About 40% of patients with advanced non-small-cell lung cancer (NSCLC) can detect a currently available drug “target” and receive targeted therapy with better efficacy and fewer side effects, but what if there is no “target”? target”, what happens?
At this point, emerging immunotherapies offer a glimmer of hope, traditional chemotherapy remains a reliable option, and a variety of new drug clinical trials are available for patients with advanced disease.
Here we focus on treatments other than targeted therapies.
Immunotherapy (PD-1/PD-L1 inhibitors)
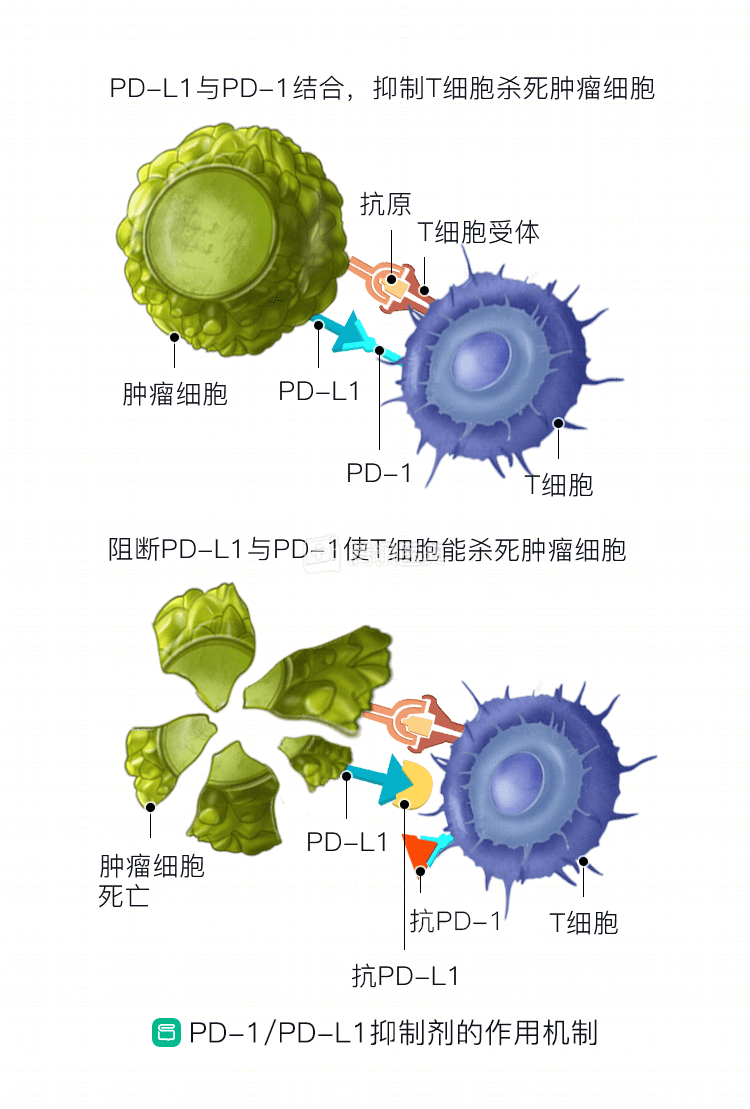
PD-1 and PD-L1 molecules are both “immune checkpoints.” PD-1 is located on the surface of T-lymphocytes, and when activated, it suppresses immune function, causing the lymphocytes to lose their “fighting power. When activated, PD-1 suppresses immune function, depriving lymphocytes of their “fighting power” and preventing them from effectively clearing tumors. PD-L1, which activates it, is located on the surface of cancer cells. Drugs that inhibit PD-1 or PD-L1 (immune checkpoint inhibitors) are currently the most widely used immunotherapy for lung cancer.
In patients who are not candidates for targeted therapy, the expression of PD-L1 on the surface of tumor cells can also help physicians predict outcomes.
PD-L1 expression ≥1%: pablizumab (trade name: Corexta, commonly known as “K drug”
)
A PD-1 inhibitor, pablizumab, can be the first-line treatment of choice as long as PD-L1 expression in tumor cells is found to be ≥1%.
Studies have demonstrated that patients with ≥50% PD-L1 expression have a 45% remission rate with pabolizumab alone (28% with chemotherapy), a median progression-free time of more than 10 months, significantly better than chemotherapy (4 months), and less adverse effects.
Further studies confirmed that pablizumab monotherapy was superior to chemotherapy in patients with PD-L1 expression of ≥1%. This means that patients without driver genes who have tumor tissue PD-L1 expression of ≥1% by pathology biopsy can be treated with pabolizumab.
PD-L1 expression<1%: Atezolizumab, or pabrolizumab + chemotherapy
PD-L1 expression<1% means a “cold tumor” that is “unresponsive” to immunotherapy, and pabrolizumab alone is difficult to achieve a favorable outcome. The combination of chemotherapy, however, can transform the tumor into a “hot tumor” that is sensitive to immunotherapy.
Different types of lung cancer have different drug choices:
- Squamous lung cancer: Pabrolizumab + chemotherapy (carboplatin + paclitaxel)
Pabrolizumab combined with chemotherapy (carboplatin + paclitaxel) as first-line treatment resulted in an overall survival time of more than 15.9 months in half of patients, 4.6 months longer than chemotherapy, a 36% reduction in the risk of death, and no significant increase in adverse events with the combination .
As of 2019 data, other immune drugs such as nabritumomab (trade name: Ondivolol) and Atezolizumab (trade name: Tecentriq) in combination with chemotherapy also achieved better outcomes than chemotherapy, but not as well as pabrolizumab.
- Non-squamous
- Non-squamous cancer: Atezolizumab + chemotherapy (platinum + pemetrexed)
Atezolizumab in combination with chemotherapy resulted in overall survival of more than 19 months and progression-free survival of more than 12.6 months in half of patients, almost double the length of chemotherapy. Combination chemotherapy with pabrolizumab or nabulizumab was also more effective than chemotherapy alone.
High tumor mutation load: combination immunotherapy
Some patients have a “high tumor mutational load. The “tumor mutational load” can be understood as the number of somatic mutations carried on the DNA of tumor cells, and the higher it is, the more antigens are likely to be recognized by the immune system and the stronger the immune response.
In patients with a “high tumor mutational load,” first-line therapy can be given with nabumetinumab alone, but it is more effective when combined with Ipilimumab (another class of immune checkpoint inhibitor), but it also has increased adverse effects.
“Back to the classics”-chemotherapy
Before the advent of immunotherapy, the “classic” option for patients with advanced lung cancer who could not use targeted drugs was chemotherapy. There are many chemotherapy regimens, and the choice depends on the type of lung cancer and the patient’s fitness status. The higher the PS score, the less fit the patient is, and the more “gentle” the chemotherapy regimen needs to be. The specific regimen is as follows:
| PS rating | Program | Drug composition | Duration of medication | Cycle |
| PS=0~1 | NP | Changchun Ruibin | Day 1,8 | 21-day cycle, typically 4 to 6 cycles |
| Cisplatin or carboplatin | Day 1 | |||
| GP | Gemcitabine | Day 1,8 | ||
| Cisplatin or carboplatin | Day 1 | |||
| DP | Docetaxel | Day 1 | ||
| Day 1 | ||||
| AP | Pemetrexed | Day 1 | ||
| Day 1 | ||||
| PCB | Paclitaxel + carboplatin + bevacizumab | Day 1 | ||
| PS=2 | Remove platinum, single agent regimen | Gicitabine/docetaxel/paclitaxel/vincristine/pemetrexed (non-squamous) | as before |