
The goal of treatment for stage I and II breast cancer is to cure as much as possible, usually requiring surgery, and may experience the following treatments.
Preoperative treatment
For resectable breast cancer, preoperative systemic therapy is not necessary. If the mass is large but you still want to pursue breast-conserving treatment, you may need to first undergo preoperative antitumor medication with the goal of shrinking the tumor and lowering the stage in order to pursue breast-conserving surgery.
Preoperative chemotherapy, targeted therapy (for HER-2 positive breast cancer) and endocrine therapy (for those who are older, cannot tolerate chemotherapy, and have positive estrogen and progesterone receptors) are called neoadjuvant therapy, and it is the same as the adjuvant regimen given postoperatively, except that it is chosen to be given preoperatively in time.
Surgery
Breast-conserving surgery
Breast-conserving surgery may be considered at the time of initial evaluation or after receiving preoperative neoadjuvant therapy if the requirements for breast-conserving surgery are met. Breast-conserving surgery removes only the tumor and some of the tissue surrounding the tumor, and is usually followed by radiation therapy. Studies have shown that those who undergo breast-conserving surgery combined with postoperative radiation therapy have similar long-term survival rates to those who undergo total mastectomy.
Mastectomy
Modified radical mastectomy for breast cancer is now usually performed by removing the affected breast and axillary lymph nodes, but preserving the pectoral muscle.
Armpit lymph node management
Breast cancer surgery also includes the removal and examination of axillary lymph nodes to further confirm breast cancer staging and determine whether the cancer has spread outside the breast, usually in one of two ways, both of which have been shown in studies to be similarly effective.
- For axillary lymph node dissection (ALND), the surgeon typically removes at least 10 axillary lymph nodes.
- Sentinel lymph node biopsy (SLNB), a method of evaluating whether the cancer has spread to the lymph nodes, has the advantage of removing only a small number of lymph nodes called the sentinel lymph nodes and is a less invasive procedure. If the test is negative (no cancer cells in the lymph nodes), axillary lymph node dissection may not be performed.
Mastopexy
Doctors often discuss breast reconstruction if undergoing a total mastectomy. The main types of surgery in terms of timing are immediate breast reconstruction and delayed breast reconstruction, which is performed either at the same time as the total mastectomy or months or years after the surgery.
Post-operative treatment
Postoperative local radiotherapy
After breast-conserving surgery, postoperative radiation therapy is usually required to destroy any local cancer cells that may remain and to reduce the recurrence rate. The surgeon will determine whether radiotherapy is needed and the extent and modality of radiotherapy based on tumor size, axillary lymph nodes and surgical margin pathology.
Postoperative systemic Adjuvant therapy
Post-operative systemic adjuvant therapy (including chemotherapy, endocrine therapy, and targeted therapy) may be required to eliminate cancer cells that may remain in the blood and throughout the body that are not detectable by current technology in order to reduce recurrence.
Adjuvant treatment options are determined based on the following factors: age, tumor size, lymph node metastasis, tumor type, surgical approach, tumor pathologic grade, tumor thrombus in lymphatic vessels and blood vessels, estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor-2 (HER-2), tumor cell proliferation index (Ki-67), and molecular typing of breast cancer.
If neoadjuvant chemotherapy is administered preoperatively and the course of chemotherapy is not completed, the physician will generally continue to complete the original planned chemotherapy regimen if the original regimen is effective; if the original regimen is not effective, the physician may choose to change the chemotherapy regimen after a thorough evaluation of the molecular typing of the tumor and the risk of recurrence. Chemotherapy is usually administered by intravenous infusion. During the treatment cycle, the drug is usually given for 1 to 2 days and then rested for several days.
People who are estrogen and/or progesterone receptor positive typically require 5 to 10 years of endocrine therapy. Physicians will usually determine the endocrine treatment plan based on menopausal status.
HER-2 positive individuals may need to receive 1 year of targeted drug therapy.
Chemotherapy is usually started within 1 month after surgery (no later than 2 months) depending on recovery. The order of postoperative treatment is chemotherapy first, and HER-2 positive individuals are usually treated with targeted therapy such as trastuzumab after completion of chemotherapy or chemotherapy and targeted therapy are started at the same time. If needed, radiotherapy can be started within 2 to 4 weeks after chemotherapy, and radiotherapy is usually started no more than six months before surgery. Endocrine therapy can be started when targeted therapy is started, when radiation therapy is started, or after radiation therapy is completed. Not all of these treatments may be administered, and the physician will choose based on the specific condition.
Follow-up
Follow-up visits may occur 1 to 4 times a year for the first 5 years after surgery, with follow-ups every 3 months in years 1 to 2 and every 6 months in years 3 to 5, depending on the condition. Follow-up visits may include laboratory tests, mammograms, ultrasounds, chest x-rays, and other imaging tests, and usually physical examinations, gynecologic examinations, and possibly bone density tests for those taking oral aromatase inhibitors.
For a good outcome, you should also maintain a healthy lifestyle, such as exercising properly, eating a healthy diet, limiting alcohol consumption, and maintaining an ideal weight.
The exact course of treatment for breast cancer is influenced by factors such as the disease, systemic status, risks of treatment, and the experience of the doctor, and the actual treatment requires the advice and recommendations of the doctor.
Summary
- The goal of treatment for resectable breast cancer is to cure it as much as possible.
- Doctors often use multimodal treatment, which may include surgery, radiation therapy, chemotherapy, targeted therapy (for those who are HER-2 positive), and endocrine therapy (for those who are estrogen and progesterone receptor positive).
- Surgery is the basic treatment, with the remaining treatments as adjuvant therapy.
- Post-operative follow-up as required, adherence to treatment, and maintenance of a healthy lifestyle are conducive to a good outcome.
Stage I Stage II Stage II Breast Cancer Treatment Flow Chart
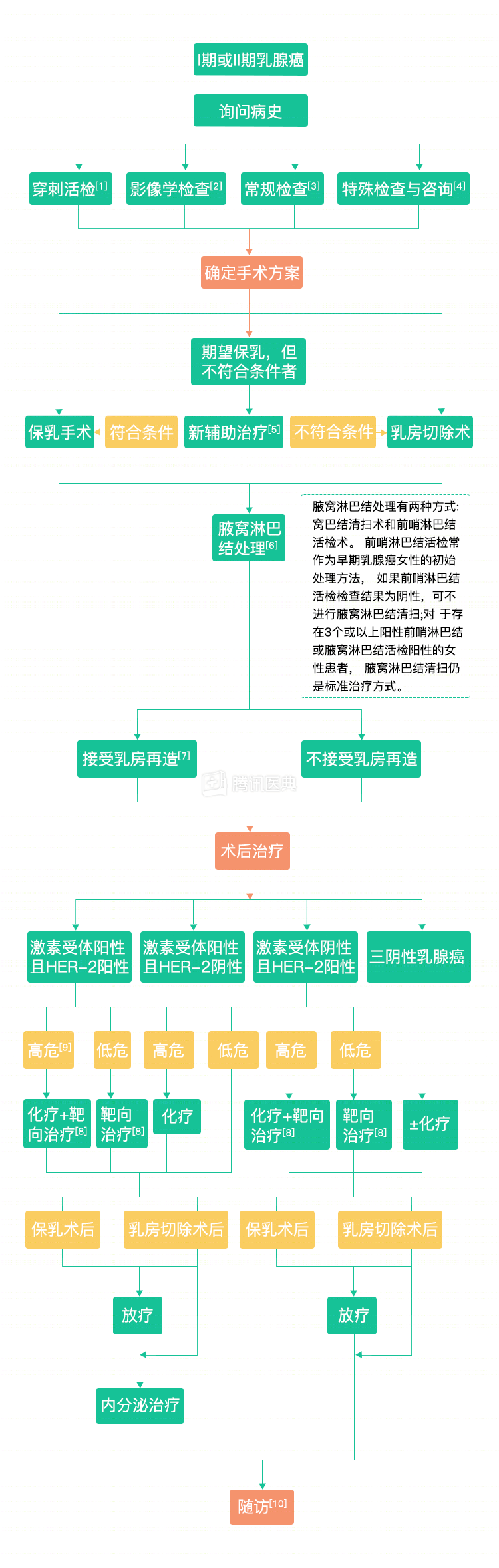
Notes:
- Puncture biopsy: The purpose of the biopsy is to obtain a tumor tissue specimen and perform biomarker testing for estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor-2 (HER-2) to assist in the development of a treatment plan.
- Imaging: imaging of the chest and abdomen (radiographs, ultrasound, CT, magnetic resonance imaging, etc.), bone scan (PET-CT may also be performed as an option).
- Routine examination: physical examination, routine blood count, blood biochemistry.
- Special tests and consultations: genetic counseling, fertility counseling.
- Neoadjuvant therapy: If the mass is large but you want to pursue breast-conserving treatment, you may need to first undergo preoperative antitumor drug therapy with the aim of shrinking the tumor and reducing the stage for breast conservation. Neoadjuvant therapy includes chemotherapy, targeted therapy (for those who are HER-2 positive) and endocrine therapy (for those who are older, cannot tolerate chemotherapy, and are estrogen receptor positive), and it is the same adjuvant regimen that is administered postoperatively, except that the timing is chosen to occur preoperatively.
- Armpit lymph node management: Breast cancer surgery also includes removal and examination of the axillary lymph nodes to further confirm breast cancer staging and to determine whether the cancer has spread outside the breast.
- Breast reconstruction: The procedure can be primarily divided in terms of timing into immediate breast reconstruction and deferred breast reconstruction, which is performed either at the same time as total mastectomy or months or years after surgery.
- Targeted therapy: Targeted therapy is usually required for HER-2 positive patients; it is still controversial whether HER-2 positive patients with stage T1a (tumor <0.5 cm) should receive targeted therapy.
- Physicians generally determine whether there is a high risk of recurrence based on lymph node metastasis, age, tumor size, tumor differentiation, HER-2 receptors, hormone receptors, etc.
- Follow-up: Depending on the situation, follow-up visits may be performed 1 to 4 times per year for the first 5 years after surgery, with reviews every 3 months in years 1 to 2 and every 6 months in years 3 to 5. Follow-up visits may include mammograms and other imaging, general physical examinations, gynecologic examinations, and bone density examinations.