A 41-year-old woman who had a mammogram (X-ray) at her physical exam found tiny calcifications in her right breast, but she did not feel any significant mass in her breast and had no family history of breast or ovarian cancer. What should I do next?
No palpable mass but abnormal mammogram may also be cancer
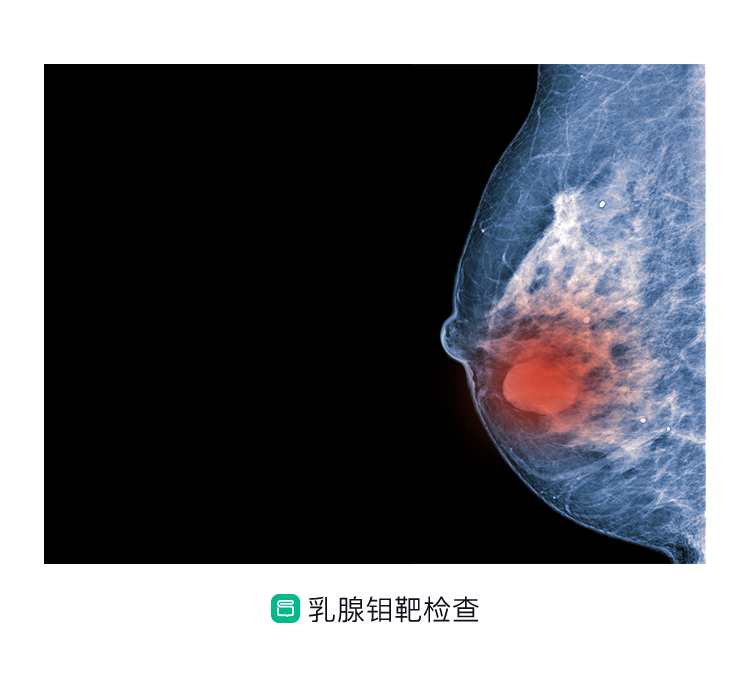
There are suspicious small calcifications in the lower part of the right breast found by mammogram only during physical examination. The mammogram is highly suspicious of malignancy and surgery is recommended. The breast specialist felt only a lamellar thickened area in the lower part of the right breast, measuring approximately 3 cm × 4 cm, but no obvious swelling was palpable and no abnormality was observed in the breast, and no definite enlarged lymph nodes were felt in the bilateral axillae or on the collarbone.
Further mammography revealed segmental distribution of small polymorphic calcifications in the lower part of the right breast, with no definite masses detected, and was considered malignant, BI-RADS grade 4C. The mammogram also revealed an area of structural disorganization in the lower right external breast, with a BI-RADS grade 4.
Although no obvious mass was palpated on breast examination, imaging still revealed abnormalities and suggested a high likelihood of breast malignancy. The numbers in the BI-RADS grading are suggestive; the higher the number, the greater the probability that the mass is malignant, and a grade 4 means that the tumor is suspicious for malignancy and needs to be improved. The mammogram is very good at detecting calcifications. Breast cancers sometimes appear as dense clusters of small calcified spots, especially in intraductal cancers, which is an advantage of the mammogram.
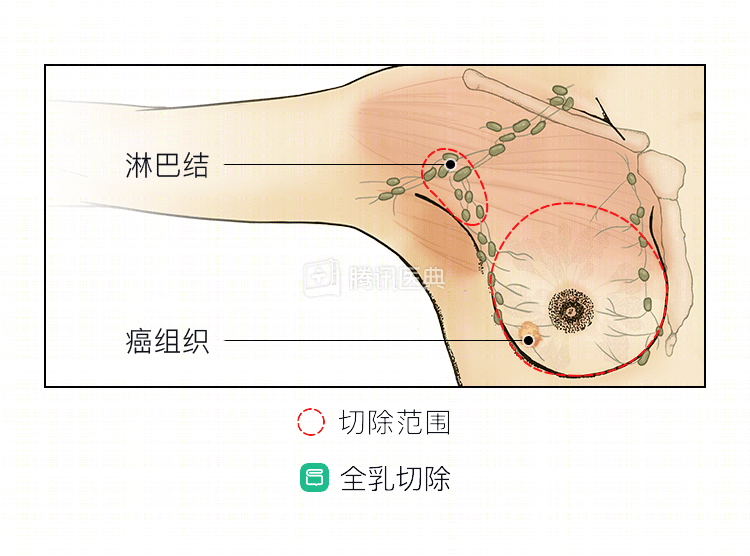
Why a total mastectomy?
This woman had suspicious calcifications suggested by mammogram, and the surgeon was not able to palpate a definite mass, so a preoperative puncture biopsy could not be performed to clarify the diagnosis, and direct surgical excision had to be performed. Combined with the ultrasound findings of the breast, the doctor recommended a total mastectomy if the intraoperative pathology confirmed a malignant lesion in order to ensure the integrity of the surgically resected tumor, considering the woman’s extensive lesion. Since imaging did not reveal any lymph node metastasis in the right axilla, from the perspective of improving quality of life and to avoid complications such as upper limb edema that may be associated with axillary lymph node dissection surgery, the doctor considered that an anterior sentinel lymph node biopsy could be performed first.
Based on these considerations, the surgeon, after thorough communication with the patient and family, developed the following surgical plan: local excision of the calcified foci, total mastectomy if intraoperative cryopathology suggests malignancy, and evaluation of the status of the sentinel lymph nodes and axillary lymph node dissection if metastases are found in the sentinel lymph nodes.
After resection of the calcified foci in the right breast, frozen pathology confirmed that the calcified foci in the right breast were cancerous, so simple excision of the right breast cancer + sentinel lymph node biopsy was performed, and no metastasis was found in the sentinel lymph nodes.
Why don’t you need adjuvant therapy after surgery?
Postoperative pathology showed high-grade ductal carcinoma in situ of the breast with a multifocal distribution, no metastatic carcinoma in the anterior lymph nodes, and pTNM staging of pTisN0(sn). Immunohistochemical results showed estrogen receptor (ER) (-), progesterone receptor (PR) (-), human epidermal growth factor receptor-2 (HER-2) (++), and cell proliferation index Ki-67 (20%).
As postoperative pathology confirmed ductal carcinoma in situ, adjuvant chemotherapy was not required for this type of breast cancer. Immunohistochemistry was negative for hormone receptors, i.e., ER(-), PR(-), and hormone receptors are the target of endocrine therapy; therefore, postoperative adjuvant endocrine therapy is also not required for those lacking this target. In summary, the woman has undergone total mastectomy with no metastasis in the anterior sentinel lymph nodes. Combined with the postoperative pathology and immunohistochemical findings, no postoperative adjuvant therapy is required, and the physician recommends periodic review.
Summary: For ductal carcinoma in situ with diffuse lesions that cannot be palpated as obvious masses and only abnormal imaging findings, only surgical excision of the lesion and diagnosis by pathology is possible, and total breast excision is recommended to ensure complete excision. The patient’s ductal carcinoma in situ itself does not require postoperative adjuvant chemotherapy, and if it is also hormone receptor negative, it does not require postoperative adjuvant endocrine therapy, but regular postoperative review is required.