margin-left: 83pt”>
- Clinical features: Epidemic Burkitt’s lymphoma occurs mainly in Africa
Equatorial region and northeastern Brazil, with peak age of onset between 4 and 7 years, male to female ratio of 2:1, mostly involving the jaws, and EBV positivity rate >95
 . Sporadic Burkitt’s lymphoma is scattered throughout the world, mainly in children and young adults, with a male to female ratio of 2:1 to 3:1. Abdominal involvement is common, with an EBV positivity rate of <30
. Sporadic Burkitt’s lymphoma is scattered throughout the world, mainly in children and young adults, with a male to female ratio of 2:1 to 3:1. Abdominal involvement is common, with an EBV positivity rate of <30 . The immunodeficiency-associated type occurs mostly in patients with AIDS and often involves lymph nodes and bone marrow. Burkitt’s lymphoma is the tumor with the shortest cell multiplication cycle and grows rapidly. Extra-nodal invasion of Burkitt’s lymphoma is common, with the head and neck, abdomen, bone marrow, and central nervous system being the most frequently involved sites.
. The immunodeficiency-associated type occurs mostly in patients with AIDS and often involves lymph nodes and bone marrow. Burkitt’s lymphoma is the tumor with the shortest cell multiplication cycle and grows rapidly. Extra-nodal invasion of Burkitt’s lymphoma is common, with the head and neck, abdomen, bone marrow, and central nervous system being the most frequently involved sites.-
Pathologic diagnosis: Classic Burkitt’s lymphoma morphology shows diffuse proliferation of moderately large tumorigenic B cells in a homogeneous pattern, with marked nuclear schizophrenia and apoptosis. The apoptosis is obvious, and starry sky phenomenon is common. The tumor cells originate from the germinal center, and the IHC immunophenotype often shows sIgM(+), single light chain(+), CD19(+), CD20
(+), CD22 (+), c-Myc (+), CD10 (+), Bcl6 (+), Bcl2
(- or weakly +), CD5 (-), CD23 (-), MUM-1 (-), and TdT (-). The proliferation index was very high, with Ki-67 nearly 100
 . Even though the morphology and immunophenotype were typical of Burkitt’s lymphoma, FISH MYC testing was performed, where t
. Even though the morphology and immunophenotype were typical of Burkitt’s lymphoma, FISH MYC testing was performed, where t(8;14) accounted for about 80
, t(2;8) and t(8;22) accounted for 15
 . The differential diagnosis includes morphology, immunophenotype are typical of Burkitt’s lymphoma, but those without MYC abnormalities are classified as high-grade B-cell lymphoma, non-specific. EBER testing is mandatory for Burkitt’s lymphoma, but more sporadic patients in our country, EBER
. The differential diagnosis includes morphology, immunophenotype are typical of Burkitt’s lymphoma, but those without MYC abnormalities are classified as high-grade B-cell lymphoma, non-specific. EBER testing is mandatory for Burkitt’s lymphoma, but more sporadic patients in our country, EBER
(-) is more common.
Bone marrow cytology: markedly active or extremely active bone marrow proliferation. The typical Burkitt’s lymphoma cells are medium to large lymphocytes of varying size and easily distributed in piles; the nuclei of leukemic cells are large, mostly round or irregular, with coarse granular nuclear chromatin and one to several distinct nucleoli of varying size; the cytosolic mass is variable, strongly basophilic and contains lipid vacuoles of varying size and number in a chisel-like pattern, and vacuoles are also seen in the nuclei. The smear showed many degenerated cells, and the proliferation of granulocytes and erythrocytes was inhibited.
-
Treatment: chemotherapy is the mainstay, but the CHOP regimen is not effective, and high-dose intensive therapy and combination with rituximab may improve the outcome. The central nervous system should be treated prophylactically and tumor lysis syndrome should be adequately prevented. The chemotherapy options for Burkitt’s lymphoma include CODOX-M + rituximab, CODOX-M/IVAC regimen, DA-EPOCH-R or R-HyperCVAD/HD-MA regimens.
protocols, etc. For low-risk patients with low tumor load, 3 cycles of treatment to CR followed by one cycle of consolidation therapy can end the treatment. In patients with existing brain parenchymal invasion at diagnosis, the first cycle of therapy should begin with a regimen that includes drugs that can cross the blood-brain barrier. The DA-EPOCH-R regimen should be chosen in combination with intrathecal MTX, which is not appropriate for patients with parenchymal invasion.
There is no clearly recommendable second-line rescue regimen; consider R-ICE, R-GDP, R-IVAC, high-dose cytarabine + rituximab, and HDT/ASCT or allogeneic hematopoietic stem cell transplantation for patients who achieve CR after rescue therapy.
- style=”margin-left: 73pt”>
- Prognosis: age >40 years, poor general condition, late staging, LDH
- Prognosis: age >40 years, poor general condition, late staging, LDH
increased, bone marrow and CNS invasion, and human immunodeficiency virus positivity have a poor prognosis.
lymphoblastic lymphoma (LBL) accounts for 3 percent of adult NHL
 ~4% of NHL in adults and about 40% of NHL in children. It is a highly aggressive lymphoma. It can be divided into T-cell-derived (T-LBL) and B-cell-derived (B-LBL), with T-LBL accounting for 80% of LBL
~4% of NHL in adults and about 40% of NHL in children. It is a highly aggressive lymphoma. It can be divided into T-cell-derived (T-LBL) and B-cell-derived (B-LBL), with T-LBL accounting for 80% of LBLand above, B-LBL accounts for about 80% of LBL
10
 ~15
~15 . LBL is associated with acute LBL and acute lymphocyte leukemia (ALL) are the same disease with different clinical manifestations and different stages of development, and the 2017 edition of WHO Hematopoietic and Lymphoid Tissue Neoplasms defines the ratio of primitive and naive lymphocytes in the bone marrow as ≥20
. LBL is associated with acute LBL and acute lymphocyte leukemia (ALL) are the same disease with different clinical manifestations and different stages of development, and the 2017 edition of WHO Hematopoietic and Lymphoid Tissue Neoplasms defines the ratio of primitive and naive lymphocytes in the bone marrow as ≥20  Defined as ALL.
Defined as ALL.-
Clinical manifestations: The typical clinical manifestations of T-LBL are cough and shortness of breath due to a large anterior mediastinal mass, which may be accompanied by pleural effusion, and bone marrow and central nervous system invasion. B-LBL often presents with enlarged lymph nodes, and skin or bone invasion is common.
-
Pathologic diagnosis: In terms of cell morphology, LBL mainly presents with diffuse growth of medium-sized tumor cells with round, non-circular nuclei. The immunophenotype of LBL is characterized by TdT(+), but CD99, CD34, CD10 can also be added to assist in the determination of maternal cell differentiation. The immunophenotype of B-LBL is sIg(-), cIg
(+), CD10(+), CD19(+), CD20(-) or (+), CD79(+), PAX5(+); the immunophenotype of T-LBL is CD3ε(+) or (-), CD2(+), CD4(+), CD8 (CD7, CD43, CD4 (+), CD4 (+), CD8 (+), CD1a (+) or (-), and CD7 (+).
Cannot be used as a marker for T lymphocytes alone. When cells are naive, additional assays for CD34, CD117, MPO, and Lys are required to identify AML. Because LBL originates from immature stage lymphocytes, it is not uncommon and particularly important to note that tumor cells may express markers of B or T lymphocytes, or even molecular markers of NK or myeloid cells. B-LBL is often associated with specific genetic abnormalities, such as BCR-ABL1, ETV6-RUNX1, and KMT2A rearrangements, and molecular genetic testing is recommended when available. The following is a list of the genes that are associated with specific genetic abnormalities
Bone marrow cytology: The bone marrow nucleated cell proliferation is mostly extremely active or markedly active, with predominantly primitive and naive lymphocytes, often with abnormal morphology; primitive lymphocytes are round, oval, or caudate in shape; nuclei are mostly round, with large nuclei and unevenly coarse and fine nuclear chromatin. The nuclei were mostly round, oval or with caudate protrusions. The nuclei were mostly round, with a large nucleus, a thick and thin nuclear chromatin, and a regular arrangement. Granulocyte proliferation was significantly inhibited, and granulocytes were significantly reduced or even absent. Erythrocyte proliferation was also significantly suppressed, and young red blood cells were rare or absent. The majority of megakaryocytes were significantly reduced or absent, and platelets were rare. Degenerated cells are significantly increased. Nuclear schwannoma cells are easily seen. In T acute lymphoblastic lymphoma, eosinophilic infiltration around the lymphoma cells was found, requiring exclusion of eosinophilia and myeloid hyperplasia with 8p11.2 cytogenetic abnormalities of the FGFR1 gene.
Blood count: leukocytes are mostly elevated, a few up to 100×109/L.
- style=”margin-left: 83pt”>
- Therapeutic principles and treatment options: Whether the patient is in stage I or stage IV, the
-
Prognosis: The prognosis for children with LBL is significantly better than that for adults. Other poor prognostic factors include high leukocytes, CNS involvement, long time to reach CR, and residual lesions at the end of induction chemotherapy. Genetic abnormalities associated with poor prognosis include: subdiploidy (<44 chromosomes), t (9;22)
(q34;q11.2):BCR-ABL1, BCR-ABL1-like (Ph-like), KMT2A heavy
row (t[4;11]), t(v;14q32)/IgH, t(17;19):TCF3-HLF fusion, complex karyotype (≥5 chromosomal abnormalities), IKZF1 gene variant, intrachromosomal amplification of chromosome 21 (intrachromosomal amplification of chromosome 21 (iAMP21). t(12;21)(p13;q22):ETV6-RUNX1
and polyploidy (patients with chromosome 4, 10 and 17 triploidy showed a better prognosis) were associated with a good prognosis.
Peripheral T-cell lymphoma (PTCL) is a group of malignant neoplasms of the lymphatic system originating from mature T lymphocytes in the posterior thymus. Peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS) accounts for 7 of all NHLs in Europe and the United States
 ~10
~10 , the incidence is significantly higher in Asian countries than in Europe and the US, accounting for 15
, the incidence is significantly higher in Asian countries than in Europe and the US, accounting for 15 ~22
~22  . Because it is not specific in morphology, immunology, genetics, or clinical presentation, the diagnosis of PTCL-NOS can be made only after excluding other independently staged T-cell lymphomas.
. Because it is not specific in morphology, immunology, genetics, or clinical presentation, the diagnosis of PTCL-NOS can be made only after excluding other independently staged T-cell lymphomas.- Clinical presentation: PTCL-NOS is common in middle-aged and older adults, with a median age of 55 years and no significant gender differences in PTCL-NOS. PTCL-NOS does not differ significantly by gender. It mostly presents as superficial lymph node enlargement, and half of them are associated with B symptoms. The nodes often involve skin and subcutaneous tissues, liver and spleen, gastrointestinal tract, thyroid and bone marrow. It is mostly stage III or IV at diagnosis.
-
Pathologic diagnosis: PTCL-NOS is a tumor of the mature (peripheral) T-cell developmental stage. The pathological histology is a mixed background of abundant hyperendothelial small vessel proliferation, epithelioid histiocyte proliferation and inflammatory cell infiltration. The tumor cells are morphologically diverse and variable, and can consist of small, medium, or large cells, mostly medium to large, with lightly stained cytoplasm, pleomorphic, irregular nuclei, multiple chromatin or vesicles, pronounced nucleoli, and frequent nuclear schizophrenia; common immunophenotypes are CD3(+), CD4
(+) > CD8(+), CD5(+), CD45RO(+), CD7(-), CD8(-). Tumor cells often express T cell-associated antigens such as CD3ε and CD2, and the loss of a
one or more other mature T-cell antigens (CD5 or CD7), suggesting clonal proliferation of T cells; meanwhile, the TCR gene of PTCL-NOS often shows clonal rearrangement, and when it is associated with altered lymphoid tissue reactivity, the TCR gene is often clonally rearranged. When it is difficult to differentiate from lymphoid tissue reactive changes, TCR gene rearrangement assay can be used to assist in the diagnosis. It is also important to identify lymphomas of follicular helper T-cell origin, such as angioimmunoblastoma T-cell lymphoma, lymph node peripheral T-cell lymphoma with follicular helper T-cell phenotype, and lymph node follicular helper T-cell lymphoma. In addition, when cellular pleomorphism is evident in DLBCL, which resembles T-cell features, differentiation is also required, so B-cell markers (such as CD20 and PAX5) are indispensable. In the presence of multiple plasma cell proliferations, note the clonality of plasma cells.
Bone marrow cytology: bone marrow nucleated cell proliferation is mostly markedly active, with lymphocytic proliferation predominating and adult-type T-cell leukemia cells often >10
 , which can be as high as
, which can be as high as80
 and above. Granulocytes, young red blood cells, and megakaryocytes are often reduced.
and above. Granulocytes, young red blood cells, and megakaryocytes are often reduced.- style=”margin-left: 83pt”>
- Treatment.
① Treatment principles: PTCL-NOS itself is a heterogeneous group of diseases, and its optimal treatment protocols and therapeutic strategies are still being explored. Patients with stage I-IV disease are first recommended to participate in appropriate clinical trials or 4-6 cycles of chemotherapy ± ISRT, and those who achieve CR after treatment may be considered for appropriate clinical trials, HDT/ASCT, or discontinuation of therapy for observation. Patients with relapsed refractory PTCL-NOS are also first recommended for clinical trials or second-line regimens and palliative radiotherapy; HDT/ASCT or allogeneic hematopoietic stem cell transplantation may be considered for patients who achieve CR on second-line therapy.
② First-line regimens: CHOP, CHOEP, DA-EPOCH recommended first; other regimens include: CHOP sequential IVE (isocyclophosphamide, etoposide, epi-EPOCH), and CHOP sequential IVE.
Adriamycin), hyperCVAD/MA.
③ Second-line regimens: priority for clinical trials. Preferred recommended regimens include: cidabendiamide, vibutuximab (for CD30 positive), DHAP, DHAX, ESHAP, GDP, GemOX, ICE, etc. Other recommended regimens include: bendamustine, gemcitabine, lenalidomide, or GVD (gemcitabine, vincristine, liposomal adriamycin).
-
Prognosis: The overall prognosis for PTCL-NOS is worse than for patients with aggressive B-cell lymphoma, with a 5-year Survival rate is about 30

. The prognostic scoring system includes the IPI and the PTCL-NOS prognostic index for peripheral T-cell lymphoma (not otherwise specified, PIT), which includes age >60 years, elevated LDH, ECOG PS score ≥2, and bone marrow invasion.(Appendix 4.5).
Mycosis fungoides/sézary syndrome (MF/SS) is the most common cutaneous T cell lymphoma (CTCL). lymphoma (CTCL), accounting for 2
 to 3 of NHL. “https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_2022109.png” alt=””/>. MF accounts for 60% of CTCL
to 3 of NHL. “https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_2022109.png” alt=””/>. MF accounts for 60% of CTCL  , SS accounts for only 5
, SS accounts for only 5 . MF is an inert course of primary cutaneous, mature T-cell lymphoma, and patients tend to present with intermittent, stable, or slowly developing lesions. Involvement of extracutaneous tissues, primarily lymph nodes and peripheral blood, suggests advanced disease. SS is a variant of MF that presents as an aggressive erythrodermic leukemia
. MF is an inert course of primary cutaneous, mature T-cell lymphoma, and patients tend to present with intermittent, stable, or slowly developing lesions. Involvement of extracutaneous tissues, primarily lymph nodes and peripheral blood, suggests advanced disease. SS is a variant of MF that presents as an aggressive erythrodermic leukemia -
Clinical features: MF clinically presents with multiple cutaneous erythema, plaques, and verrucous nodules. It can occur all over the skin and is often associated with marked pruritus. The disease course is inverse
Recurrent progression, with lesions confined to the skin for months, years, or even decades, can occur in the advanced stages of the disease. Lymph node and visceral invasion may occur in advanced stages of the disease. Approximately 10
 of lesions present as generalized erythrodermatosis. SS presents as generalized erythrodermatosis with peripheral blood (abnormal cells in the circulating blood as a percentage of lymphocytes >5
of lesions present as generalized erythrodermatosis. SS presents as generalized erythrodermatosis with peripheral blood (abnormal cells in the circulating blood as a percentage of lymphocytes >5 ), and in the lesion tissue, lymph nodes Sezary cells can be seen in lesion tissue, lymph nodes and peripheral blood. The diagnosis of SS should meet the following criteria: absolute Sezary cell value ≥1×109/L, CD4+/CD8+ cell ratio ≥10, tumor cell immunophenotype of CD3(+), CD4(+), CD5(+), CD45RO
), and in the lesion tissue, lymph nodes Sezary cells can be seen in lesion tissue, lymph nodes and peripheral blood. The diagnosis of SS should meet the following criteria: absolute Sezary cell value ≥1×109/L, CD4+/CD8+ cell ratio ≥10, tumor cell immunophenotype of CD3(+), CD4(+), CD5(+), CD45RO(+), CD7(-), CD8(-) and evidence of clonal proliferation of T cells.
-
Pathologic diagnosis: The diagnosis of MF is difficult and may require several years of observation and multiple biopsies to confirm the diagnosis. Small, polymorphonuclear lymphocytes accumulate at the epidermal or epidermal-dermal junction, infiltrating toward the epidermis and forming Pautrier microabscesses are characteristic. the most prominent features of SS are similar to those of MF. the MF immunophenotype is usually that of mature helper T cells, with CD3ε(+), CD4(+), CD45RO
(+), CD8 (-). A mature T-cell phenotype of CD4(-), CD8(+) is occasionally seen, and evidence of clonal proliferation of T cells exists. The disease needs to be differentiated from follicular adjuvant T-cell-derived lymphoma.The pathologic diagnosis of the nonmass stage of MF is difficult and requires attention to differentiation from nonspecific dermatitis, which must be closely integrated clinically.
- style=”margin-left: 72pt”>
- Staging: See Staging Criteria for Cutaneous T-Cell Lymphoma (Appendix 1.3).
- Staging: See Staging Criteria for Cutaneous T-Cell Lymphoma (Appendix 1.3).
- Treatment principles: There is no curative treatment for MF and SS, and appropriate treatment is chosen based on the stage. The main goal of treatment is to control the extent of lesions, reduce symptoms and reduce the risk of progression. In most cases, treatment does not provide lasting relief. Treatment of primary lesions should be based on low toxicity and low cumulative toxicity to achieve durable or maintenance therapy. When chemotherapy is required, the first choice is recommended
Monotherapy, as combination therapy also does not significantly prolong remission. The relationship between efficacy and prognosis is unclear, and changes in clinical symptoms and signs can be used as a basis for determining efficacy. When the lesion progresses again after a period of discontinuation of treatment, resumption of the previous treatment or medication may continue to be effective. Prevention and control of skin infections and relief of pruritus are also important aspects of treatment.
Early stage lesions should not be treated aggressively, with a single or combination of topical treatments; stages IIB, III, IV, and refractory lesions may be treated with a combination of systemic systemic treatments or in appropriate clinical trials. Treatments for skin lesions include radiotherapy, phototherapy, and topical corticosteroids, azelaic acid ointment, or retinoic acid. Systemic drug therapy is recommended with vibutuximab, interferon, methotrexate (≤50 mg/week), gemcitabine, liposomal adriamycin, and vincristine.
-
Prognosis: Patients with MF have a good prognosis with a 5-year survival rate of nearly 90%. The prognosis for SS patients is usually poor, with a median survival of approximately 2 to 4 years.
The most common type of NK/T-cell lymphoma is extranodal NK/T-cell lymphoma, nasal type. It usually occurs in the upper respiratory tract, including the nasal cavity, nasopharynx, paranasal sinuses, tonsils, hypopharynx, and larynx; it can also involve the extra-nasal region, with the skin, testes, and gastrointestinal tract being the most common sites of extra-nasal involvement. This type of lymphoma is more common in Asia than in Europe and the United States, and is the most common type of peripheral T-cell lymphoma in China, accounting for 40% of all peripheral T-cell lymphomas
 ~50
~50  .
.
-
Clinical features: common in young males, B symptoms are common, and tumors are often confined to the nasal cavity or Invasion of adjacent tissues. Early lesions account for 70
 to 90
to 90 . Common signs and symptoms are nasal congestion or rhinorrhea and enlarged lymph nodes in the neck.
. Common signs and symptoms are nasal congestion or rhinorrhea and enlarged lymph nodes in the neck. -
Pathologic diagnosis: extranodal NK/T-cell lymphoma, nasal type pathology characterized by diffuse lymphoma cell infiltration with angiocentric, vascular destructive growth, resulting in tissue ischemic necrosis and mucosal ulceration. Necrosis is common and is a major cause of missed diagnoses. IHC markers required for diagnosis include CD3, CD56, CD2, CD4, CD5, CD7, CD8, CD45RO, CD20, PAX5, TIA-1, granules
Enzyme B, Ki-67, and EBER, among others. The typical immunophenotypes are CD2(+), CD3
(+), CD56(+), TIA-1(+), granzyme B(+), and EBER(+). Diagnosis is cautious with EBER (-), diagnostic if CD56 (+), CD3 (+), and cytotoxic T cell markers are expressed, and diagnostic of PTCL-NOS if CD3 (-), CD56 (-).60
 ~90
~90  of extranodal NK/T-cell lymphomas do not have TCR gene rearrangements. This disease needs to be differentiated from undifferentiated carcinoma, and epithelial markers such as CK and EMA testing should be added.
of extranodal NK/T-cell lymphomas do not have TCR gene rearrangements. This disease needs to be differentiated from undifferentiated carcinoma, and epithelial markers such as CK and EMA testing should be added.Bone marrow cytology: tumor cells are round or oval with pseudopod-like protrusions; nuclei are mostly round with finely granular chromatin and multiple but inconspicuous nucleoli; cytoplasm is medium and dark blue with vacuoles. When the thorax is involved, tumor cells are visible in the pleural water.
- style=”margin-left: 72pt”>
- Treatment.
① Treatment principle: A distinction needs to be made between patients with primary nasal or upper respiratory tract and those with primary extra-nasal origin. Because of sensitivity to radiotherapy, early stage patients should be treated with a combined chemoradiotherapy strategy. Stage I/II (primary nasal type): Patients who are not suitable for chemotherapy are recommended
- Treatment.
Radiotherapy alone or participation in an appropriate clinical trial; for patients suitable for chemotherapy, participation in an appropriate clinical trial or combination chemoradiotherapy with 2 to 4 chemotherapy cycles is recommended. Stage IV (primary nasal type) or stages I-IV (primary extra-nasal) are recommended to participate in an appropriate clinical trial or a combination regimen of chemotherapy±radiotherapy with menadase as the primary.
② First-line chemotherapy regimens: P-GemOx (gemcitabine, peginterferonase, oxaliplatin), DDGP (dexamethasone, cisplatin, gemcitabine, peginterferonase), SMILE (dexamethasone, methotrexate, isocyclophosphamide, peginterferonase (dexamethasone, methotrexate, isocyclophosphamide, peginterferonase, etoposide).
Recommended regimens for synchronized chemoradiotherapy: DeVIC (dexamethasone, etoposide, isocyclophosphamide, carboplatin), VIPD (etoposide, isocyclophosphamide, cisplatin, dexamethasone).
③ Second-line regimens: DAHP, DHAX, ESHAP, GDP, GemOx, ICE, cidabendiamide, etc.
-
Prognostic factors: The common prognostic model used internationally is the Prognostic Index of Natural Killer Lymphoma (Prognostic Index). Prognostic Index of Natural Killer Lymphoma (PINK) and Prognostic Index of Natural Killer Lymphoma with Epstein-Barr Virus DNA (PINK-E). Poor prognostic factors for the PINK model included age >60 years, distant lymph node invasion, stage III/IV, extra-nasal primary, and PINK-E if the presence or absence of detectable EBV-DNA in plasma was included. See Annex 4.6.
Note: This guideline was developed based on clinical research evidence and expert consensus
. The recommended treatment regimens are based on drugs with approved indications in China, while advances in domestic and international research are presented. In deciding on a patient’s treatment plan, each patient should be given a standardized and individualized treatment based on the characteristics and clinical presentation of the disease.
Annex 1. World Health Organization Classification of Tumours of Haematopoietic and Lymphoid Tissues Lymphoma section
 (Revision 2017)
(Revision 2017)Lymphoma Type


Prominent lymphoid neoplasm
- style=”margin-left: 62pt”>
- B lymphoblastic leukemia/lymphoma, non-specific
-
B lymphoblastic leukemia/lymphoma with frequent genetic abnormalities
B lymphoblastic leukemia/lymphoma with t(9;22) (q34.1;q11.2); BCR-ABL1 B lymphoblastic leukemia/lymphoma with t(v; 11q23.3); KMT2A rearrangement
B lymphoblastic leukemia/lymphoma with t(12;21) (p13.2;q22.1); ETV6-RUNX1
B lymphoblastic leukemia/lymphoma with hyperdiploidy B lymphoblastic leukemia/lymphoma with hypodiploidy
B lymphoblastic leukemia/lymphoma with t(5;14)(q31.1;q32.3); IL3-IGH B lympho lymphoblastic leukemia/lymphoma with t(1;19) (q23;p13.3); TCF3-PBX1 B lymphoblastic leukemia/lymphoma, BCR-ABL1-like
B lymphoblastic leukemia/lymphoma with iAMP21
-
T lymphoblastic leukemia/lymphoma
Early T prolymphocytic leukemia
- NK lymphoblastic leukemia/lymphoma a
Mature B-cell lymphoma
- style=”margin-left: 62pt”>
- Chronic lymphocytic leukemia/small lymphocytic lymphoma
- Monoclonal B lymphocytosis
- B-cell juvenile lymphocytic leukemia
- Lymphoma of the splenic marginal zone
-
Hairy cell leukemia
- Spleen B-cell lymphoma/leukemia, unclassified a a span>Spleen diffuse erythroid small B-cell lymphoma a Hairy cell leukemia – variant a
- Spleen B-cell lymphoma/leukemia, unclassified a a span>Spleen diffuse erythroid small B-cell lymphoma a Hairy cell leukemia – variant a
 Lymphoplasmacytic lymphoma
Lymphoplasmacytic lymphoma


Waldentrom’s Macroglobulinemia
- style=”margin-left: 80pt”>
-
Monoclonal gammopathy of undetermined significance, IgM-type mu heavy chain disease
ɑ heavy chain disease gamma heavy chain disease
- style=”margin-left: 62pt”>
-
Plasma cell tumors
Monoclonal gammopathy of undetermined significance, non-IgM plasma cell myeloma
Isolated plasmacytoma of bone extracellular plasmacytoma of bone
Monoclonal immunoglobulin deposition disease Primary amyloidosis Light and heavy chain deposition disease
- Lymphoma of the extra-nodal marginal zone of mucosa-associated lymphoid tissue
-
Lymphoma of the marginal zone of lymph nodes
Lymphoma of the marginal zone within the nodes in children a
-
Follicular lymphoma
In situ follicular neoplasm
Duodenal follicular lymphoma Testicular follicular lymphoma
- Childhood type follicular lymphoma
- Large B-cell lymphoma with IRF4 rearrangementa
- Follicular center lymphoma of primary skin
-
Sleeve cell lymphoma
In situ condyloma
-
Diffuse large B-cell lymphoma, non-specific germinal center B-cell subtype a
Activated B-cell subtype
-
- Large B-cell lymphoma enriched in T-cells/histiocytes


- style=”margin-left: 62pt”>
- Diffuse large B-cell lymphoma of the central nervous system in the primary
- Primary diffuse large B-cell lymphoma of the skin, leg type
- EBV-positive diffuse large B-cell lymphoma, non-specific
-
EBV-positive mucocutaneous ulcers
- Chronic inflammation-associated diffuse large B-cell lymphomaFibrin-associated diffuse large B-cell lymphoma
- Chronic inflammation-associated diffuse large B-cell lymphomaFibrin-associated diffuse large B-cell lymphoma
- Lymphomatoid granulomatosis, grade 1/2
- Lymphomatoid granulomatosis, grade 3
- Primary mediastinal (thymic) large B-cell lymphoma
- Intravascular large B-cell lymphoma
- ALK-positive large B-cell lymphoma
- Plasmacytoid lymphoma
- Primary exudative lymphoma
-
HHV8-related lymphoproliferative disorders
Multicentric Castleman disease
HHV8-positive diffuse large B-cell lymphoma, non-specific HHV8-positive pro-liferative lymphoproliferative disease
- Burkitt’s lymphoma
- Burkitt-like lymphoma with 11q abnormalities a
-
High-grade B-cell lymphoma
High-grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements, non-specific
- Unclassifiable B-cell lymphoma between diffuse large B-cell lymphoma and classic Hodgkin’s lymphoma
Mature T/NK cell lymphoma
- style=”margin-left: 62pt”>
- T-cell juvenile lymphocytic leukemia
- T-cell Large Granular Lymphocytic Leukemia
- Chronic NK-cell lymphoproliferative disorders a
- Aggressive NK-cell leukemia a


- style=”margin-left: 86pt”>
-
Childhood EBV-positive T-cell and NK-cell lymphoproliferative disordersSystemic EBV-positive T-cell lymphoma in children
T/NK cell type chronic active EBV infection, systemic seedpox blister-like lymphoid tissue proliferative disease
Severe mosquito bite allergy
- style=”margin-left: 62pt”>
- Adult T-cell leukemia/lymphoma
- Extra-nodal NK/T-cell lymphoma, nasal type
-
Intestinal T-cell lymphoma
Intestinal disease-associated T-cell lymphoma
Enterotypic epitheliophilic intestinal T-cell lymphoma enterocytic lymphoma, non-specific
- Intestinal disease-associated T-cell lymphoma
- Haploid epitheliophilic intestinal T-cell lymphoma
- Proliferative disease of inert T-cell lymphoid tissue of the gastrointestinal tract a
- Hepatosplenic T-cell lymphoma
- Subcutaneous lipofuscinosis-like T-cell lymphoma
- Mycosis fungoides
-
Sézary’s syndrome
-
Lymphomatoid papulosis with primary cutaneous CD30-positive T-cell lymphoproliferative disorder
Primary cutaneous mesenchymal large cell lymphoma
-
Primary cutaneous peripheral T-cell lymphoma, rare subtype of cutaneous primary γ/δ T-cell lymphoma
Primary cutaneous CD8-positive aggressive pro-epidermal cytotoxic T-cell lymphoma a
Primary cutaneous limbic CD8-positive T-cell lymphoma a
Primary cutaneous CD4-positive small/medium T-cell lymphoproliferative disorder a
-
- Peripheral T-cell lymphoma, non-specific
- Intestinal disease-associated T-cell lymphoma
- Angioimmunoblast T-cell lymphoma and other T follicular helper cell-derived lymph node lymphomas


Angioimmunoblastoma T-cell lymphomaFollicular T-cell lymphoma
Peripheral T-cell lymphoma with follicular-associated T-cell phenotypic lymph nodes
- style=”margin-left: 68pt”>
- Melanotic large cell lymphoma, ALK-positive
- Megamorphic large cell lymphoma, ALK-negative
- Breast implant-associated mesenchymal large cell lymphoma a
Hodgkin’s lymphoma
- style=”margin-left: 68pt”>
-
Classical Hodgkin’s lymphoma
Nodular sclerosis type
Mixed cell type rich in lymphocytes
Lymphocyte-ablative
 Nodular lymphocyte-dominant Hodgkin’s lymphoma
Nodular lymphocyte-dominant Hodgkin’s lymphoma
Note: IRF4 (interferon regulatory factor 4). EBV
(Epstein-Barr virus, EBV); HHV8 (human herpes virus 8, human herpes virus type 8); ALK (anaplastic lymphoma kinase);a italics indicate Tentative name.
Annex 2. Staging System for Lymphoma
 Annex 2.1 Ann-Arbor (Cotswolds Revised) Staging System.
Annex 2.1 Ann-Arbor (Cotswolds Revised) Staging System.Stage I: Invasion of a lymph node area (I), or invasion of a single extra-lymph node organ or site
(IE).
Stage II: on one side of the diaphragm, invading two or more lymph node areas (II) or plus limited invasion of one extra-nodal organ or site (IIE).
Stage III: invasion of lymph node areas on both sides of the diaphragm (III) or additional limited invasion of an extra-nodal organ or site (IIIE) or spleen (IIIS) or both (IIIES).
 Stage IV: Diffuse or disseminated invasion of one or more extra-nodal organs with or without lymph node invasion.
Stage IV: Diffuse or disseminated invasion of one or more extra-nodal organs with or without lymph node invasion.Group A: No systemic symptoms.
Group B: systemic symptoms, including unexplained fever (>38°C for 3 or more consecutive days), night sweats (7 or more consecutive days), or weight loss (10

. = “https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_2022135.png” alt=””/>or more).E: Lymphoma involving extra-lymph node organs. A single extra-nodal site is invaded, and the lesion invades the lymph node with
If the lesion invades an organ/tissue directly connected to the lymph node, it is not recorded as stage IV, but should be entered as “E” after each stage (e.g., if the lesion infiltrates into the skin of the node connected to the left cervical lymph node, it is recorded as “IE”). ).
 X: Large tumor mass with tumor diameter > 1/3 of the thoracic width or fusion mass with maximum diameter > 10cm.
X: Large tumor mass with tumor diameter > 1/3 of the thoracic width or fusion mass with maximum diameter > 10cm.Annex 2.2 Rai staging and Binet staging system for chronic lymphocytic leukemia
Staging<
clinical features
Danger
Layering
Median survival
(months)
0
Lymphocytosis, peripheral blood lymphocyte count
>>5×109/L, and the percentage of lymphocytes in the bone marrow is >40

Low risk
>105
I
Stage 0 with enlarged lymph nodes
Medium risk
101
< span style="font-family:imitation-song; font-size:12pt">II
Stage 0 to I with splenomegaly, hepatomegaly, or both
Intermediate risk
71
III
< span style="font-family:imitation-song; font-size:12pt">Stage 0-II with hemoglobin <110g/L or erythrocyte pressure <
Stage 0-II with hemoglobin <110g/L or erythrocyte pressure <
high-risk
19
IV
33

Stage 0 to III with platelets <100×109/L
High Risk
19
>


Stage A Hemoglobin ≥100g/L, platelets ≥100×109/L, involved lymph node areas <3 Stage B Hemoglobin ≥100g/L, platelets ≥100×109/L, with ≥3 lymph node areas involved
 Stage C hemoglobin <100g/L and/or platelets <100×10 >9/L, with no restriction on the area of involved lymph nodes
Stage C hemoglobin <100g/L and/or platelets <100×10 >9/L, with no restriction on the area of involved lymph nodes
Annex 2.3 TNMB staging system for mycosis fungoides and Sezary syndrome
Staging Define skin (T)
 Stage T1 Restricted patches, papules and/or plaques, <10
Stage T1 Restricted patches, papules and/or plaques, <10  body surface area T2 stage patches, papules and/or plaques, ≥10
body surface area T2 stage patches, papules and/or plaques, ≥10  body surface area
body surface areaT3 stage 1 or more mass formation (≥1 cm in diameter) T4 stage Confluent erythema ≥80
 body surface area
body surface areaLymph nodes (N)
N0 stage No abnormal lymph nodes; no biopsy required
Stage N1 abnormal lymph nodes; histopathology of Dutch grade 1 or NCI LN grade 0-2 Stage N2 abnormal lymph nodes; histopathology of Dutch grade 2 or NCI LN grade 3
Stage N3 abnormal lymph nodes; histopathology of Dutch grade 3-4 or NCI LN grade 4 Stage Nx abnormal lymph nodes; no histologic confirmation
Visceral (M)
M0 stage No visceral organ involvement
M1 stage Visceral involvement (pathology must be confirmed and organ involvement indicated) Mx stage Visceral abnormalities; no histological confirmation
Blood (B)
Stage B0 No significant blood involvement: heterotypic cells (Sezary cells) to peripheral blood lymphocytes ≤ 5

Phase B1 Low-load blood involvement: heterotypic cells (Sezary cells) to peripheral blood lymphocytes ratio >5
 , but not at B2 level
, but not at B2 levelPhase B2 High-load blood involvement: heterotypic cells (Cezarie cells) ≥ 1,000/ul or CD4 (+)
 /CD7(-) cell ratio ≥ 40
/CD7(-) cell ratio ≥ 40  or CD4(+)/CD26(-) cell ratio ≥30
or CD4(+)/CD26(-) cell ratio ≥30Mycosis fungoides and Sezary syndrome TNMB staging system
< span style="font-family:imitation-song; font-size:12pt">Staging
T Staging
N Staging
M Staging
B Instalment
Phase IA
Phase IA
T1
N0
M0
M0
B0~1
Ib Issue
T2
N0
M0
B0 to 1
< col style="width:110px"/> IIA period
Phase IIB
T1 to 2
T3
N1 ~2
N0 to 2
M0
M0
B0 ~1
B0 to 1
< td style="border-top: none"> IIIA period
T4
>
N0 to 2
M0
B0
td>
IIIB period
T4
N0 to 2
M0
B1
IVA1 Issue
T1 to 4
N0~2
>
M0
< /td>
B2
IV A2 period
T1 to 4
N3
M0
M0
B0~2
IVB period
T1~4
N0 to 3
M1
M1
B0~2 
Annex 2.4 Lugano staging system for gastrointestinal lymphoma
Stage IE: lesions confined to the gastrointestinal tract
Stage IE1: Invasion of the mucosa and submucosaⅠE2: Invasion of the intrinsic muscular layer and plasma layer
Stage IIE: Lesions spread to the abdominal cavity
IIE1: Involvement of local lymph nodes IIE2: Involvement of distant lymph nodes
Stage IIIE: Invasion of plasma membrane layer to adjacent organs or tissues
 Stage IV: disseminated extra-nodal organ involvement or supradiaphragmatic lymph node invasion
Stage IV: disseminated extra-nodal organ involvement or supradiaphragmatic lymph node invasion
Annex 2.5 CA staging system for nasal NK/T-cell lymphoma
Stage I: lesions invade the nasal cavity or nasopharynx without local invasion of the tumor (skin, bone, paranasal sinuses)
Stage II: Non-nasal lesions or lesions invading the nasal cavity or nasopharynx with local invasion (skin, bone, paranasal sinuses)
Stage III: lesion with regional lymph node invasion
 Stage IV: non-regional lymph node invasion or lymph node invasion above and below the diaphragm or extensive disseminated lesions
Stage IV: non-regional lymph node invasion or lymph node invasion above and below the diaphragm or extensive disseminated lesions
Annex 3 Lymphoma Efficacy Determination CriteriaAnnex 3.1 Deauville 5-point scale
 Score (points) PET-CT findings
Score (points) PET-CT findings- style=”margin-left: 89pt”>
- No uptake
- Uptake value of lesions or other normal tissue ≤ mediastinum
- Uptake of lesions or other normal tissue > mediastinum but ≤ liver
- The degree of uptake of lesions or other normal tissues is moderately increased compared to the liver
- style=”margin-left: 41pt”>
 The uptake value of the lesion or other normal tissue is significantly higher than that of the liver and/or new lesion X The new area of uptake is unlikely to be associated with lymphoma
The uptake value of the lesion or other normal tissue is significantly higher than that of the liver and/or new lesion X The new area of uptake is unlikely to be associated with lymphoma

Annex 3.2 Lugano 2014 Lymphoma Treatment Effectiveness Evaluation Criteria
Efficacy Focal area PET-CT evaluation CT evaluation


Complete Lymph node and extranodal remission Involved site
Complete metabolic remission Complete imaging remission (including the following)
5-point scale (5-PS) score 1, 2, lymph node target lesion length ≤
3 score with or without residual mass shadowing; note: metabolism may be higher in pharyngeal lymphatic rings, extra-nodal high metabolic uptake organs such as spleen or bone marrow after granulocyte colony-stimulating factor intervention mediastinum
/hepatic blood pool, when the uptake at the site of infiltration does not exceed the surrounding normal tissue, is judged to be in complete remission
1.5cm; extra-nodal lesions disappear
Non-measurable lesions Not applicable Disappear
Organ enlargement N/A Return to normal
New lesions None None
Bone marrow No FDG metabolic hyperplastic lesions Normal morphology; if morphology not possible
 Determined, immunohistochemical confirmation of negative is required
Determined, immunohistochemical confirmation of negative is requiredPartial Lymph node and extranodal Partial metabolic remission Partial remission, including the following conditions.
remission Involved site
Score 4 or 5, reduced uptake compared to baseline, image residual lesions may
Decrease in the sum of the product of the vertical diameters of up to 6 lymph nodes and extra-nodal lesions
for any size; for midterm evaluation, ≥50
 . When the lesion is so small that CT cannot
. When the lesion is so small that CT cannotThe above suggests effective treatment; evaluation of effectiveness at the end of treatment suggests possible lesion residual
Measurements, uniformly set at 5 mm x 5 mm; when lesions are invisible, set at 0 mm x 0 mm; when lymph nodes are larger than 5 mm x 0 mm
5mm, take the actual value
Non-measurable lesion Not applicable Disappearing/fading/maintaining, not increasing
Organ Enlarged
Not applicable
Not applicable
Longer than normal spleen diameter
Increasing value decreases by >50 
New lesions
None
None
Bone marrow
< span style="font-family:imitation-song; font-size:12pt">higher than normal bone marrow uptake, but higher
Not applicable
baseline reduction; if lymph nodes shrink
=”font-family:imitation-song; font-size:12pt”>Case of persistent focal bone marrow
abnormal sexual changes that require consideration of biopsy or
or scan again
Disease
Lymph nodes and extranodal
Lymph nodes and extranodal
improvement Disease Stability
Stability
Participating site
Participating site
=”font-family:imitation-song; font-size:12pt”>Evaluated at mid-term or at the end of treatment, with evaluation
Up to 6 lymph nodes and extranodal disease
scored 4 or 5 compared to baseline
The focal length diameter multiplied by the corresponding vertical diameter
No significant change in uptake value
The sum of the products is reduced by <50

Non-measurable lesions
Not applicable
Not up to disease progression
Organ enlargement
Not applicable
>
Not up to disease progression
New lesions
No
No
No Bone marrow
No change from baseline
Not applicable
Disease
Lymph node target lesions
Scoring 4 or 5, with a higher baseline of intake
“font-family:仿宋; font-size:12pt”>Meet at least 1 of the following
Progression
/lymph node fusion
/lymph node fusion
elevated and/or in mid-stage or treated nodes elevated and/or in mid-stage or treated nodes
1 lymph node lesion needs to meet the criteria of < span style="font-family:imitation-song; font-size:12pt">Masses/Extra-nodal Disease
New FDG uptake during bundle evaluation
Next abnormal condition: length diameter > 1.5cm<
Zao
Take of augmentation lesions
< span style="font-family:imitation-song; font-size:12pt">and the long diameter multiplied by the corresponding vertical diameter
< td>
The sum of the products increases by ≥
50
 ; lesions ≤2cm in length:
; lesions ≤2cm in length:< span style="font-family:imitation-song; font-size:12pt">Long or short diameter increase by 0.5cm; long
Latio >2cm: long or short
Diameter increase by 1cm
When the spleen is large, the long diameter increases >previously more
50
 ; if the baseline
; if the baselineNo splenomegaly, long diameter needs to be on the base value
increase >2cm; new or recurrent
Splenomegaly
Non-measurable lesions
No new lesions or
Previously non-measurable lesions clearly progressing
New lesions Newly developed foci with increased FDG uptake after exclusion of inflammation, infection, etc.; if the nature of the new lesion is uncertain biopsy needs to be considered
 Bone marrow New or recurrent foci of increased FDG uptake
Bone marrow New or recurrent foci of increased FDG uptakeEnlarged primary remission lesion; new lymph node >1.5cm in any diameter; new extranodal lesion >1cm in any diameter; confirmation of lymphoma association if <1cm; any lesion clearly associated with lymphoma size lesion
New or recurrent infiltrates
5PS (five-point scale); a 5PS score of 3 usually predicts a good prognosis with standard therapy in most patients, especially at midterm evaluation. A score of 3 is usually considered poor in most patients with standard therapy, especially at midterm evaluation, but in step-down clinical trials involving PET to avoid undertreatment, a score of 3 is usually considered poor; definitions of measurable lesions: 1) lymph nodes: regionally, preferably including mediastinal and retroperitoneal regions; 2) non-lymph node lesions: including solid organs (e.g., liver, spleen, kidney, lung, etc.), gastrointestinal tract, skin, and primary diagnosable lesions.
PET-CT (positron emission tomography-computed tomography FDG (fluorodeoxyglucose).
Annex 4. Prognostic scoring system for lymphomaAnnex 4.1 HL prognostic score
 Early HL Adverse Prognostic Factors
Early HL Adverse Prognostic FactorsStudy group Early HL adverse prognostic factors


NCCN Erythrocyte sedimentation rate >50mm/1h or with B symptoms, mass maximal diameter/thoracic maximal diameter >
0.33 or >10cm in diameter with >3 lymph node areas involved
GHSG erythrocyte sedimentation rate >50mm/1h without B symptoms; erythrocyte sedimentation rate >30mm/1h with B symptoms, mass maximal diameter/thoracic maximal diameter >0.33, >2 lymph node areas involved, extra nodal lesions
EORTC Age ≥50 years, erythrocyte sedimentation rate >50mm/1h without B symptoms; erythrocyte sedimentation rate
>30mm/1h with B symptoms, mass maximal diameter/thoracic T5/6 level transverse diameter >0.35, involved lymph node area >3
NCIC Age ≥ 40 years, mixed cell or lymphocytic decompensation, erythrocyte sedimentation rate > 50mm/1h or with B symptoms. Mass maximal diameter/thoracic maximal diameter > 0.33 or diameter >
 10cm, >3 lymph node areas involved
10cm, >3 lymph node areas involvedNCCN (National Comprehensive Cancer Network); GHSG Comprehensive Cancer Network); GHSG
(German Hodgkin Study Group); EORTC (European Organization for Research and Treatment of Cancer) European Organization for Research and Treatment of Cancer); NCIC (National Cancer Institute, Canada)

 International Prognostic Score (IPS) for Advanced Hodgkin’s Lymphoma Item 0 points 1 point
International Prognostic Score (IPS) for Advanced Hodgkin’s Lymphoma Item 0 points 1 pointAlbumin ≥40g/L < 40g/L
Hemoglobin ≥ 105g/L < 105g/L
Male No Yes
IV period No Yes
White blood cells <15×109
/span>/L ≥ 15×109/L
Lymphocytes Percentage of white blood cells <8 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_2022176.png" alt=""/>and/or count
 <0.6×109 /L
<0.6×109 /LAs a percentage of white blood cells ≥8
 and counts ≥ 0.6×109/L
and counts ≥ 0.6×109/L International Prognostic Score and Survival in Advanced Hodgkin’s Lymphoma
International Prognostic Score and Survival in Advanced Hodgkin’s Lymphoma< span style="font-family:imitation-song; font-size:12pt">Score
5-year progression-free survival rate (
)
5 years Overall survival rate (
)
0 points
84
89
1 point
77
90
2 points
2 points
67
81
81 3 points
60
78
4 points
51
51
61 ≥5 points
42
56
Attachments 4.2 Prognostic score for diffuse large B-cell lymphoma
International Prognostic Index (IPI) >
Item 0 points
1 point
Age (years) ≤60
>60
ECOG rating 0 or 1
Grade 2 to 4
Clinical stage I or II
III or IV
Number of invasive sites outside the node <2
≥2
LDH Normal
elevated
ECOG (Eastern Cooperative Oncology Group); LDH
(lactate dehydrogenase)
Risk grouping
Number of risks
5-year progression-free survival
5-year overall survival
Low risk
0 or 1
< span style="font-family:imitation-song; font-size:12pt">70
73

Low-Medium Risk
2
50

51

High-Medium Risk
3
49

43

High Risk
4 or 5
40

26

 Revised International Prognostic Index (Revised IPI, R-IPI)
Revised International Prognostic Index (Revised IPI, R-IPI)Item 0 points 1 point


Age (years) ≤60 >60
ECOG score 0 or 1 level 2 to 4
Clinical stage I or II III or IV
Number of invasive sites outside the node <2 ≥2
 LDH Normal Ascending
LDH Normal AscendingECOG (Eastern Cooperative Oncology Group); LDH
(lactate dehydrogenase)
Risk grouping
Number of risks
4-year progression-free survival
>
4-year overall survival
Prognosis is very good
0
94

92

Good prognosis
1 to 2
82

82

Poor prognosis
3 to 5
45 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_2022197.png" alt=""/>
58


 Age Age Adjusted International Prognostic Index (age adjusted IPI, aaIPI)
Age Age Adjusted International Prognostic Index (age adjusted IPI, aaIPI)Item 0 score 1 score ECOG score 0 or 1 level 2 to 4
Clinical stage I or II III or IV
 LDH Normal Ascending
LDH Normal AscendingECOG (Eastern Cooperative Oncology Group); LDH
(lactate dehydrogenase)
Risk Subgroups
Number of risks
5-year disease-free survival
5-year overall survival
Low risk
0
56

83

Low-Medium Risk
>
1
44

69

High- Mid-risk
2
37

46

high-risk
3
21

32

Annex 4.3 Follicular lymphoma prognostic score

 Follicular Folicullar lymphoma International Prognostic Index (FLIPI) Item 0 points 1 point
Follicular Folicullar lymphoma International Prognostic Index (FLIPI) Item 0 points 1 pointAge (years) <60 ≥60 Hemoglobin level ≥120g/L <120g/L
Clinical stage Ⅰ or Ⅱ Ⅲ or Ⅳ
Number of invasive lymph nodes <5 ≥5
 LDH Normal Ascending
LDH Normal AscendingLDH (lactate dehydrogenase)
 Risk Grouping and Survival in Follicular Lymphoma International Prognostic Index
Risk Grouping and Survival in Follicular Lymphoma International Prognostic IndexRisk Group Score Proportion of Patients (
 ) 5-year overall survival rate (
) 5-year overall survival rate ( ) 10-year overall survival (
) 10-year overall survival ( )
)Low risk
0~1
36
90.6
< span style="font-family:imitation-song; font-size:12pt">70.7
Mid-risk
2
37
77.6
50.9
High Risk
3 to 5<
27
52.5
. /span>
35.5
Follicular Lymphoma International Prognostic Index 2 (Folicullar lymphoma IPI 2, FLIPI2)
Project< /p>
0 points
1 point
Age (years)<
<60 ≥ 60
≥
Hemoglobin level
≥120g/ L
<120g/L
td>
Lymph node longest diameter<
≤6cm
>6cm
β2 microglobulin
normal
elevated
Bone marrow
Uninfringed
infested
 Risk Grouping and Survival for Follicular Lymphoma International Prognostic Index 2
Risk Grouping and Survival for Follicular Lymphoma International Prognostic Index 2 Risk Group Score 5-year overall survival (
Risk Group Score 5-year overall survival ( ) 5-year progression-free survival (
) 5-year progression-free survival ( ) Low risk 0 or 1 98 79
) Low risk 0 or 1 98 79< col style="width:125px"/> Mid-risk
2
88
51
< tr style="height: 31px">
High risk
3 to 5
77
20
Annex 4.4 Prognostic score for sleeve cell lymphoma
 Mantle cell lymphoma international prognostic index (MIPI)
Mantle cell lymphoma international prognostic index (MIPI)ECOG (Eastern Cooperative Oncology Group); LDH
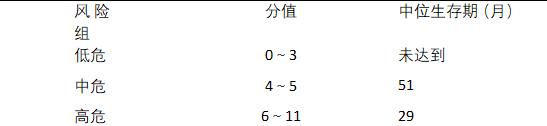 (lactate dehydrogenase) International Prognostic Index and Survival of Sleeve Cell Lymphoma
(lactate dehydrogenase) International Prognostic Index and Survival of Sleeve Cell Lymphoma The combined mantle cell lymphoma international prognostic index (MIPIc) with Ki-67
The combined mantle cell lymphoma international prognostic index (MIPIc) with Ki-67
 MIPI-c Prognosis MIPI Prognosis Ki-67 Index Low Risk Group Low Risk Group <30
MIPI-c Prognosis MIPI Prognosis Ki-67 Index Low Risk Group Low Risk Group <30 
Low-risk group ≥30

 Low to medium risk group
Low to medium risk groupHigh and medium risk groups
Mid-risk group <30

Mid-risk group ≥30

High-risk group <30

 < img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_2022233.png" alt=""/>
< img src="https://www.kiraspecialist.com/wp-content/uploads/2022/06/062222_1008_2022233.png" alt=""/>High Risk Group High Risk Group ≥30

Annex 4.5 Peripheral T-cell lymphoma, non-specific prognostic score
Project< /p>
0 points
1 point
Age (years)< /p>
≤60
> 60
Bone marrow invasion
No
Yes
ECOG Rating
Grade 0 or 1
Level 2 to 4
LDH
normal< /p>
elevated
ECOG (Eastern Cooperative Oncology Group (Eastern Oncology Group); LDH
 (lactate dehydrogenase)
(lactate dehydrogenase)Score
5-year overall survival rate (
)
10-year overall survival rate (
 )
)0
62.3
54.9<
1
< td>
52.9
38.8
2
32.9
18.0
3~4
18.3
12.6
Annex 4.6 Prognostic scoring system for NK/T-cell lymphoma
Prognostic Index of Natural Killer Lymphoma (NK/T-cell Lymphoma.
PINK)
Risk Factors
td> 1 point
Age (years) Stage III/IV
Distant lymph node invasion
Non-nasal primary
>60 have Yes
Yes
<
Score
Risk stratification
3-year overall survival rate (
 )
)0
Low Risk
81
1
< span style="font-family:imitation-song; font-size:12pt">Mid-risk
62
≥2
High risk
25
< /tbody>
 Prognostic Index of Natural Killer Lymphoma with Epstein- Barr Virus DNA, PINK-E)
Prognostic Index of Natural Killer Lymphoma with Epstein- Barr Virus DNA, PINK-E) Risk factors 1 point
Risk factors 1 pointAge (years) >60
Stage III/IV Yes
Distant lymph node invasion Yes
Non-nasal primary Yes
 EBV DNA is detectable
EBV DNA is detectableScore
Risk stratification
3-year overall survival rate (
 )
)0 to 1
Low risk
81
1
mid-risk
55
≥3
high-risk
28
Attachment 5
Lymphoma Diagnostic and Treatment Guidelines (2022 Edition) Development and Validation Expert Group
(in order of last name stroke)
Team leader: Shi Yuankai
Members: Ma Jun, Wang Huaqing, Lu Xiaoyang, Feng Li, Zhu Jun, Zhu Mingqing, Zhu Xiongzeng, Li Yexiong, Lin Tongyu, Guo Xiaomao, Jiang Wenqi, Gao Zifen, Qin Yan, Xie Chuanmiao
-
-
-



