Pancreatic Cancer Treatment Guidelines
(2022 Edition)
I. Overview
In recent years, the incidence of pancreatic cancer has been on a significant rise both at home and abroad.
The year 2021 statistics show that among all malignancies in the United States, new cases of pancreatic cancer
Men ranked 10th and women ranked 9th in terms of new cases of pancreatic cancer among all malignancies in the United States. 9 th, accounting for malignancy-related mortality
of the 4th ranking. China National Cancer Center 2021 statistics show that pancreatic cancer
Ranked 7th in incidence of malignant tumors in men and 11th in incidence of malignant tumors in women in China. Roman”>11th position, accounting for the evil
The 6th ranking for malignancy-related mortality. (All pancreatic cancers described herein refer specifically to pancreatic ductal adenocarcinoma)
In recent years, the diagnosis of pancreatic cancer has been improved with the development of imaging, endoscopy, pathology and other disciplines; the development of new concepts and techniques in surgery (e.g. laparoscopic techniques, robotics, etc.), local treatment methods (e.g. stereotactic radiotherapy, nano-ablative therapy, particle source implantation), and the development of the pancreatic cancer diagnosis. knife ablation therapy, particle source implantation, etc.) and the use of antitumor drugs (e.g., gemcitabine, nanoalbumin paclitaxel, tegeo, capecitabine, irinotecan, oxaliplatin, nitrozumab, etc.) have brought opportunities and advances in the treatment of pancreatic cancer.
This guideline was developed to further standardize the practice of pancreatic cancer treatment in China, improve the level of pancreatic cancer treatment in medical institutions, improve the prognosis of pancreatic cancer patients, and ensure medical quality and medical safety. Although the guideline is intended to assist in clinical decision making, it cannot incorporate all possible clinical variations. This guideline applies only to malignancies of ductal epithelial origin of the pancreas.
II. Diagnostic Techniques and Applications
(i) High-risk factors.
The etiology of pancreatic cancer is not fully understood, and epidemiological surveys have shown that the development of pancreatic cancer is associated with multiple risk factors. Non-genetic risk factors: long-term smoking, advanced age, high-fat diet, overweight body mass index, chronic pancreatitis or concomitant diabetes are possible non-genetic risk factors for pancreatic cancer. Hereditary risk factors: Family inheritance is also a high risk factor for pancreatic cancer, with approximately 10% of pancreatic cancer cases having family inheritance. Patients with hereditary pancreatitis, Boyds– Yeager syndrome, familial malignant melanoma, and other hereditary neoplastic diseases are at significantly increased risk for pancreatic cancer. The genetic basis for these genetic predispositions is not yet clear, and up to 80% of patients with pancreatic cancer have no known genetic cause. CDKN2A, BRCA1/2, PALB2 and other gene mutations have been shown to be strongly associated with familial pancreatic cancer development.
(ii) Clinical presentation.
Pancreatic cancer is highly malignant and progresses rapidly, but its onset is insidious and early symptoms are atypical, and most patients are already in the middle or late stage when they are seen in the clinic. The first symptoms often depend on the location and extent of the tumor, for example, obstructive jaundice can appear in the early stage of pancreatic head cancer; while early pancreatic body tail tumor usually does not have jaundice. The main clinical manifestations include.
-
Abdominal discomfort or pain: this is the common first symptom. Most patients with pancreatic cancer only present with upper abdominal discomfort or vague pain, dull pain and distension. It is easily confused with symptoms of gastrointestinal and hepatobiliary diseases. If there is also obstruction of the pancreatic outlet, pain or discomfort may increase after eating. Tumor invasion of the abdominal plexus in the middle and late stages may lead to persistent severe abdominal pain.
- Loss of weight and weakness:< /span>80%~90%90%of pancreatic cancer patients have wasting, weakness, and weight loss at the beginning of the disease, associated with lack of appetite, anxiety, and tumor depletion.
- Gastrointestinal symptoms: When the tumor obstructs the lower bile duct and pancreatic duct, the bile and pancreatic fluid cannot enter the duodenum, and indigestion symptoms often occur. Exocrine function of the pancreas may be impaired, leading to diarrhea. In the late stage, pancreatic cancer invades the duodenum and may cause obstruction or bleeding in the digestive tract.
- Jaundice: associated with biliary outlet obstruction, is the main clinical manifestation of pancreatic head cancer, which may be accompanied by skin pruritus, dark tea-colored urine and clay-like stools.
-
Other symptoms: Some patients may have persistent or intermittent low-grade fever and generally no biliary tract infection. Some patients may also have abnormal blood glucose.
(iii) Physical examination.
Pancreatic cancer has no obvious physical signs in the early stage, and as the disease progresses, signs such as wasting, epigastric pressure and jaundice may appear.
- style=”margin-left: 44pt”>
- Wasting: advanced patients often appear cachexia.
- Wasting: advanced patients often appear cachexia.
- Jaundice: Most often seen in pancreatic head cancer, due to biliary outlet obstruction resulting in bile stasis.
- Hepatomegaly: As a result of biliary stasis or liver metastasis, the liver is hard, mostly painless, and smooth or nodular in appearance.
- Gallbladder enlargement: Some patients can palpate a cystic, non-pressure, smooth and pushable gallbladder, called Kuvasier’s sign, which is characteristic of periampullary carcinoma.
-
Abdominal mass: An abdominal mass, mostly located in the upper abdomen, is deep, nodular, hard, and immobile in the advanced stage.
- style=”margin-left: 44pt”>
- Other signs: Advanced pancreatic cancer may present with enlarged supraclavicular lymph nodes, abdominal
- Other signs: Advanced pancreatic cancer may present with enlarged supraclavicular lymph nodes, abdominal
Water and other signs. A periumbilical mass, or palpable rectal –vaginal or rectal –posterior bladder wall nodule.
(iv) Imaging.
Imaging is an important tool for obtaining a preliminary diagnosis and accurate staging, and the scientific and rational use of various imaging methods plays an important role in standardizing diagnosis and treatment. According to the condition, choosing the appropriate imaging technique is a prerequisite for diagnosing occupying pancreatic lesions. Imaging should be complete (showing the whole pancreas), fine (thin layer thickness 1 to 2mm), dynamic (dynamic enhancement, regular follow-up), and the pancreatic occupying lesion should be diagnosed. (dynamic enhancement, regular follow-up), and stereoscopic (multi-axis reconstruction for a comprehensive understanding of the adjoining relationships) are the basic principles. Please see Appendix 1 and Appendix 2 for pre- and post-treatment imaging procedures.
-
Ultrasound: Ultrasound is a primary screening test for pancreatic cancer diagnosis because of its simplicity, flexibility and intuitiveness, non-invasive and non-radiation, and the ability to observe in multiple axes.
Conventional ultrasound can better show the internal structure of the pancreas, observe whether there is obstruction in the biliary tract and the site of obstruction, and look for the cause of obstruction. Color Doppler ultrasound can help determine whether the tumor is compressing or invading the surrounding large blood vessels. Real-time ultrasonography can reveal hemodynamic changes in tumors, help identify and diagnose tumors of different nature, and have advantages in evaluating tumor microvascular perfusion and guiding interventions by virtue of the flexible nature of real-time imaging and multi-sectional imaging.
Limitations of ultrasound include a small field of view, which is affected by gas in the gastrointestinal tract, patient size, and other factors that sometimes make complete visualization of the pancreas, especially the tail of the pancreas, difficult.
-
CTExamination: With better spatial and temporal resolution, it is the best noninvasive imaging method to examine the pancreas, mainly used for the diagnosis, differential diagnosis and staging of pancreatic cancer. Plain scan can show the size and location of the lesion, but cannot accurately
Deterministically diagnose pancreatic lesions, and the relationship between tumor and surrounding structures The ability to show the relationship between the tumor and the surrounding structures is poor. The three-stage enhancement scan can better show the size, location, morphology, internal structure and relationship with surrounding structures of the pancreatic mass, and can accurately determine the presence of liver metastases and show enlarged lymph nodes.
- MRI and magnetic resonance pancreaticobiliary imaging examination: not as the preferred method to diagnose pancreatic cancer, with the improvement of MR scanning technology, the increase of temporal resolution and spatial resolution has greatly improved MR image quality and improved MRI diagnostic accuracy has shown increasing value in showing pancreatic tumors, determining vascular invasion, and accurate clinical staging, while family:Times New Roman”>MRI has the characteristics of multiparametric, multiplanar imaging and no radiation, and can be used as a diagnostic tool when the differential diagnosis of pancreatic lesions is difficultCT enhanced scan is a useful supplement; when patients are interested in CT enhanced contrast can be used when the patient is allergic to MR instead of enhanced contrast. span>CT scan for diagnosis and clinical staging; the application of magnetic resonance pancreaticobiliary imaging and multi-phase enhancement scan is more advantageous in the qualitative diagnosis and differential diagnosis of pancreatic cancer. It has been reported that MRI using tissue-specific contrast can diagnose occult pancreatic head cancer. MRI also monitors pancreatic cancer and can predict recurrence of pancreatic cancer, vascular invasion, and also pancreatic tumor aggressiveness, while pancreatic cancer tissue invasion can be used as an indicator of survival prediction. Magnetic resonance cholangiopancreatography can clearly show the whole picture of the pancreaticobiliary system and help determine the site of lesions, thus helping to detect and differentially diagnose peri-potbelly tumors, and is compatible with endoscopic retrograde cholangiopancreatography (Endoscopic Retrograde Cholangiopancreatography, ERCPand percutaneous transhepatic cholangiography, PTC) has the advantage of being non-invasive compared to ; in addition, < MR functional imaging can quantitatively reflect tumor metabolic information from a microscopic perspective, including diffusion
weighted imaging, perfusion-weighted imaging and spectral imaging, which need to be compared with MR conventional sequences need to be closely integrated to play a greater role in the diagnosis, differential diagnosis, and outcome of pancreatic cancer.
- Positron Emission Tomography (PET/CT PET/CT)/ and PET-MRI: shows the metabolic activity and metabolic load of the tumor, and has significant advantages in detecting extra-pancreatic metastases and evaluating the systemic tumor load advantage. In clinical practice: 1) it is not recommended as a routine test for pancreatic cancer diagnosis, but it can be used as CT and/or MRI is a complementary means of examining lesions that cannot be clearly diagnosed and helps to distinguish between benign and malignant tumors; however, its role in diagnosing small pancreatic cancer is limited. ②PET/CT examination is advantageous in excluding and detecting distant metastatic lesions, for large primary lesions, suspected regional lymph node metastases and glycoantigens 19-9(carbohydrate New Roman”>carbohydrate antigen 19-9 ,CA19-9 >) is recommended in patients with significantly elevated (iii) In post-treatment follow-up of pancreatic cancer, to identify postoperative and post-radiotherapy changes from local tumor recurrence, for CA19-9 elevated and conventional imaging PET/CT is useful for the diagnosis and localization of recurrent metastatic lesions when the results of conventional imaging methods are negative. The results of PET/CT can be used to monitor the efficacy of glucose metabolism in inoperable patients who are treated with radiotherapy, which can provide a basis for clinical changes and more aggressive treatment.
-
Ultrasound Endoscopy () style=”font-family:Times New Roman”>endoscopic ultrasonography,EUS): the combination of ultrasound imaging on the basis of endoscopic techniques improves the sensitivity and specificity of pancreatic cancer diagnosis; in particular, ultrasound endoscopy-guided fine-needle aspiration biopsy
(endobronchial ultrasound-guided fine needle aspiration.
EUS-FNA), which has become the most accurate method for localizing and qualitatively diagnosing pancreatic cancer.
In addition, EUS also contributes to the determination of tumor staging . In recent years, EUS elastography-based tumor elastic strain rate testing can assist in determining the mesenchymal content of pancreatic cancer and guide clinical drug selection.
EUS is an invasive procedure, and its accuracy is greatly influenced by the operator’s skill and experience. For patients with proven diagnosis and surgical indications, preoperative routine EUS is not required.
- ERCP in the diagnosis of pancreatic cancer Role: The most common ERCP presentation of pancreatic cancer is proximal stenosis of the main pancreatic duct with distal dilatation. ERCP does not directly show the tumor lesion, it relies mainly on the changes of the pancreatic duct and the morphological changes of the common bile duct to make the diagnosis of pancreatic cancer, for The diagnosis of pancreatic cancer is mainly based on the morphological changes of the pancreatic duct and the common bile duct. In addition, intra-pancreatic bile duct cytology or biopsy can be performed, followed by pancreatic fluid and bile-related exfoliative cytology or pathology for diagnosis. In particular, in patients with inoperable obstructive jaundice, the reduction of yellowness and pathology and cytology can be performed in one visit.
-
Bone scan: the most widely used, experienced, cost-effective, and highly sensitive method for detecting bone metastases from malignant tumors. It is the most widely used, experienced, cost-effective, and has a high sensitivity in detecting bone metastases of malignant tumors. Preoperative bone scan can be routinely performed in pancreatic cancer patients with high suspicion of bone metastases.
(E) Blood immunobiochemical examination.
-
Blood biochemical examination: no specific blood biochemical changes in the early stage, but when the tumor involves the liver and obstructs the bile duct, it may cause corresponding biochemical indicators, such as glutathione transaminase. In the early stage, there is no specific blood biochemical change, but when the tumor involves the liver and obstructs the bile duct, it may cause the corresponding biochemical indicators, such as glutathione transaminase, glutamic oxalacetic transaminase, bile acid and bilirubin to increase. In the advanced stage of tumor, electrolyte disorders and hypoproteinemia may occur along with malignant fluid. In addition, changes in blood glucose are also associated with the onset or progression of pancreatic cancer, and patients need to be aware of the changes in blood glucose.
-
Blood Tumor marker testing: The tumor markers commonly used in clinical practice for pancreatic cancer diagnosis are CA19-9 , carcinoembryonic antigen ( >carcinoembryonic antigen , , CEA), glycan antigen 125(carbohydrate antigen 125, CA125), etc., where CA19-9is the most valuable tumor marker in pancreatic cancer, which can be used for adjuvant diagnosis, efficacy monitoring and recurrence monitoring. SerumCA19-9>37U/ml is a positive marker, and repeated tests are usually better than single tests, and repeated tests should be performed at least Repeat assays should be performed at least 14 days apart. Patients with untreated pancreatic ductal carcinomaCA19-9 can show a progressive increase that can be as high as 1000U/ml, sensitivity is related to tumor stage, size and location, specificity 72% to 90%. However, it should be noted that about 10% of patients with pancreatic cancer are Lewis antigen-negative blood group structure that does not express CA19-9< , so such pancreatic cancer patients are undetectable CA19-9 levels are abnormal and need to be combined with other tumor markers such as CEA,< span style="font-family:Times New Roman">CA125to assist in the diagnosis. Moreover, CA19-9 may be falsely positive in cases of biliary tract infection (cholangitis), inflammation, or biliary obstruction (regardless of the etiology) that do not suggest tumor or advanced lesions. Therefore, preoperative testing of CA19-9 levels is best performed after biliary decompression has been completed and bilirubin levels have returned to normal. CA19-9 measures usually correlate well with the clinical course, and surgical radical surgery (I stage) after surgical radical surgery (2 to 4 2 to 4 stage). span>weeks, the elevated CA19-9 can return to normal levels; in case of tumor recurrence or metastasis,CA19-9 can be elevated again. Serum CA19-9 levels may also reflect tumor load or the presence of possible micrometastases to some extent. The elevated serum CA19-9 levels in postoperative pancreatic cancer may indicate recurrence or metastasis, but it needs to be combined with imaging evidence and other comprehensive judgment.
(vi) Histopathological and cytological diagnosis.
Histopathological or cytological examination can determine the diagnosis of pancreatic cancer. By preoperative
or intraoperative cytologic aspiration, biopsy, or referral to an appropriate higher level hospital for histologic aspiration biopsy to obtain a definitive diagnosis. The surgical specimens included pancreaticoduodenectomy specimens and pancreatic caudal (+ spleen) resection specimens.
- style=”margin-left: 57pt”>
- Cytopathological diagnosis of pancreatic cancer
The guidelines for the cytopathologic diagnosis of pancreatic cancer consist of the sampling technique of the specimen, the production technique, and the diagnostic report.
Cell specimen retrieval techniques: There are four commonly used techniques for pancreatic cell specimen retrieval: 1) imaging (CT or ultrasound)-guided percutaneous fine needle aspiration biopsy (fine needle aspiration, FNA); ② EUS-FNA; ③ FNA in caesarean section.
④ Cell brushing of the pancreatic duct and terminal common bile duct during ERCP.
Production techniques for cellular specimens: Production techniques for cellular specimens include conventional smear, liquid-based production, and cell block sectioning. Conventional smear is the most commonly used filming method, where FNA or brushed cells are directly coated on the slide, dried, and 95% fixed in alcohol. alcohol fixed. If the FNA puncture material is cystic fluid, the liquid-based filming method will enrich the cells in the cystic fluid, resulting in a more abundant smear than conventional smears. The main purpose of cell block preparation is to perform immunocytochemical assays, and in addition, small tissue structures can be restored in cell block sections to aid in morphologic diagnosis.
Each unit can choose different methods of preparation depending on its own situation and the nature of the lesion, with 3 methods of preparation being used simultaneously to improve diagnostic accuracy. On-site evaluation of cellular specimens can also be performed in units where available to improve the satisfactory rate of sampling.
Diagnostic cytopathology reporting: The diagnostic cytopathology report uses the 6 level reporting system recommended by the American Academy of Cytopathology, in which cytology
diagnosis is divided into 6 diagnostic levels: I grade, not diagnostic; grade II, no malignancy seen.
Grade III, atypical; Grade IV A, neoplastic lesion, benign; Grade IVGrade B, neoplastic lesion, other; Grade V, suspicious malignant; Grade VI, malignant. The most challenging diagnostic classification is “Neoplastic lesions, other (IV B)“, intraductal papillary mucinous tumors and mucinous cystic tumors with cyst wall covered cells in this level of diagnosis can be mildly, moderately, or even severely atypical, and cells showing severe atypical changes are difficult to distinguish from adenocarcinoma cells. In addition, the diagnosis of tumors composed of small round cells, such as solid –pseudopapillary tumors, neuroendocrine tumors, and blastocytic carcinomas often requires the aid of immunocytochemical testing of cell blocks. See Appendix 3 for cytologic grading criteria.
- style=”margin-left: 57pt”>
- Histopathologic diagnosis of pancreatic cancer
-
Pancreatic cancer histopathological diagnosis criteria: biopsy or surgery for occupying lesions or metastases in the pancreas The tissue specimens were excised and diagnosed as pancreatic cancer by pathological histology and/or cytological examination. The pathological diagnosis must be combined with clinical evidence and a comprehensive understanding of the patient’s clinical presentation and imaging studies.
-
Pancreatic cancer pathological diagnosis guidelines: The pancreatic cancer pathological diagnosis guidelines consist of specimen handling, specimen sampling, pathological examination and pathological report.
- style=”margin-left: 56pt”>
- Key points of specimen handling
①The surgeon should mark the site, type and number of specimens to be sent for examination on the pathology request form, and the surgical margins and important lesions can be marked with dye staining or sutures.
Tumor specimens should be delivered to the pathology department for incision and fixation within 30 minutes of isolation, if possible.
③ 10% neutral formaldehyde solution for fixation 12~24 hours.
- Key points of specimen handling
- style=”margin-left: 69pt”>
- Specimen sampling and Examination
①Pancreaticoduodenectomy specimen: open the tumor with a probe through the duodenal papilla to the common bile duct, cut the tumor vertically through the common bile duct, and observe the relationship between the tumor and the wall of the common bile duct and duodenum. One piece was taken from each of the gastric resection margin, pylorus, small intestine resection margin, pancreatic resection margin and common bile duct resection margin; the main body of the tumor (including the deepest infiltration and the relationship with surrounding tissues or organs) was taken at least every 1 cm according to the size of the tumor. family:Times New Roman”>1 block; areas with different colors and textures in various sections of the bulk should also be taken.
②Pancreas body caudal + splenectomy specimens: the main body of the tumor is dissected in booklet form, and depending on the size of the tumor, at least every < span style="font-family:Times New Roman">1 cm Take 1 block, including the pancreatic peritoneum, pancreatic duct, pancreatic cut margin, surrounding pancreas, and relationship to the spleen. All lymph nodes were taken including peripancreatic lymph nodes and splenic hilar lymph nodes. The pancreatic tissue between the tumors needs to be taken for multiple tumors.
- style=”margin-left: 57pt”>
- Immunohistochemical examination
Commonly used markers are Vimentin, CK, EMA, CEA, CEA, CEA, CEA. span style=”font-family:Times New Roman”>CA19-9, CK19, CK7, CK20, MUC1, MUC1, < span style="font-family:Times New Roman">MUC4, CDX2, PR, CD10, CD10, CD10.
syn, CgA, CD56, ACT, AAT, β-cantenin, Ki-67 and so on. A rational combination of immunohistochemical markers is needed for the differential diagnosis of pancreatic endocrine tumors as well as various types of pancreatic tumors.
- style=”margin-left: 57pt”>
- Pancreatic cancer pathology diagnosis report
By gross specimen description, microscopic description, immunohistochemical findings, pathological diagnosis name, extent of infiltration (focus on the relationship with common bile duct, duodenum and spleen, if portal vein margin is involved, need to report whether portal vein margin is involved), presence of
The presence of metastasis, TNM staging, and other components. A general description of the requirements, with detailed requirements in Annex 4 and Annex 5, is required. In addition, molecular pathology findings related to drug target detection, biological behavior assessment, and prognostic determination may be included for clinical reference.
(VII) Differential diagnosis of pancreatic cancer.
-
Chronic pancreatitis: Chronic pancreatitis is a recurrent and progressive extensive pancreatic fibrotic lesion, resulting in pancreatic duct stenosis and obstruction. The pancreatic ducts are dilated and the drainage of pancreatic juice is obstructed. The main manifestations are abdominal pain, nausea, vomiting and fever. As with pancreatic cancer, there may be clinical manifestations such as epigastric discomfort, dyspepsia, diarrhea, loss of appetite, weight loss, etc. The two are differentiated as follows.
- Chronic pancreatitis has a slow onset, long history, often recurrent, and acute attacks may present with elevated hematuria, amylase, and rarely jaundice.
- AbdomenCT Examination reveals irregular pancreatic contours, nodular elevation, and uneven pancreatic parenchyma density.
-
Abdominal plain film and CT examination of calcified spots in the pancreatic area can be helpful for diagnosis.
- style=”margin-left: 74pt”>
- Serum =”font-family:Times New Roman”>IgG4 elevation is a specific type of diagnosis of chronic pancreatitis
— A more sensitive and specific laboratory indicator of autoimmune pancreatitis, and when imaging is difficult to differentiate Pathological examination is required to assist in the identification.
- Serum =”font-family:Times New Roman”>IgG4 elevation is a specific type of diagnosis of chronic pancreatitis
-
Potbelly cancer: Potbelly cancer occurs at the confluence of the common bile duct and pancreatic duct. Jaundice is the most common symptom and can appear early in the development of the tumor. The differentiation is as follows.
- style=”margin-left: 72pt”>
- Intermittent jaundice may occur as the tumor necrosis is dislodged and biliary obstruction is relieved.
- Intermittent jaundice may occur as the tumor necrosis is dislodged and biliary obstruction is relieved.
Jaundice.
- Duodenal hypotension angiography may show filling defects in the duodenal papilla and bilateral signs of mucosal destruction.
- Ultrasound,CT, MRI, , , , . span>ERCP etc. may show dilated pancreatic ducts and bile ducts, low biliary obstruction sites, double duct signs, and occupying lesions in the jugular abdominal region.
- Ultrasound endoscopy: As a new diagnostic technique, ultrasound endoscopy is unique in distinguishing pancreatic cancer from jugular cancer, detecting smaller lesions and observing the depth and extent of lesion infiltration and surrounding enlarged lymph nodes.
- The pancreatic endoscope is a new diagnostic technique for differentiating pancreatic cancer from pancreatic cancer.
-
Cystic adenoma and cystic adenocarcinoma of the pancreas: Cystic tumors of the pancreas are rare in clinical practice and occur mostly in female patients. It is rare and occurs in female patients. Imaging is an important tool to differentiate it from pancreatic cancer, and the tumor marker CA19-9 is not elevated. Ultrasound,CT,, EUS can show cystic lesions in the pancreas with regular cystic lumen, whereas pancreatic cancer only shows cystic lesions and irregular cystic lumen in the case of central necrosis.
-
Choledocholithiasis: choledocholithiasis tends to be recurrent with a long history of disease. Jaundice levels fluctuate widely, and attacks are often accompanied by the triad of abdominal pain, chills and fever, and jaundice, most of which are not difficult to identify.
-
Other occupying lesions of the pancreas: mainly including pancreatic pseudocysts, insulinoma, and pancreatic tumors. The clinical growth of the mass is usually slow and the course of the disease is long, and there may be specific clinical manifestations: for example, insulinoma may show symptoms of episodic hypoglycemia, and patients with pancreatic pseudocysts mostly have a history of acute pancreatitis, combined with CT and other imaging examinations are generally not difficult to identify, and if necessary, a puncture biopsy and pathological examination can assist in the diagnosis.
III. Classification and Staging of Pancreatic Cancer
(A) Histological types of pancreatic cancer.
Refer to the 2019 edition of the WHO Histologic Classification of Pancreatic Cancer (Annex 6).
(ii) Staging of pancreatic cancer (AJCC, p. 8 edition).
- style=”margin-left: 57pt”>
- Pancreatic CancerTNMstaging in T,N,,M is defined.
- style=”margin-left: 45pt”>
- Primary tumor (< span style="font-family:Times New Roman">pT)pTx: not assessable. pT0: no evidence of primary tumor.
pTis: carcinoma in situ, including high-grade pancreatic intraepithelial neoplasia of the pancreas (PanIN 3), intraductal papillary mucinous neoplasm with high-grade intraepithelial neoplasm, intraductal ductal papillary neoplasm with high-grade intraepithelial neoplasm, and mucinous cystic neoplasm with high-grade intraepithelial neoplasm.
pT1: Maximum tumor diameter ≤2 cm. /span>. pT1a: maximum tumor diameter ≤0.5cm.
pT1b: maximum tumor diameter ≤1cm , >0.5cm. pT1c: maximum tumor diameter 1 to 2cm. pT2: maximum tumor diameter > 2cm, ≤4cm. pT3: Maximum tumor diameter >4cm.
pT4: Tumor of any size involving the celiac trunk, superior mesenteric artery, or common hepatic artery.
- style=”margin-left: 85pt”>
- Regional lymph nodes (pN)
pNx: could not be evaluated.
pN0: no regional lymph node metastasis. pN1: 1 to 3 regional lymph node metastases. pN2: ≥4 regional lymph node metastases.
- style=”margin-left: 45pt”>
-
Distant metastases (pM). pMx: cannot be evaluated. pM0: no distant metastasis. pM1: with distant metastasis.



0 Tis, N0, M0
ⅠA T1, M0, N0
ⅠB T2, N0, M0
IIA T3, N0, M0
IIB T1, N1, M0
IIB T2, N1, M0
IIB T3, N1, M0
III T1, N2, M0
III T2, N2, M0
III T3, N2, M0
III T4, anyN, M0
IV anyT ,< span style="font-family:Times New Roman">anyN, M1

IV.
(a) Principles of treatment.
Integrated multidisciplinary diagnosis and treatment is the basis for the treatment of any stage of pancreatic cancer, and a multidisciplinary consultation model can be used to apply the available treatment methods in a planned and rational manner according to different patients’ physical condition, tumor site, invasion range and clinical symptoms, in order to maximize the eradication and control of tumor, reduce complications and improve patients’ quality of life. The treatment of pancreatic cancer mainly includes surgery, surgery, and surgery. The treatment of pancreatic cancer mainly includes surgery, radiotherapy, chemotherapy, interventional therapy and best supportive therapy. For patients to be treated with radiotherapy or chemotherapy, a Karnofsky (Appendix 7) or 7 should be performed. =”font-family:Times New Roman”>ECOG score (Annex 8).
(ii) Surgical treatment.
- style=”margin-left: 57pt”>
- Principles of surgical treatment
Surgical resection is the only effective way for patients with pancreatic cancer to have a chance of cure and long-term survival. However, more than 80% of patients with pancreatic cancer are lost to surgery due to late stage disease. Every effort should be made to perform radical resection (R0) for surgical procedures. Surgical margins are judged using the 1 mm principle of R0/R1 resection criteria, i.e., distance from the margin 1mm from the margin for R0 resection, otherwise R1 resection for R1 excision. Before treating the patient, the necessary imaging and assessment of the systemic condition should be completed, and a multidisciplinary consultation should include diagnostic imaging, pathology, chemotherapy, and radiotherapy.
The assessment of tumor status prior to surgical treatment is clinically important. The tumor is classified as resectable, potentially resectable, or unresectable on the basis of imaging findings before surgery, and specific treatment plans are developed. The determination is based on the presence of distant metastases, invasion of the superior mesenteric vein or portal vein, and the presence of tumors in the fatty spaces around the celiac trunk, hepatic artery, and superior mesenteric artery, as detailed in Appendix 9. Standard surgical treatment is the best way to obtain a good prognosis and should be guided by the following principles.
- Tumor-free principle: including the principle of tumor non-contact, the principle of whole tumor resection and the blockage of tumor supplying vessels.
-
Adequate scope of resection: ①Standard pancreaticoduodenectomy: The scope of pancreatic The extent of duodenectomy includes 1/3toof the distal stomach family:Times New Roman”>1/2, the full length of the common bile duct and the cut edge of the gallbladder and head of the pancreas on the left side of the superior mesenteric vein/3 cm from the tumor, all of the duodenum, the proximal segment 15 cm of the jejunum; the fascia anterior to the pancreas and the soft tissue posterior to the pancreas were fully resected. Tissue in the region of the hooked eminence with local lymphatic reflux, the nerve plexus in the region. The loose connective tissue around large blood vessels, etc. ②Standard distal pancreatectomy: the scope includes the caudal part of the body of the pancreas, spleen and splenic artery, lymphatic clearance, may include the left renal fascia, may include part of the colonic mesentery, but does not include colonic resection. (3) Standard total pancreatectomy: the scope includes the head, neck and tail of the pancreas, duodenum and first jejunum, gallbladder and common bile duct, spleen and splenic artery, lymphatic clearance, may include the gastric sinus and pylorus, may include the renal fascia, may include part of the colonic mesentery, but does not include colectomy.
-
Safe margins: pancreatic duodenal resection for pancreatic head cancer requires attention 6 incisional margins, including the pancreas (pancreatic neck), common bile duct (common hepatic duct), stomach, duodenum, retroperitoneum (which refers to skeletal clearance of the superior mesenteric artery), other soft tissue margins (such as posterior pancreatic The margins of the pancreas should be larger than 1mm(no tumor remains microscopically), and the margins of the pancreas can be frozen during surgery to ensure adequate Pathological examination.
- style=”margin-left: 72pt”>
-
Lymph node Lymph node dissection: With the standard lymph node dissection range, one should obtain
-
15 or more lymph nodes. Number of lymph nodes acquired in patients after neoadjuvant therapy
can be less than 15 . Whether to perform an expanded lymph node dissection is still controversial, as
This is not recommended for routine extended retroperitoneal lymph node dissection. The extent of lymph node dissection that should be performed in standard radical pancreatic cancer surgery is as follows.
1) Standard lymph node dissection for pancreaticoduodenectomy for pancreatic head cancer: Suprapyloric and inferior lymph nodes (No.5, No.6), anterior lymph nodes of the common hepatic artery (No.8a), lymph nodes of the hepatoduodenal ligament (common hepatic duct, common bile duct and gallbladder lymph nodes, No.12b1, 12b2, 12c), dorsal superior and inferior marginal lymph nodes of the pancreatic duodenum
(No.13a, 13b), lymph nodes on the right side of the superior mesenteric artery (No.14a,14b), lymph nodes on the ventral superior and inferior margins of the pancreaticoduodenum (No.17a,17b).
②Lymphatic clearance for standard pancreatic body tail cancer resection: splenic hilar lymph nodes
(No.10), peri-splenic artery lymph nodes (No.11) Roman”>No.11), lymph nodes at the lower margin of the pancreas
(No.18), and the above lymph nodes were excised in whole with the specimen. For lesions located in the body of the pancreas, the peri-abdominal trunk lymph nodes (No.9) plus part of the superior mesenteric artery (No.14) can be cleared. span>)+ periaortic lymph nodes (No.16).
- style=”margin-left: 57pt”>
- Preoperative yellowing reduction
-
The main purpose of preoperative yellowing reduction is to relieve biliary obstruction, reduce symptoms such as cholangitis, and at the same time improve liver function, correct coagulation abnormalities, and reduce surgical mortality. However, preoperative routine biliary drainage is not recommended.
-
Preoperative reduction of yellowing is feasible in patients with severe symptoms, fever, sepsis, and septic cholangitis.
- style=”margin-left: 73pt”>
- Yellowing can be reduced by transnasal bile duct drainage or percutaneous hepatic puncture biliary drainage
(percutaneous transhepatic cholangiodrainage, PTCD) is completed, and choledochostomy is feasible in hospitals without it.
- style=”margin-left: 72pt”>
- Usually done in decolonization . family:Times New Roman”>2 weeks later, the bilirubin decreases to the initial value of one
- Yellowing can be reduced by transnasal bile duct drainage or percutaneous hepatic puncture biliary drainage
The procedure can be performed when the liver function recovers and the body temperature and blood picture are normal.
- style=”margin-left: 57pt”>
- Indications for radical surgical resection
-
Age<80 years, good general condition, multidisciplinary assessment of heart//years =”font-family:Arial”>lung/liver/ Renal function can tolerate the procedure.
- style=”margin-left: 72pt”>
- The clinical staging isStage II pancreatic cancer below.
- No liver metastasis and no ascites.
- The clinical staging isStage II pancreatic cancer below.
-
The intraoperative exploration of the mass was confined to the pancreas and did not invade important vessels such as the mesenteric portal vein and superior mesenteric vein.
- style=”margin-left: 72pt”>
- No distant dissemination or metastasis.
- style=”margin-left: 44pt”>
-
Surgical Modality
- Tumor located in the head and neck of the pancreas is feasible for pancreaticoduodenectomy.
- Tumor located in the tail of the pancreatic body can be treated by pancreatic body tail plus splenectomy.
- When the tumor is large and the scope includes the head, neck and body of the pancreas, total pancreatectomy is feasible.
- Tumor located in the head and neck of the pancreas is feasible for pancreaticoduodenectomy.
- No distant dissemination or metastasis.
Operation.
- style=”margin-left: 85pt”>
- Minimally invasive radical pancreatic cancer radical surgery has been shown to be safe in surgery, lymph node clearance
Number of sweeps and R0 resection rates are comparable to open surgery, but its “oncological “benefit to be confirmed by further clinical studies and is recommended to be performed by experienced pancreatic surgeons in a large specialized pancreatic center.
- style=”margin-left: 57pt”>
- Stump anastomosis after pancreatic resection
The purpose of post-pancreatic resection stump management is to prevent pancreatic leakage, and pancreatic-enteric anastomosis is the commonly used anastomosis. There are various anastomoses for pancreatic-enteric anastomosis, and the appropriate anastomosis should be selected to reduce the occurrence of pancreatic leakage.
- style=”margin-left: 57pt”>
- Perioperative medication management. Patients undergoing major open heart surgery, regardless of their nutritional status
status, immunonutrition is recommended before surgery regardless of their nutritional status 5 to 7 days and continue until 7 days after surgery or until the patient consumes >60% of the required amount by mouth. Immune-enhanced enteral nutrition should contain both ω-3 polyunsaturated fatty acids, arginine, and nucleotide 3 class substrates. Adding any of the above 3 classes of nutrients alone or 1 or 2 species, the role of which requires further study. Oral enteral nutrition support is preferred.
Patients with moderate malnutrition planning major surgery or patients with severe malnutrition are recommended to receive nutritional therapy for 1 to 2 weeks before surgery, even if the surgery is delayed. Patients who are expected to be unable to meet their nutritional needs through a normal diet for more than 7 days after surgery, as well as those who cannot meet 60% of their 1 week, should be given postoperative nutritional therapy.
- style=”margin-left: 57pt”>
-
Management of complications and principles of management
- Postoperative bleeding: postoperative bleeding after surgery 24 hours or less for acute
- Postoperative bleeding: postoperative bleeding after surgery 24 hours or less for acute
bleeding and more than 24 hours for delayed bleeding. This includes mainly abdominal bleeding and gastrointestinal bleeding. The ISGPS established a clinical staging system for postoperative bleeding, which divides postoperative bleeding into A phase, Phase B and Phase C . See Appendix 14.
1) Abdominal bleeding: mainly due to incomplete intraoperative hemostasis, the illusion of bleeding cessation in the intraoperative hypotensive state, or dislodged ligature wires or dislodged electrocoagulation scabs; impaired coagulation mechanisms are also a cause of intraoperative bleeding. The main methods of prevention are close hemostasis during surgery, careful examination before closing the abdomen, important vascular sutures, and preoperative correction of coagulation function. In the event of abdominal bleeding, great attention should be paid to the small amount of bleeding that can be treated conservatively with medication and blood transfusions; in the event of large blood loss in a short period of time, resulting in hemorrhagic shock, surgical hemostasis should be performed as soon as possible.
②Gastrointestinal bleeding: Stress ulcer bleeding, mostly occurring 3 days after surgery
or more. Its prevention and treatment is mainly to correct the patient’s nutritional status before surgery, to minimize the blow of surgery and anesthesia, to treat mainly conservatively, to apply hemostatic drugs, growth inhibitors, proton pump inhibitors, etc., to indwelling gastrointestinal decompression device, to inject 8mg/dl via gastric tube Ice noradrenaline saline, also gastroscopic hemostasis, angiographic embolization. If conservative treatment is ineffective, surgical treatment is indicated.
-
Pancreatic fistula: according to 2016 Edition ISGPS criteria, the diagnosis of pancreatic fistula requires that the amylase value in the drainage fluid on the third postoperative day or later reaches the upper limit of normal 3 fold, while producing certain clinical effects that require aggressive clinical treatment. The original 2005 version of A grade pancreatic fistula is changed to a biochemical fistula, not a postoperative pancreatic fistula, independent of the clinical course. B Grade B fistula diagnosis needs to be clinically relevant and affect the postoperative course, including: continuous drainage 3 weeks or more; a clinically relevant change in pancreatic fistula treatment measures; the use of percutaneous or endoscopic puncture drainage; the use of angiographic interventions for bleeding; and the development of signs of infection other than organ failure. Once single or multiple organ dysfunction has occurred, including due to pancreatic fistula infection, the pancreatic fistula classification is adjusted from B to Grade span style=”font-family:Times New Roman”>Class C . The management of pancreatic fistula includes appropriate fasting, effective and adequate drainage, infection control, nutritional support, acid and enzyme suppression, etc. If abdominal bleeding occurs, interventional embolization can be considered to stop the bleeding. Surgical treatment is mainly suitable for patients with pancreatic fistula who have poor drainage, severe abdominal infection or hemorrhage.
- style=”margin-left: 72pt”>
- Gastric emptying disorder
1) There is no unified criterion for gastric emptying disorder, and the commonly used diagnostic criteria are no obstruction of the gastric outflow tract confirmed by examination; gastric fluid > 800 ml/d over 10 days; no significant water-electrolyte and acid-base balance abnormalities; no underlying disease causing gastroparesis; and no drugs affecting smooth muscle contraction.
- Gastric emptying disorder
② Diagnosis is mainly based on history, symptoms, signs, gastrointestinal imaging, gastroscopy, etc.
③The treatment of gastric emptying disorder is mainly based on adequate gastrointestinal decompression, enhanced nutritional psychotherapy or psychological suggestion therapy; application of gastrointestinal motility drugs; treatment of underlying disorders and disorders of nutritional metabolism. Traditional Chinese medicine treatment has good effect on promoting the recovery of gastrointestinal function and shortening the recovery time of gastric emptying.
-
Other complications include abdominal infection, biliary fistula, celiac leakage, and long-term postoperative complications.
- style=”margin-left: 44pt”>
- Surgical treatment for those whose tumors may be resected
Patients with potentially resectable tumors have low access to R0 resection rates, and the optimal treatment strategy has been controversial. A neoadjuvant-first treatment model is currently advocated, in which patients with potential benefit are considered for neoadjuvant treatment (chemotherapy, or radiotherapy, or induction chemotherapy followed by concurrent radiotherapy, etc.) in a multidisciplinary discussion, evaluated to achieve tumor downstaging, and then treated with surgery. For patients with sequential tumor resection after neoadjuvant therapy, combined venous resection that achieves R0 radicalization is associated with a comparable survival benefit to resectable patients. The improvement in patient prognosis with combined atherectomy is controversial and needs to be evaluated in a prospective large sample of data. Given the lack of sufficient high-level evidence-based medical evidence, participation in clinical studies is recommended for patients with borderline resectable pancreatic cancer. Surgical exploration can also be performed directly if requested by the patient. Palliative R2 resection is not recommended in this group of patients, except in special circumstances such as life-saving hemostasis.
- style=”margin-left: 40pt”>
- Surgical treatment of locally advanced unresectable pancreatic cancer
For this group of patients, aggressive treatment is still possible to achieve a better outcome. In patients with tentative duodenal obstruction but expected survival ≥3 months.
- Surgical treatment for those whose tumors may be resected
Patients with clinical indications for prophylactic gastrojejunostomy; patients with unresectable tumors but combined biliary obstruction, or those who are expected to have possible biliary obstruction, may be considered for choledochal < span style="font-family:Times New Roman">/ common hepatic duct jejunostomy; patients with duodenal obstruction who have an expected survival ≥3 months, gastrojejunostomy is feasible. Intraoperative local treatment of the tumor can be performed by intraoperative radiotherapy and irreversible electroporation therapy (nano-knife ablation) to achieve increased local control rate and pain relief. Postoperative combination chemotherapy ± radiotherapy is required
(iii) Internal medicine treatment.
Medical treatment of pancreatic cancer can be applied to patients at all stages, including preoperative neoadjuvant/conversion therapy for resectable and critically resectable patients, adjuvant therapy for post-radical patients, and treatment for patients with locally advanced or metastatic recurrence. Internal drug therapy not only prolongs survival, but also reduces pain and improves quality of life in patients with advanced disease. Timely medication and dose adjustments are made according to the patient’s condition and physical status score. Emphasis is placed on improving patients’ quality of life and comorbidity management, including pain, nutrition, and psychosomatic. Genetic testing for locally advanced and metastatic pancreatic cancer, including but not limited to BRCA1/2, NTRK1/2/3, PALB2, ATM/ATR and RAS, is recommended prior to medical drug therapy to help guide the optimal drug regimen and participate in clinical studies of new drugs. For patients with advanced metastatic pancreatic cancer who have failed standard therapy, high-throughput sequencing at a qualified genetic testing facility may be considered to find appropriate clinical studies or drug therapies to participate in.
- style=”margin-left: 61pt”>
- Neoadjuvant/translational therapy for resectable or critically resectable pancreatic cancer
The goal of neoadjuvant/transformation therapy for patients with resectable or critically resectable pancreatic cancer is to improve surgical R0 resection rates and thereby prolong patient disease-free and overall survival.
However, there is a lack of evidence from high-level clinical studies, and relevant clinical studies are recommended. For resectable pancreatic cancer in good physical status with high-risk factors (e.g.
High serum CA19-9 levels, large primary pancreatic tumors, extensive lymph node metastases, severe wasting, and extreme pain) and Preoperative neoadjuvant/conversion therapy can be considered for patients with borderline resectable pancreatic cancer. Patients who undergo radical surgery 4-8 weeks after preoperative chemotherapy and have no evidence of recurrence or metastasis after surgery are recommended to continue adjuvant chemotherapy after multidisciplinary evaluation, with the regimen taking into account the efficacy of neoadjuvant chemotherapy or other clinical factors such as the patient’s general condition and tolerance of chemotherapy. A two-drug combination based on gemcitabine or a three-drug combination with mFOLFIRINOX is recommended. See Table 2 for details of commonly used regimens.
For patients in poor physical status who cannot tolerate surgical treatment, a puncture biopsy is recommended to clarify the pathology, followed by late palliative chemotherapy and optimal supportive care.
Table 2 Neoadjuvant/translational treatment options for resectable or critically resectable pancreatic cancer
Program |
Specific medications |
Gemcitabine + albumin binding |
Albumin-bound paclitaxel 125mg/m2 Intravenous drip No. |
|
type paclitaxel |
1, 8 |
|
Gemcitabine 1000mg/m2 IV doses on days 1 and 8 |
|
|
Repeat every 3 weeks |
FOLFIRINOX (only for
Patients with ECOG PS score 0 to 1)
Oxaliplatin 85mg/m2 IV Irinotecan 180mg/m on day 12 IV drip Day 1 Calcium folinic acid 400mg/m2 IV drip Day 1
5- fluorouracil (5- fluorouracil (5-FU) 400mg/m2Rapid IV Day 1
After 5-FU 2400mg/m2 Continuous infusion for 46 hours
Repeated every 2 weeks
mFOLFIRINOX (only for patients with ECOG PS score 0 to 1)< /p>
< span style="font-family:仿宋">Oxaliplatin 85mg/m2IV drip Day 1 irinotecan 150mg/m2 IV drip Day 1 calcium folinic acid 400mg/m2 IV drip Day 1 5-FU 2400mg/m2 2 Continuous infusion 46 hours
Repeat every 2 weeks
- style=”margin-left: 61pt”>
- Postoperative adjuvant therapy for resectable pancreatic cancer
Patients with pancreatic cancer after radical surgery should undergo adjuvant chemotherapy if there is no contraindication. Adjuvant chemotherapy regimens based on gemcitabine or fluorouracil-based agents (5-FU, capecitabine, or tegeo) are recommended; in patients with good physical status, combination chemotherapy, including gemcitabine + capecitabine, mFOLFIRINOX, etc., is recommended. Patients in poorer physical status are recommended to be given gemcitabine or fluorouracil-based monotherapy with optimal supportive therapy. Adjuvant chemotherapy should be initiated within 12 weeks of surgery and continued for 6 months if possible.
Table 3 Postoperative adjuvant adjuvant treatment options for resectable pancreatic cancer treatment options for resectable pancreatic cancer
Program |
Specific medications |
|
mFOLFIRINOX (only for patients with ECOG PS score 0 to 1)< /p> |
Oxaliplatin 85mg/m2 IV Irinotecan 150mg/m on day 12 IV drip Day 1 Calcium folinic acid 400mg/m2 IV drip Day 1 After 5-FU 2400mg/m2 Continuous infusionContinuous infusion 46 hours Repeated every 2 weeks |
|
Gemcitabine + Capecitabine |
Gemcitabine 1000mg/m2IV Capecitabine 1660mg/(m2 on days 1 and 82 -(d) in 2 oral doses Days 1 to 14 Repeat every 3 weeks |
Gemcitabine |
Gicitabine |
|
Tigeo |
Tegeo 80-120mg/d in 2 oral doses Day 1-14 Repeat every 3 weeks |
Capecitabine |
Capecitabine 2000mg/(m2-d) in 2 oral doses Days 1-14 Repeat every 3 weeks |
5-FU/calcium folinate (leucovorin, LV) |
LV 400mg/m2 IV drip Day 1 5-FU 400mg/m2 IV drip Day 1 After 5-FU 2400mg/m2 Continuous infusion for 46 hours |
- style=”margin-left: 61pt”>
- Unresectable locally advanced or metastatic pancreatic cancer
The overall treatment of unresectable locally advanced or combined distant metastatic pancreatic cancer is not effective, and clinical studies are recommended. Currently, the commonly used chemotherapeutic agents for unresectable locally advanced or metastatic pancreatic cancer include gemcitabine, albumin-bound paclitaxel, 5-FU/LV, cisplatin, oxaliplatin, irinotecan, tegeo, and capecitabine. Targeted agents include erlotinib.
First-line chemotherapy regimens were selected based on the patient’s fitness status (see Table 4). Combination chemotherapy is recommended for patients in good general condition. For patients with ECOG PS score 0 to 1, the three-drug combination FOLFIRINOX or mFOLFIRINOX regimen can be considered. For patients with advanced pancreatic cancer with BRCA1/2 germline mutations who may be sensitive to platinum drugs, a regimen containing cisplatin or oxaliplatin (GP or FOLFIRINOX, mFOLFIRINOX) may be considered as the first choice. Other regimens include FOLFOX (oxaliplatin/5-FU/LV), CapeOx (oxaliplatin/capecitabine), and FOLFIRI (irinotecan/5-FU/LV) are often used as second-line treatment options.
Follow-up strategies for patients with effective combination chemotherapy include continuing treatment with the previously effective regimen, stopping treatment altogether, withdrawing the more toxic drugs from the previous combination regimen, withdrawal of the more toxic drug from the previous combination regimen, or switching to a new drug for maintenance therapy. For patients with
Patients with BRCA1/2 germline mutations who have not progressed after ≥16 weeks of first-line treatment with a platinum-containing regimen are treated with polyglandular therapy. Patients who have progressed are treated with maintenance therapy with the polyadenosine diphosphate ribose polymerase inhibitor olaparib monotherapy. Patients with systemic BRCA1/2 gene mutations or other abnormalities in the homologous recombination repair pathway may be treated equally with reference to germline mutations. If GN regimen was previously used, gemcitabine monotherapy may be used for maintenance; if (m)FOLFIRINOX regimen was previously used, capecitabine or 5-FU/LV, or FOLFIRI regimen may be considered for maintenance (oxaliplatin maintenance is not recommended due to cumulative neurotoxicity of oxaliplatin).
Patients who have failed first-line therapy may choose nanoliposomal irinotecan + 5-Fu/LV if they are in good health, or they may choose non-overlapping drugs as second-line based on drugs already used in first-line, patient comorbidities and toxicities The patient may choose non-overlapping drugs as second-line chemotherapy or participate in clinical studies. For advanced pancreatic cancer with specific genetic variants (e.g. NTRK fusion, ALK gene rearrangement, HER2 amplification, high microsatellite instability), studies have shown the efficacy of their corresponding targeted therapy or immune checkpoint inhibitor therapy. The first recommendation is to enroll these patients in their corresponding clinical studies, or to consider targeted therapy or immunotherapy with specific targets under the guidance of an experienced medical oncologist.
If the physical status is poor, monotherapy or/and best supportive care is recommended. The continuation of chemotherapy for pancreatic cancer patients after failure of first- or second-line chemotherapy regimens is controversial, and no definitive chemotherapy regimen is available. The WHO criteria for evaluating the efficacy of solid tumors and the RECIST criteria can be used for post-chemotherapy evaluation, as described in Annex 10 and Annex 11.
Table 4 Treatment options for unresectable locally advanced or metastatic pancreatic cancer
The more physically fit |
|
Program |
Specific medications |
|
GN: Gemcitabine + albumin-bound paclitaxel |
Albumin-bound paclitaxel 125mg/m2 IV Gemcitabine 1000mg/m2 IV drip days 1 and 8 Repeat every 3 weeks |
|
GP: Gemcitabine + cisplatin (especially for patients with hereditary tumors that may have BRCA1/2 or other DNA repair gene mutations) |
Gemcitabine 1000mg/m2 Intravenous drip day 1, 8 Cisplatin 75mg/m2 Intravenous drip day 1 Day 1 Repeat every 3 weeks |
|
FOLFIRINOX (for ECOG only |
Oxaliplatin 85mg/m 2 IV drip Day 1 |
|
PS score 0 to 1 for patients) |
Iritecan 180mg/m2 IV drip Day 1 |
|
LV400mg/m2 IV drip Day 1 |
|
|
5-FU 400mg/m2 Rapid IV Day 1 |
|
|
Repeat every 2 weeks |
|
|
mFOLFIRINOX (for ECOG only |
Oxaliplatin 85mg/m 2 IV drip Day 1 |
|
PS score 0 to 1 for patients) |
Iritecan 150mg/m2IV drip Day 1 |
|
Calcium folinic acid 400mg/m2 IV drip day 1 |
|
|
After 5-FU 2400mg/m2 continuous infusion for 46 hours |
|
|
Repeat every 2 weeks |
|
Gicitabine + Erlotinib
Gemcitabine 1000mg/m2 IV drip, day l and 8 Erlotinib 150mg/day Oral
Repeat every 3 weeks
GX: gemcitabine + capecitabine
Gemcitabine 1000mg/m2 Intravenous drip Day 1, 8
Capecitabine 1660mg/(m2-d) in 2 oral doses Days 1 to 14
Repeat every 3 weeks
GS: Gemcitabine + Tegeo
Gemcitabine 1000mg/m2 Intravenous drip Day 1, 8
Tegeo 80-120mg/d in 2 oral doses Repeat every 3 weeks on days 1-14
Gemcitabine
Gicitabine
=”font-size:12pt”>Gemcitabine 1000mg/m2 IV drip Repeat every 3 weeks on days 1 and 8
Tigeo
Tegeo 80-120mg/d in 2 oral doses Repeat every 3 weeks on days 1-14
Olaparib maintenance therapy (for BRCA1/2 germline mutations with good PS scores, first-line platinum-containing regimen)
No disease progression at ≥ 16 weeks
Patients with progressive disease at ≥ 16 weeks
Olaparib 300mg orally twice daily
CapeOx: oxaliplatin + capecitabine
Oxaliplatin 130mg/m2IV drip Day 1
Capecitabine 2000mg/(m2-d) in 2 oral doses 1st to 14th
day
Repeat every 3 weeks
5-FU/LV
LV 400mg/m2 intravenous drip Day 1
5-FU 400mg/m2 IV drip Day 1
After that 5-FU 2400mg/m2 continuous infusion 46 hours repeated every 2 weeks
Nanoliposomal irinotecan
+5-FU/LV
Nanoliposomal irinotecan 80mg/m2 IV drip Day 1 LV 400mg/m2, IV drip Day 1
5-FU 2400mg/m2, continuous infusion for 46 hours
Repeat every 2 weeks
FOLFIRI
Irinotecan 180mg/m2 IV day 1 LV 400mg/m2, IV day 1
5-FU 400mg/m2, intravenous drip day 1
Then 5-FU 2400mg/m2, continuous infusion over 46 hours repeated every 2 weeks Pablizumab (only for patients with high microsatellite instability or mismatch repair defects)
Pabrolizumab 200mg intravenous drip Day 1 repeated every 3 weeks
(iv) Radiation therapy.
Radiation therapy is one of the important local treatments for pancreatic cancer and is used throughout all stages. For patients with surgically resectable limited pancreatic cancer who are intolerant to surgery or refuse surgery due to medical disease, precise radical radiation therapy combined with concurrent chemotherapy for sensitization is recommended as a new option to improve the long-term survival of these patients. Patients with critical surgically resectable disease
Patients can receive direct high-dose radiotherapy or combined chemotherapy and decide whether to undergo surgical resection based on the efficacy of the treatment. Concurrent radiotherapy is the treatment of choice for locally advanced pancreatic cancer. For pancreatic cancer patients with few metastases (limited number of metastases and organs), simultaneous irradiation of the primary site and metastases can be used to relieve obstruction, compression or pain and improve local control of the tumor. The role of postoperative radiotherapy for pancreatic cancer is still controversial. For patients with postoperative pancreatic cancer with local residual or unclear cut margins, simultaneous postoperative radiotherapy can compensate for the lack of surgery. Intensity-modulated radiotherapy techniques and stereotactic radiotherapy based on multibeam (X-ray or gamma-ray) focusing
(The dose pattern of radiotherapy is gradually changing towards high dose and less fractionation (large fractionated radiotherapy), and the local control rate, pain relief rate and survival rate have been improved and enhanced, but further confirmation in large phase III clinical trials is still needed.
Indications for radiotherapy for pancreatic cancer
- style=”margin-left: 85pt”>
- Surgically resectable pancreatic cancer
For surgically resectable limited stage pancreatic cancer that refuses surgical treatment or is medically intolerant to surgical treatment, it is recommended to receive high-dose less fractionated or SBRT radiotherapy in combination with neoadjuvant or concurrent radiotherapy. There is no clear standard for the total dose and fractionated dose of SBRT, and the currently recommended fractionated dose is 5 times per SBRT. span style=”font-family:Times New Roman”>25 to 45 Gy or every 5 sessions 33 to 40 Gy per 6.6 to 8.0 Gy.
- style=”margin-left: 85pt”>
- Critically resectable pancreatic cancer
There is no standard model for radiation therapy for borderline resectable pancreatic cancer. High-dose fractionated radiotherapy or SBRT can be administered directly to the tumor area, and radiotherapy followed by surgery to improve R0 resection rate. It is beneficial to improve patient survival. Neoadjuvant radiotherapy
Total radiotherapy dose is 45 at the time of therapy. ~50.4 Gy at 1.8~ 2.0 Gy at 5 weekly exposures, or a total dose of 36 Gy at 2.4 Gy at 5 weekly exposures can be used.
Irradiation. For surgically resectable cases, surgery is recommended around 4 weeks after neoadjuvant radiotherapy or chemotherapy, while for critically resectable cases, the best time to operate is 4 to 8 weeks after neoadjuvant radiotherapy or chemotherapy to allow sufficient time for the tumor to shrink sufficiently before surgery. It is also possible to undergo surgery beyond 8 weeks, but fibrosis from radiation therapy can make surgery more difficult.
- style=”margin-left: 85pt”>
- Low stage pancreatic cancer
For locally advanced pancreatic cancer, high-dose fractionated intensity-modulated radiation therapy or SBRT in combination with neoadjuvant or concurrent radiotherapy or chemotherapy. This can have a better prognosis compared to conventional radiotherapy modalities.
- style=”margin-left: 85pt”>
- Oligometastatic pancreatic cancer
Patients with metastatic pancreatic cancer who are well treated with systemic systemic therapy or who have a relatively slow rate of progression receive high-dose radiotherapy for both primary and metastatic sites, and the rate of local control translates into prolonged survival time.
- style=”margin-left: 85pt”>
- Recurrent pancreatic cancer
Patients with recurrent pancreatic cancer after surgery or other local treatments such as radiofrequency therapy are at higher risk for radiotherapy than primary patients because of the adverse gastrointestinal diversion for visualization and previous treatment damage.
- style=”margin-left: 85pt”>
- Postoperative adjuvant radiotherapy
Postoperative adjuvant radiotherapy is controversial and lacks high-level evidence-based medical rationale. The use of conventional radiotherapy modalities in combination with chemotherapy may improve the local recurrence rate of tumors compared to chemotherapy alone. The total dose of radiotherapy was 45~50.4 Gy , fractionated dose 1.8~2 Gy per dose, with an additional 52 Gy for sites with high risk of recurrence family:Times New Roman”>~9 Gy.
- style=”margin-left: 57pt”>
- Radiotherapy Techniques
SBRT and IMRT including volumetric rotational intensity modulated radiotherapy and spiral tomography intensity modulated radiotherapy, have better dose distribution conformality and focus than 3D conformal radiotherapy, and can increase the dose of pancreatic tumor irradiation without increasing the dose to normal tissues when combined with the synchronous dose of target-in-target or target-in-zone radiation therapy. In the case of pancreatic cancer, it is important to refine all aspects of radiotherapy to improve the accuracy of the target area outline and to reduce positional errors and interference from respiratory motion.
- style=”margin-left: 57pt”>
- Radiotherapy target area
For non-surgically resected lesions, irradiation of primary or recurrent pancreatic lesions and metastatic lymph nodes, excluding regional lymph node drainage areas, is recommended.
The target area volume for postoperative radiotherapy should be determined based on preoperative CT scan results or surgically placed silver clips and should include the primary tumor bed and regional high-risk lymph node areas.
- style=”margin-left: 57pt”>
- Radiotherapy dose
Increasing the dose of radiotherapy is one of the key factors to improve the local control rate of pancreatic cancer, and the dose pattern to be used is determined by the equipment technology, the optional range is 40 to 70Gy/5 to 20 times, the higher the biologically effective dose, the higher the local control rate, provided that ensure avoidance or reduction of gastrointestinal radiation damage occurrence. The total conventional dose pattern is 45 to 54Gy, with a single dose of 1.8 to 2.0Gy.
- style=”margin-left: 57pt”>
- Concurrent chemotherapy
Concomitant chemotherapy regimens with gemcitabine or fluorouracil are preferred as single agents.
(5-FU continuous intravenous infusion, or capecitabine, or S-1), or give multi
drug in combination with gemcitabine or a fluorouracil-based regimen.
- style=”margin-left: 57pt”>
- Intraoperative radiotherapy
Intraoperative radiotherapy is usually planned or used when the tumor is found to be unresectable during the exploratory dissection, when the tumor margin is close or when the margin is positive during surgery. Intraoperative electron beam irradiation radiotherapy is recommended for 15 to 20Gy, postoperatively (within 1 month, supplemented with external irradiation 30Gy/10f or 40Gy/10f or 40Gy/10f. Roman”>40Gy/20f.
(v) ERCP and related treatments.
Solely diagnostic ERCP operations are no longer recommended as the first choice for the diagnosis of pancreaticobiliary system diseases, but more is to perform diagnostic cholangiography during therapeutic ERCP operations. A flow chart of the role of pancreatic cancer ERCP diagnosis is shown in Appendix 12.
- style=”margin-left: 57pt”>
-
ERCP for preoperative yellowing reduction in pancreatic cancer
Cholestasis caused by compression of bile duct strictures by pancreatic cancer theoretically increases the complication rate after surgical treatment, leading to high postoperative mortality and disability rates. Preoperative drainage can also improve the synthetic function of the liver, improve the clearance of endogenous toxins and improve the function of the mucosa of the digestive tract, thus contributing to the smooth operation. In contrast, preoperative reduction of jaundice in pancreatic cancer patients with indications for surgery needs to be carefully considered, and the results of a randomized controlled trial have shown that within the range of surgically acceptable jaundice
(≤250 μmol/l), patients who underwent direct surgery had better postoperative outcomes than those who underwent preoperative biliary The postoperative outcome is better in patients with direct surgery than in patients with preoperative application of biliary stents for anterior reduction of yellowing. Therefore, the selection of the indications for preoperative drainage for yellowing reduction should be strictly controlled, and the indications for preoperative yellowing reduction are as follows.
-
Patients with fever, sepsis, and significant cholangitis who require preoperative improvement of symptoms.
- style=”margin-left: 72pt”>
- Patients with severe symptoms, pruritus and purulent cholangitis.
- Patients with severe symptoms, pruritus and purulent cholangitis.
- style=”margin-left: 85pt”>
- Patients with various reasons for delayed surgery.
- Patients who need preoperative radiotherapy or chemotherapy.
Reduction of yellowing is possible with nasobiliary drains (ENBD) or removable bile duct stents, avoiding the use of non-removable bare metal stents.
- style=”margin-left: 57pt”>
- ERCPin the treatment of pancreatic cancer without surgical indications
More than 80% of pancreatic cancer patients cannot be treated with radical surgery at the time of initial diagnosis because of progressive local invasion or distant metastases, so palliative care for pancreatic cancer patients is particularly important. Therefore, palliative care for pancreatic cancer patients is particularly important, with the goal of relieving symptoms and improving quality of life. Patients with advanced pancreatic cancer 70% to 80% will have bile duct obstruction, and the main objective of palliative care for advanced pancreatic cancer is Bile duct decompression. Compared to PTCD, endoscopic bile duct drainage has a greater chance of successful placement and more accurate stent positioning, less risk of bleeding and bile leakage, and a higher overall complication rate than PTCD. “font-family:Times New Roman”>PTCD is lower. In general, ERCP is recommended as the preferred method for palliative bile duct drainage, only when ERCP is not available, the The use of PTCD was considered only when ERCP was not available, failed, or when endoscopic treatment was not effective. Based on efficacy and cost-effectiveness analysis, plastic bile duct stenting is recommended for patients with an expected survival <3 months, whereas for patients with an expected survival ≥3 months Roman”>≥3 months, a metal biliary stent should be implanted and a nasobiliary drainage tube should be used to reduce pressure and drainage if necessary before stenting.
(vi) Interventional therapy.
Interventional treatment of pancreatic cancer includes: interventional treatment of pancreatic cancer and pancreatic cancer metastases and treatment of complications related to pancreatic cancer, including transarterial infusion chemotherapy, ablation therapy, PTCD, biliary stenting, gastrointestinal stenting, bleeding embolization, abdominal plexus block for cancer pain (celiac
plexus neurolysis, CPN). 1. Principles of interventional therapy
-
Must have digital subtraction angiography machine,CT/MR, ultrasound and other image-guided equipment, strictly grasp clinical indications and contraindications, and emphasize standardized and individualized treatment.
- style=”margin-left: 72pt”>
- Interventional treatment is mainly applied to the following cases
① Locally advanced pancreatic cancer that cannot be surgically resected as assessed by imaging.
②Pancreatic cancer that has been lost to surgery for other reasons.
③Infusion chemotherapy as a special form of neoadjuvant chemotherapy for pancreatic cancer.
④Postoperative prophylactic infusion chemotherapy or adjuvant chemotherapy.
5 Pancreatic cancer with liver metastases.
⑥Treatment of pancreatic cancer-related complications such as control of pain, bleeding, gastrointestinal obstruction and obstructive jaundice.
- style=”margin-left: 44pt”>
- Transcatheter arterial infusion chemotherapy
- Interventional treatment is mainly applied to the following cases
-
Infusion chemotherapy for pancreatic cancer: place catheters selectively in the celiac artery, mesenteric artery, and superior mesenteric artery, respectively. If the tumor-supplying vessels are clearly visible, carefully analyze the imaging performance to clarify the site, size, number and blood-supplying arteries of the tumor, and super-select to the tumor-supplying arteries for perfusion chemotherapy; if the tumor-supplying arteries are not visible, the target vessels should be determined according to the tumor site, invasion range and blood supply as shown by imaging. In principle, tumors in the head and neck of the pancreas are treated by perfusion chemotherapy via the gastroduodenal artery; tumors in the body and tail of the pancreas are mostly treated by perfusion chemotherapy via the celiac artery, superior mesenteric artery or splenic artery.
- style=”margin-left: 72pt”>
- Infusion embolization chemotherapy for liver metastasis of pancreatic cancer: if the patient also has liver
- Infusion embolization chemotherapy for liver metastasis of pancreatic cancer: if the patient also has liver
liver metastases, then concurrent hepatic artery perfusion chemotherapy and/or embolization is required.
-
Primary perfusion chemotherapy is used: commonly used drugs include gemcitabine, fluorouracil, adriamycin (epi-adriamycin), platinum drugs (cisplatin and the new chemotherapy drug lopressor) These drugs are used as single agents or in combination. The drug dose is determined by patient-specific parameters such as body surface area, liver/renal function, and blood count.
- style=”margin-left: 44pt”>
- Ablation therapy
The operating physician must undergo rigorous training and sufficient practice. Before treatment, the patient’s general condition, the tumor situation (size, location, number, etc.), and the relationship between the tumor and the surrounding adjacent organs should be fully evaluated, and the appropriate puncture path and ablation range should be formulated. The choice of appropriate imaging-guided techniques (ultrasound, CT or MRI) and ablative means (e.g. irreversible electroporation treatment).
Ablation should aim to include at least 5 mm of paracancerous tissue to completely kill the tumor. For some tumors with unclear borders and irregular shapes, it is recommended to extend the ablation area appropriately when the adjacent tissue and structural conditions allow.
- style=”margin-left: 44pt”>
- Interventional treatment of complications of pancreatic cancer
- Ablation therapy
-
Interventional Treatment of Jaundice: Approaching 65%~75% of patients with pancreatic cancer have symptoms of biliary obstruction, which can be treated by percutaneous transhepatic endobiliary stenting andPTCD treatment can effectively lower the patient’s bilirubin level, reduce jaundice, diminish symptoms such as pruritus, prevent other complications such as cholecystitis, and provide opportunities for surgery and chemotherapy.
-
Interventional treatment of GI obstruction. Approximately 5%~10% of pancreatic cancer patients will have symptoms of GI obstruction such as gastric outflow tract obstruction and duodenal obstruction, and GI stenting can reduce early satiety, nausea, postprandial vomiting, body
Reducing discomfort such as early satiety, nausea, postprandial vomiting, body weight reduction, and improving patients’ quality of life.
- Interventional treatment of bleeding: For patients with bleeding from the primary site of pancreatic tumor, bleeding from metastatic tumor of pancreatic cancer and post-surgical bleeding, if conservative treatment is ineffective, embolization therapy can be performed to clarify the location of bleeding through interventional angiography. The patient can be embolized by interventional angiography to identify the location of bleeding and embolize the bleeding vessel to stop the bleeding.
-
Nerve block therapy for cancer pain: Patients with pancreatic cancer causing persistent pain in the upper abdomen, who cannot tolerate the effects of oral pain medication or who cannot tolerate the adverse effects of opioid pain medication, may be considered. Patients with adverse effects may be considered for CPN. The treatment is performed on CT/MR, ultrasound/ Ultrasound endoscopy and other imaging-guided injections of drugs (anhydrous ethanol and local anesthetic drugs) into the abdominal plexus to achieve relief of abdominal pain by blocking the sympathetic pathways innervating the viscera.
(vii) Supportive therapy.
Common symptoms in patients with end-stage pancreatic cancer can be divided into 4 categories: pain, malnutrition, obstructive jaundice, tumor-associated thrombosis, etc. Optimal supportive care should be provided throughout the treatment of pancreatic cancer, especially in patients with end-stage disease, with the aim of preventing or reducing clinical symptoms and improving quality of life.
- style=”margin-left: 44pt”>
- Control of pain
Pancreatic cancer invasive pain is the primary symptom for the vast majority of pancreatic cancer patients at the time of presentation. The main causes of pain due to pancreatic cancer include: direct infiltration of the peripheral nerves by pancreatic cancer; inflammation of the peripheral nerves of the pancreas; increased pericardial tension due to pancreatic masses and increased pressure in the pancreatic duct due to pancreatic head masses. Pain management is based on analgesic medication and often requires a combination of surgery, intervention, nerve block, chemotherapy, radiotherapy, psychotherapy, and other multidisciplinary and multimodal combinations to select the best analgesic treatment.
- Control of pain
First, the cause of pain needs to be identified, and surgical management is often required for non-cancerous pain caused by emergencies such as gastrointestinal obstruction or perforation. Analgesic drug therapy follows the WHO three step analgesic drug therapy. For mild pain, non-opioid medications such as indomethacin, acetaminophen, and aspirin can be given orally; for moderate pain, weak morphine-based medications such as codeine, commonly used as amfungin and lofungin, are given daily 3 to 3. family:Times New Roman”>4 times; oral morphine should be applied promptly for severe pain. For cancer pain, the degree of pain should be clarified, and oral opioid analgesics should be administered on time and in sufficient quantity according to the patient’s pain level. Avoid only intramuscular injection of pethidine, etc. Pay attention to timely management of adverse reactions to oral pain medications such as nausea and vomiting, constipation, dizziness and headache, etc.
- style=”margin-left: 57pt”>
- Improve nutritional status
Patients with pancreatic cancer require routine nutritional screening and assessment, and if they are at nutritional risk or malnourished, they should be treated with aggressive nutritional support to prevent or delay the development of cancer cachexia. Recommended calories 25 to 30kcal/kg/ body weight per day, protein 1.2 to 2.0g/kg body weight, and adjust the nutrition supply according to the patient’s nutritional and metabolic status. For patients with complications, the caloric intake can be increased to 30 to 35kcal/kg body weight, depending on the patient’s nutritional and metabolic status. The amount of nutrients supplied is adjusted according to the patient’s nutritional and metabolic status. Commonly used nutritional support treatments include: nutrition education, enteral nutrition, and parenteral nutrition. The recommended nutritional therapy is based on the five steps of malnutrition. When patients have anorexia or dyspepsia, medications such as medroxyprogesterone or megestrol and pancreatic enzyme tablets can be used to improve appetite and promote digestion.
(H) Chinese medicine treatment of pancreatic cancer.
TCM helps to promote the recovery of body functions after pancreatic cancer surgery, reduce the toxic reactions of radiotherapy, chemotherapy and targeted drug therapy, relieve patients’ symptoms and improve patients’
Quality of life, possibly prolonging survival, can be one of the important means of pancreatic cancer treatment, either alone or in combination with other anti-tumor drugs.
China’s drug regulatory authority once approved a variety of modern Chinese medicine preparations can be used to treat pancreatic cancer, which have been widely used in clinical practice and accumulated certain practical experience, with certain efficacy and respective characteristics, and better patient compliance, safety and tolerability. However, these drugs have been on the market for many years, and early experimental and clinical studies are weak, lacking sufficient support from high-level evidence-based medical evidence, and require active, in-depth research.
In addition to these marketed proprietary Chinese medicines, the use of Chinese herbal medicine compound treatment according to the principles of Chinese medicine diagnosis and treatment is one of the most common methods in Chinese medicine, which can be individualized according to the differences of patients and has certain advantages; it can reduce tumor-related complications, improve patients’ quality of life and prolong their survival. It has certain efficacy in reducing tumor-related complications, improving patients’ quality of life, and prolonging their survival.
V. Treatment flow and follow-up
(a) The pancreatic cancer treatment process.
The general process of pancreatic cancer diagnosis and treatment is shown in Appendix 13.
The main purpose of follow-up is to detect potential metastatic recurrence that is still amenable to treatment aimed at eradication, to detect tumor recurrence or second primary cancer earlier, and to intervene in a timely manner to manage it in order to improve the overall survival and quality of life of patients. In patients with postoperative pancreatic cancer, the first 1 year after surgery, it is recommended to follow up every 3 months 1 time; in the second 2 to 3 years, every
3 to 6 monthly follow-up visits 1 time; and every 6 monthly follow-up visits 1 . follow-up visits include routine blood, biochemistry, CA19-9, CA125, CEA and other serum tumor markers, ultrasound, X ray, thin-section CT scan of the chest, and enhanced CT of the upper abdomen, etc. At follow-up
At least 5 years for patients with suspected liver metastases or bone metastases, plus liver MRI and bone scan at least every 2 to 3 monthly follow-up visits 1 . follow-up visits include routine blood, biochemistry, CA19-9, CA125, CEA and other serum tumor markers, chest CT, upper abdominal enhancement Attachment
style=”margin-left: 57pt”>








Attachment 1: Preferred roadmap for imaging pancreatic cancer before treatment


































Annex 2: Preferred roadmap for imaging follow-up after pancreatic cancer treatment










 Annex 3: Diagnostic grading of pancreaticobiliary duct cytology
Annex 3: Diagnostic grading of pancreaticobiliary duct cytology
Ⅰ Not diagnosableⅡ Not malignantIII Atypical
IVNeoplastic lesions
A A A =”font-family:仿宋”>Benign
Plasmacytoid cystadenoma
Neuroendocrine microadenoma lymphangioadenoma
BOther
Intraductal papillary mucinous neoplasm (cells can be mild, moderate, or severe atypical) Mucinous cystic neoplasm (cells can be mild, moderate and severe atypical)
well-differentiated solid neuroendocrine tumors–pseudopapillary tumors
VVV =”font-family:imitation-song”>Suspicious malignancy
VI VI VI =”font-family:imitation-song”>Malignant
Ductal adenocarcinoma
High-grade (G3) neuroendocrine carcinoma adenoidal cell carcinoma
Pancreaticoblastoma lymphoma
 Secondary tumors
Secondary tumors
Appendix 4: General description of pancreatic cancer specimens seen in general
Pancreatic duodenum

 Pancreaticoduodenectomy specimen, distal stomach, greater curvature length cm, lesser curvature length cm, duodenum length < span style="text-decoration:underline"> cm, circumference cm, common bile duct length cm, circumference cm, pancreas size–×–×– cm, in (duodenal papilla/inferior aspect of common bile duct/ (head of pancreas) see (description of appearance) mass, size –×–×– cm, cut surface properties; depth of infiltration (duodenal papilla >/infiltration of the lower bile duct) to . Involvement/ of other organs adjacent to the swelling is not involved. The mucosa of the intestinal canal next to or around the mass/is seen within the muscle wall (polyps/adenoma/ulcerative colitis/required negative visualization), gastric wall visualization (required negative visualization), pancreatic visualization (required negative visualization). (necessary). Duodenal, gastric, common bile duct, pancreatic dissection, and retroperitoneal margins (labeled or sent clinically alone) . Lymph nodes were found in the greater curvature (number/many/more than ten/ (dozens of) pieces, diameter to cm; small curved found lymph nodes
Pancreaticoduodenectomy specimen, distal stomach, greater curvature length cm, lesser curvature length cm, duodenum length < span style="text-decoration:underline"> cm, circumference cm, common bile duct length cm, circumference cm, pancreas size–×–×– cm, in (duodenal papilla/inferior aspect of common bile duct/ (head of pancreas) see (description of appearance) mass, size –×–×– cm, cut surface properties; depth of infiltration (duodenal papilla >/infiltration of the lower bile duct) to . Involvement/ of other organs adjacent to the swelling is not involved. The mucosa of the intestinal canal next to or around the mass/is seen within the muscle wall (polyps/adenoma/ulcerative colitis/required negative visualization), gastric wall visualization (required negative visualization), pancreatic visualization (required negative visualization). (necessary). Duodenal, gastric, common bile duct, pancreatic dissection, and retroperitoneal margins (labeled or sent clinically alone) . Lymph nodes were found in the greater curvature (number/many/more than ten/ (dozens of) pieces, diameter to cm; small curved found lymph nodes
(number/more/more than ten/ (several dozen), with diameters to cm. Lymph nodes were found in the intestinal wall (number
/More/than ten///dozens), with a diameter of
to
cm; mesenteric found lymph nodes (number/ more/more than ten/dozens), with a diameter of
to
cm; peripancreatic lymph nodes were found (number/more/more than ten/dozens), with a diameter of
to
cm.
Annex 5: Routine description of pancreatic cancer as seen microscopically
1. Tumor.
- style=”margin-left: 95pt”>
- Tissue staging.
- Tissue grading.
- Dip and range.
- Vascular infiltration.
- style=”margin-left: 43pt”>
-
Perineural infiltrates. 2. Cut margins.
- style=”margin-left: 40pt”>
- Distal pancreas.
- Common bile duct.
- Proximal (stomach).
- Distal pancreas.
-
distal (duodenum). 3. Other pathology seen.
- style=”margin-left: 40pt”>
- Chronic pancreatitis.
- Atypical hyperplasia.
- Chemical growth.
- Other.
- Chronic pancreatitis.
4. Regional lymph nodes (including gastric, duodenal, parapancreatic and separately sent lymph nodes).
- style=”margin-left: 83pt”>
- Total.
- style=”margin-left: 43pt”>
-
Number of involved. 5. Distant metastases.
- Other tissues/organs.
- Other tissues/organs.
- Special ancillary findings (histochemical staining, immunohistochemical staining, etc.).
-
Difficult pathologies are referred to higher level hospitals for consultation (provide original pathology report to verify the correctness of the sent sections, reduce errors, provide adequate lesion sections or wax blocks, and what was seen intraoperatively, etc.).
Annex 6: Histologic Classification of Pancreatic Tumors (WHO 2019)
Benign epithelial tumors and precursor lesions
8441/0 Plasmacytoid cystadenoma, non-specific Oligocystic plasmacytoid cystadenoma
Solid plasmacytoid adenoma
Mixed plasmacytoma associated with cerebral retinal angiomatosis–endocrine tumors
8441/3 Plasmacytoid cystic adenocarcinoma, non-specific
8148/0 Pancreatic intraepithelial neoplasia, low grade
8148/2 Pancreatic intraepithelial neoplasia, high grade
8453/0 Intraductal papillary mucinous neoplasm with low-grade heterogeneous hyperplasia
8453/2 Intraductal papillary mucinous neoplasm with high-grade heterogeneous hyperplasia
8453/3 Intraductal papillary mucinous neoplasm with infiltrative carcinoma
8455/2 Ductal eosinophilic papillary neoplasm Non-specific type
8455/3 Ductal eosinophilic papillary neoplasm with invasive carcinoma
8503/2 Intraductal tubular papillary neoplasm
8503/3 Intraductal ductal papillary neoplasm with invasive carcinoma
8470/0 Mucinous cystic neoplasm with low-grade heterogeneous hyperplasia
8470/2 Mucinous cystic neoplasm with high-grade heterogeneous hyperplasia
8470/3 Mucinous cystic neoplasm with infiltrative carcinoma Malignant epithelial neoplasm.
8500/3 Ductal adenocarcinoma,Non-specific
8480/3 Glial carcinoma
8490/3 Low-adherent carcinoma
8490/3 Indolent cell carcinoma
8510/3 Medullary carcinoma, non-specific type
8560/3 Adenosquamous carcinoma
8576/3 Hepatocellular carcinoma
8014/3 Large cell carcinoma with transverse myeloid phenotype
8020/3 Undifferentiated carcinoma,Non-specific
8035/3 Undifferentiated carcinoma with osteoblastic giant cells
8550/3 Adenosquamous cell carcinoma
8551/3 Adenocarcinoma of the blastocyst
8154/3 Mixed glandular blasts –Endocrine carcinoma
8154/3 Mixed glandular blasts –Endocrine–Ductal carcinoma
8552/3 Mixed glandular blasts –Ductal carcinoma
8971/3 Pancreaticoblastoma
8452/3 Pancreatic solid< span style="font-family:Times New Roman">–pseudopapillary tumor
Pancreatic solid–Pseudopapillary tumor with high-grade carcinoma pancreatic neuroendocrine tumor
8150/0 Pancreatic neuroendocrine microadenoma
8240/3 Pancreatic neuroendocrine tumor
8240/3 Neuroendocrine Tumors,G1
8249/3 Neuroendocrine tumors,G2
8249/3 Neuroendocrine Tumor,G3
8150/3 Neuroendocrine tumor of the pancreas, no Functional eosinophilic neuroendocrine tumor, no Functional pleomorphic neuroendocrine tumor, no Functional
Transparent cell neuroendocrine tumor, no Functional cystic neuroendocrine tumor, no Functional
Functional pancreatic neuroendocrine tumor
8241/3 Secretion < span style="font-family:imitation-song span style="font-family:Times New Roman">5-hydroxytryptamine tumors
8153/3 Gastrinoma
8152/3 Hyperglycemia
8151/3 Insulinoma
8156/3 Growth-inhibiting hormone tumor
5155/3 VIP tumor
8158/3 Adrenocorticotropin-secreting tumor
8241/3 Chromophobe carcinoid tumor of the intestine
8246/3 Neuroendocrine carcinoma
|
8041/3 |
small cell neuroendocrine carcinoma |
|
8013/3 |
Large cell neuroendocrine carcinoma |
|
8154/3 |
mixed neuroendocrine–non-neuroendocrine tumors |
|
8154/3 |
Mixed glandular blisters< span style="font-family:Times New Roman">–Endocrine Carcinoma |
8154/3 Mixed glandular blasts–Neuroendocrine carcinoma
8154/3 Mixed glandular blasts –Endocrine–Ductal carcinoma
Mature teratoma Mesenchymal tumor Malignant lymphoma Secondary tumor
Annex 7: Karnofsky score (KPS, percent method)


100 Normal health status, no complaints and no obvious objective signs and symptoms.
90 Normal activity with minor signs and symptoms.
80 Very barely able to perform normal activities with some symptoms or signs and symptoms.
70 Self-supporting, but unable to maintain a normal life or work.
60 Mostly able to take care of themselves, but occasionally need help and cannot do their normal work. Mostly able to take care of myself, but occasionally need help with normal tasks.
50 Mostly unable to care for themselves and need frequent treatment and care.
40 Living on their own and needing specialist treatment and care.
30 Complete loss of self-care, requiring hospitalization and Total loss of self-care requiring hospitalization and active supportive treatment.
20 Severe enough to require supportive care.
10 Dying, rapidly deteriorating and near death.
 0 Death.
0 Death.

Attachment 8: Zubrod-ECOG-WHO score (ZPS, 5-point scale)


- style=”margin-left: 66pt”>
- Normal activity.
- style=”margin-left: 66pt”>
- Mild symptoms, self-care, able to perform light physical activities.
- style=”margin-left: 69pt”>
- Tolerate the symptoms of tumor and live on their own, but not more than 50% of the time they are in bed during the day. Severe tumor symptoms with more than 50% of daytime bed rest, but still able to get up and stand, part
- Partly self-care.
- style=”margin-left: 66pt”>
- Seriously ill and bedridden.
- style=”margin-left: 66pt”>
- Death.

Annex 9: Criteria for resectable pancreatic cancer
resectable status Arterial Venous


Removable pancreatic cancer
Critical resectable pancreatic cancer
No Partial
Progressable
Cutting period
Excluding
Pancreatic cancer
 Combined distant metastases
Combined distant metastases
The tumor did not invade the celiac trunk, superior mesenteric artery, or common hepatic artery.
Tumors of the head and neck of the pancreas.
Tumors invading the common hepatic artery but not involving the abdominal trunk or left and right hepatic artery initiation, can be completely resected and reconstructed; the tumor invades the superior mesenteric artery but does not exceed 180 degrees; if a variant artery is present anatomy
(e.g., collateral right hepatic artery, alternative right hepatic artery, alternative common hepatic artery and alternative or collateral arteries of origin), care should be taken to clarify whether tumor invasion and the extent of invasion may influence surgical decisions.
PancreasCaudal tumors.
Tumor invades the abdominal trunk without exceeding 180 degrees; tumor invasion of the abdominal trunk exceeds 180 180 degrees. span>degree, but without invasion of the abdominal aorta and with the gastroduodenal artery intact and uninvaded.
Tumors of the head and neck of the pancreas.
Tumor invading superior mesenteric artery more than180 degrees; tumor invading the celiac trunk more than 180 degrees; tumor invades the first jejunal branch of the superior mesenteric artery.
PancreasCaudal tumors.
Tumor invading superior mesenteric artery or celiac trunk more than
180180 span>degree; tumor invades the abdominal trunk and abdominal aorta. Distant metastases (including non-regional lymph node metastases).
Tumor does not invade the superior mesenteric vein and portal vein, or invades but does not exceed 180degrees, and the vein contour is regular.
 < span style="font-family:imitation-song; font-size:12pt">Tumors of the head and neck of the pancreas.
< span style="font-family:imitation-song; font-size:12pt">Tumors of the head and neck of the pancreas.
Tumor invading the superior mesenteric vein or portal vein beyond 180 degrees or invasion although not exceeding
180degree, but there is venous contour irregularity; or there is venous thrombosis, which allows for safe venous reconstruction after resection; the tumor touches the inferior vena cava.
 < span style="font-size:12pt">胰体/Caudal tumors.
< span style="font-size:12pt">胰体/Caudal tumors.
 Tumor invasion of splenic vein portal venous confluence, or invasion of the left side of the portal vein does not exceed 180 degree, but there is venous contour irregularity; and there are suitable proximal or distal vessels available for safe and complete resection and venous reconstruction; and the tumor touches the inferior vena cava. Tumors of the head and neck of the pancreas.
Tumor invasion of splenic vein portal venous confluence, or invasion of the left side of the portal vein does not exceed 180 degree, but there is venous contour irregularity; and there are suitable proximal or distal vessels available for safe and complete resection and venous reconstruction; and the tumor touches the inferior vena cava. Tumors of the head and neck of the pancreas.
Tumor invasion or embolization (tumor thrombus or thrombus) resulting in non-resectable reconstruction of the superior mesenteric vein or portal vein.
 The tumor invades most of the proximal jejunal draining branches of the superior mesenteric vein.
The tumor invades most of the proximal jejunal draining branches of the superior mesenteric vein.
Pancreas/Caudal tumors.
 Tumor invasion or embolization (possibly tumor embolus or thrombus) leading to unresectable reconstruction of the superior mesenteric vein or portal vein.
Tumor invasion or embolization (possibly tumor embolus or thrombus) leading to unresectable reconstruction of the superior mesenteric vein or portal vein.
Distant metastases (including non-regional lymph node metastases).
Annex 10: WHO criteria for evaluating the efficacy of solid tumors
- style=”margin-left: 55pt”>
- Complete remission: complete disappearance of tumor beyond 1 month.
- Partial remission: reduction of the product of the maximum tumor diameter and the maximum vertical diameter by up to “font-family:Times New Roman”>50%, with no increase in other lesions that persist beyond 1 . span>months.
-
Stable lesion: the product of the two diameters of the lesion is reduced by no more than 50%, enlargement not more than 25% for more than 1 month.
- style=”margin-left: 44pt”>
- Progression of the lesion: the product of the two diameters of the lesion increases by more than 25%.
- Progression of the lesion: the product of the two diameters of the lesion increases by more than 25%.
Annex 11: RECIST Efficacy Evaluation Criteria
Evaluation of target lesions
Complete remission: all target lesions disappeared.
Partial remission: the sum of the longest diameter of the target lesions is reduced compared to the baseline status by at least 30%.
Lesion progression: increase in the sum of the longest diameter of the target lesion compared to the sum of the longest diameter of the smallest target lesion recorded after the start of treatment 20%, or the appearance of one or more new lesions.
Stable lesions: between partial remission and disease progression. Evaluation of non-target lesions
Complete remission: disappearance of all non-target lesions and return of tumor markers to normal. Incomplete remission/Stable: presence of one or more non-target lesions and/or
persistent above-normal tumor markers.
Progression of lesion(s): One or more new lesions and/or definite progression of existing non-target lesions.
Evaluation of best overall outcome
The evaluation of best overall outcome is the smallest value measured between the start of treatment and disease progression or relapse. Typically, the classification of a patient’s best outcome consists of focal measurement and confirmation.
Annex 12: Flowchart of the role of ERCP in the diagnosis and treatment of pancreatic cancer
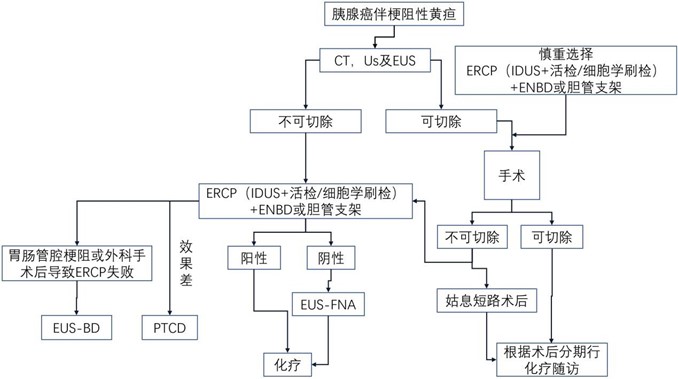
 Attachment 13: Pancreatic Cancer Treatment Flow
Attachment 13: Pancreatic Cancer Treatment Flow
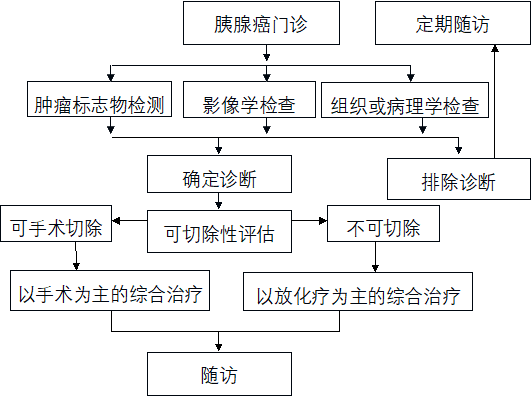
Annex 14: Clinical staging system for postoperative bleeding
|
Grading |
“border-top: solid black 0.5pt; border-left: none; border-bottom: solid black 0.5pt; border-right: solid black 0.5pt”>
Time, location, severity, and clinical aspects of bleeding Impact |
Clinical situation |
Diagnosis |
Treatment results |
|
A |
early, in the abdominal cavity or in the digestive tract. Mild |
good |
Observation, blood work, ultrasound if necessary CT |
< span style="font-family:Arial; font-size:12pt">none |
|
B |
Early stage, intra-abdominal or intra-digestive tract, severe. Late, intra-abdominal or elimination Intra-abdominal, mild |
Usually good or moderate, rarely life-threatening |
observation, blood count, ultrasound,CT, angiography, endoscopy |
Blood Transfusion/Transfusion, Intensive Care, Endoscopic Hemostasis, Vascular Embolization, Early Bleeding Cesarean section |
|
C |
Advanced, intra-abdominal or intra-digestive, severe |
severe damage, life-threatening < /td> |
Hematography. CT, endoscopy |
Define the location of the bleeding, angiography and embolization, endoscopic hemostasis, cesarean Exploration for hemostasis, critical |
Attachment 15
Pancreatic Cancer Guidelines (2022 Edition) Development and Validation Expert Group
(in order of surname stroke)
Team leader: Zhao Yupei Vice team leader: Wang Chengfeng
Members: Wang Liwei, Ba Yi, Shi Susheng, Cong Minghua, Liu Jun, Liu Rong, Liu Xuebao, Tang Zhaohui, Du Chunxia, Li Shengping, Li Jiangtao, Li Yexiong, Li Shu, Yang Yinmer, Yang Zhiying, Yang Lin, Yang Liu, Zhang Taiping, Zhang Jianwei, Chen Rufus, Lin Dongmei, Ouyang Han, Jin Gang, Zhao Xinming, Zhao Haiping, Hao Jihui Qin Renyi, Yuan Yufeng, Peng Li, Peng Bing, Jiang Kui Rong, Fu Deliang, Dai Guanghai, Dai Menghua
Secretary: Zhang Jianwei