A 42-year-old woman had an incidental finding of a left breast mass for 6 months, which was approximately 1 cm in diameter at the time of discovery. The mass was about 1 cm in diameter at the time of discovery. Since 1 month ago, the mass has increased significantly. The woman did not have any breast or ovarian cancer in her family, and had a hysterectomy for “fibroids” (without removal of the ovaries).
What happened next?
Imaging strongly suggests breast cancer
On breast examination by the breast specialist, a mass measuring approximately 1.5 cm x 1.5 cm was palpated in the upper outer left breast, which was hard, with less well-defined borders, and the mass was not very pushable. The breast was symmetrical, the nipple was not sunken or overflowing, and the skin of the breast was not red, swollen, or hot. The doctor also did not find clear enlarged lymph nodes in the axillae and clavicles bilaterally.
Further breast ultrasound showed a solid nodule in the upper left outer breast, Breast Imaging Reporting and Data System (BI-RADS) grade 4C-5, and a nodule visible in the left axilla. Mammography (X-ray) revealed a nodule in the left breast consistent with breast cancer, and no clear enlarged lymph nodes were seen in the bilateral axillae. Breast magnetic resonance imaging (MRI) also suspected breast cancer.
Cancer cells were seen on cytology after undergoing a puncture biopsy, suggesting breast cancer.
Imaging findings are important in suggesting the diagnosis. According to the BI-RADS grading, the higher the number, the greater the probability that the mass is malignant, with grade 4C indicating a high probability that the tumor is malignant, with a probability of >50% but <95% malignancy, and grade 5 with a higher probability of >95% malignancy.

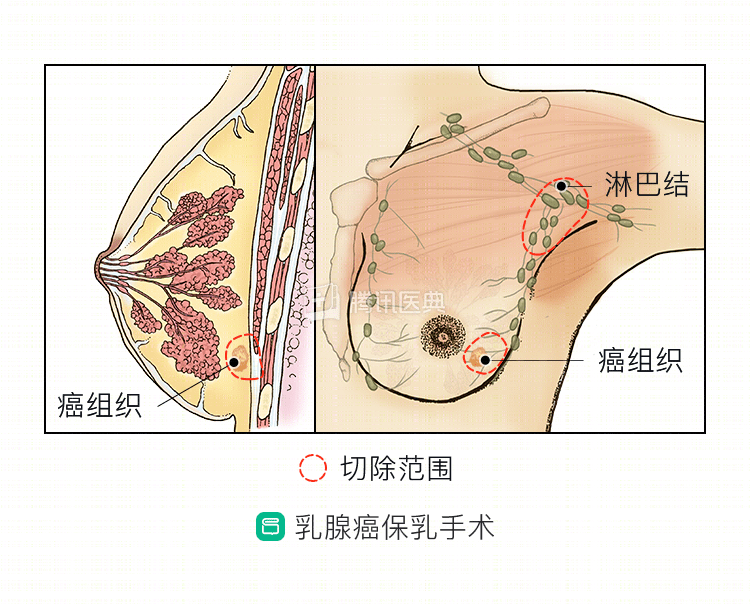
Milk-conserving surgery may also be followed by non-chemotherapy
In this woman, the imaging suggested a high probability of malignancy, but given the small size of the mass, which was about 1.5 cm in diameter, and the fact that it was a solitary lesion, it was predicted to maintain good breast shape after breast-conserving surgery and was consistent with the indication for breast-conserving surgery, so the surgeon considered breast-conserving surgery as a first step.
So, after completing the relevant blood and imaging tests and ruling out contraindications to surgery, the surgeon fully communicated with the patient and her family and developed the following surgical plan: breast-conserving surgery first, while evaluating for metastases in the sentinel lymph nodes and performing a total mastectomy if intraoperative cryopathology suggests that breast-conserving surgery is not indicated, or axillary lymph node dissection if metastases are found in the sentinel lymph nodes.
The final breast-conserving surgery was successful. The postoperative pathology was: invasive carcinoma of the left breast, non-specific grade II, no metastatic carcinoma in the anterior lymph nodes, and pTNM staging of pT1N0(sn). Immunohistochemical results showed estrogen receptor (ER) (80% strongly positive), progesterone receptor (PR) (30% moderately positive), human epidermal growth factor receptor-2 (HER-2) (+), and cell proliferation index Ki-67 (10%).
After breast-conserving surgery, adjuvant radiotherapy is usually required to reduce the local recurrence rate of the breast. Several large studies have demonstrated that patients with early-stage breast cancer treated with breast-conserving therapy in combination with radiotherapy have similar survival and odds of developing distant metastases compared with patients treated with total mastectomy.
The woman’s postoperative pathology suggested invasive breast cancer with early stage breast cancer and no high risk factors for tumor recurrence (high risk factors include younger age at presentation, larger tumor, vascular tumor embolism, nerve invasion, lymph node metastasis, etc.), so she could be treated postoperatively without adjuvant chemotherapy. Since immunohistochemistry suggests that her breast cancer is hormone receptor positive, i.e., ER (80% strongly positive) and PR (30% moderately positive), hormone receptors are the targets of endocrine therapy, and endocrine therapy can help reduce the risk of breast cancer recurrence and new contralateral breast cancer.
Based on these considerations, this woman received adjuvant radiation therapy after breast-conserving surgery and endocrine therapy with tamoxifen for 5 years.
Summary: Patients with early-stage breast cancer who meet the indications for breast-conserving surgery may not undergo postoperative adjuvant chemotherapy after successful breast-conserving surgery if there are no high-risk factors for recurrence, but radiation therapy is required after breast-conserving surgery, and, if hormone receptor-positive, endocrine therapy can help reduce the risk of tumor recurrence.